The Emergence of Sodium glucose Co-transporter 2 Inhibitors as a Successful Agent for Management of Diabetes Mellitus
Most of current guidelines for management of diabetes mellitus are recommending comprehensive strategy inclusive of adequate control of blood pressure and weight apart from hyperglycemia . Several innovative anti-diabetic molecules have been launched in recent years. Out of these agents, injectable incretin based therapy like GLP 1 receptor agonist has shown great promise, but high cost and injectable route of administration have prevented their wide acceptance. In the last 4 years, sodium glucose co-transporter inhibitor, which works in kidney to induce excess glucose elimination through urine, has been launched globally. This oral anti-diabetic agent works comprehensively and more intensively than existing dipeptyl peptidase 4 inhibitors (DPP4i). Apart from its’ excellent glycemic benefit with negligible risk of hypoglycemia, and extra-glycemic benefits like weight loss and blood pressure control, compatibility with almost all existing anti-diabetic agents, possible positive impact on cardiovascular and renal outcomes, and rapid reversal of glucotoxicity in type 2 diabetes mellitus patient whose renal function is intact, make them irresistible options for management of type 2 diabetes mellitus. However, despite huge advantages, injudicious ,use of agents this class throws up unique challenges like genito- urinary infections, eu-glycemic keto-acidosis, electrolyte imbalance etc.. This review tries to give a comprehensive and balanced view of this class of drug.
Introduction
Diabetes mellitus is a becoming a huge pharma co- economic burden globally due to its substantial impact on increase in mortality, morbidity, and quality of life. The number of adults with diabetes in the world increased from 108 million in 1980 to 422 million in 2014. The diabetes prevalence rate has increased from 4.3%to 9.0% in male and 5.0% to 7.9% in females during the period from 1980 to2014..The rate of increase in diabetes prevalence is faster in low and middle income countries than higher income countries during last three decades. Out of the top five countries contributing half of total global population of patients with diabetes, three are from South-East Asian region (China, India and Indonesia), with a continuous increasing trend [1, 2]. During the last three decades, several oral or injectable anti-diabetics molecules including some innovative ones like GLP 1 receptor agonist (GLP-1a), dipeptyl peptidase 4 inhibitors (DPP4i), newer generation of analogue insulin etc have evolved -and incorporated into the armamentarium of diabetes management [3, 4, 5]. Diabesity, a term used to describe obesity amongst persons with diabetes has evolved as a major issue for clinicians as well as epidemiologist during last few decades [6]. Since 2012 onwards, SGLT2 inhibitors have been launched globally in different countries. From clinical perspective, the medical fraternity needs to evaluate whether this class of molecule deserves a respectable place in the treatment armamentarium to fight diabetes [7].
SGLT2 Inhibitors – Mechanism of Action
Kidneys play an important role in glucose homeostasis in body. Every day, they produce 15-55 gm of glucose by gluconeogenes is while simultaneously utilizing 25 gm. Along with this, kidneys also reabsorb 180 gm of glucose per day at proximal convoluted tubules (PCT) [8]. This renal glucose reabsorption is happening mainly through SGLT 1 and SGLT2 co-transporters. Almost 90% of glucose re-absorption is by SGLT 2 co-transporter situated at S1 segment of PCT and rest 10% glucose re- absorption is by SGLT1 co-transporter situated at S3 segment of PCT (Figure1) [9].
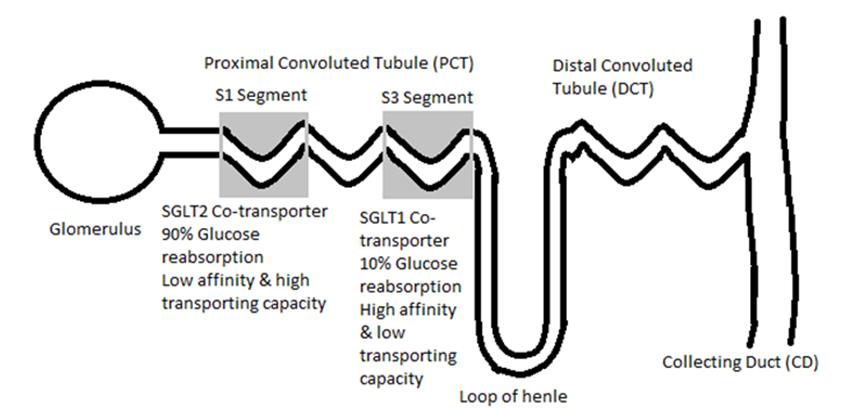
In type 2 diabetes mellitus (T2DM), over expression of SGLT2 and SGLT1 co-transporters lead to enhanced renal threshold for glucose upto ~250 mg/dl which in normal subject without diabetes is ~ 180 mg/dl (10, 11) SGLT2 inhibitors block reabsorption of glucose by SGLT2 co- transporter resulting in excretion of ~70 gm/day of in urine which is equivalent to approximately ~280 kcal/day. This is accompanied by a loss of ~400 ml of water per day due to osmotic dieresis [11, 12]. In addition to this, they improve pancreatic beta-cell function indirectly by reducing glucotoxicity, increase lipid oxidation in adipose tissues, increase endogenous glucose production in liver by stimulating pancreatic alpha cells to secrete glucagon, improve insulin sensitivity and glucose utilization in skeletal muscles. Thus SGLT2 inhibitors counterbalance multiple aspects of diabetes pathophysiology, except perhaps increase in endogenous glucose production [11].
Glycemic and Extra-Glycemic Benefit with SGLT2 Inhibitors
In the last 6 years, almost six SGLT inhibitors (canagliflozin, dapagliflozin, empagliflozin, tofogliflozin, lose ogliflozin, ipragliflozin) have been launched globally [13, 14, 15, 16, 17]. There is no head to head trial looking at comparative efficacy amongst different SGLT2 inhibitors. Most widely used SGLT2 inhibitors are canagliflozin, dapagliflozin and empagliflozin(not in any order). Few meta-analyses involving different agents within the class of SGLT2 inhibitors show can agliflozin300 mg as the most efficacious vs all others in terms of glycemic efficacy and extra-glycaemic benefit like weight loss but with higher incidences of adverse events such as genito- urinary infection (Table 1). On the other hand dapagliflozin10 mg and empagliflozin25 mg both show balance in terms of safety and efficacy as per meta- analysis within SGLT2 inhibitors class [18].
| Name of SGLT2inhibitor | HbA1c Changes (%) | Weight Reduction (in Kg) |
| Canagliflozin 300 mg | -0.9 CI (-1.0, -0.8) | -2.5 CI (-2.8, -2.1) |
| Canagliflozin 100 mg | -0.8 CI (-0.9, -0.7) | -1.9 CI (-2.2, -1.5) |
| Empagliflozin 25 mg | -0.7 CI (-0.8, -0.6) | -2.3 CI (-2.6, -1.9) |
| Dapagliflozin 10 mg | -0.7 CI (-0.7, -0.6) | -2.1 CI (-2.5, -1.8) |
| Empagliflozin 10 mg | -0.6 CI (-0.7, -0.5) | -2.2 CI (-2.5, -1.9) |
| Dapagliflozin 5 mg | -0.6 CI (-0.7, -0.4) | -1.6 CI (-2.0, -1.2) |
Table 1: Salient efficacy features of different SGLT2 inhibitors from multitudes of clinical trials.18 SGLT2: Sodium Glucose Tabl
The first decade of this millennium witnessed a paradigm shift in the approach to the management of T2DM with the advent of incretin based therapy, namely dipeptyl peptidase 4 inhibitors (DPP4i) and glucagon like polypeptide 1receptor agonist (GLP-1RA). DPP4i has seen wide acceptance globally as add on to metformin therapy, or even as accompaniment to insulin. But the same cannot be said about GLP-1a due probably to high cost especially in developing countries, inspite its’ potent glycemic as well as extra-glycemic benefit like weight loss which is an important component of comprehensive anti-diabetic management as suggested by many of current guidelines (Table 2) [26, 27, 28, 29, 30].
Japan have shown similar glycaemic and extra-glycaemic benefits [13, 14, 15].
SGLT2 Inhibitors and Incretin Therapy
| Glycaemic control | Weight (kg) | Blood pressure | ||
|---|---|---|---|---|
| HbA1c | BMI (Kg/sqm) | WC centimetre (inches) | mmHg | |
| WHO 200626 | <7.0% | <25 (M) <24 (F) | - | <130/80 |
| EASD-ESC 200727 | ≤6.5% | <25 (M) | <94 (<37) Male | <130/80 |
| EASD-ESC 200727 | ≤6.5% | <25 (M) | <80 (<32) Female | <130/80 |
| ADA 201228 | <7.0% | ≤25 (M) | - | <130/80 |
| ADA 201129 | ≤6.5% | - | - | <130/80 |
| CDA 200830 | ≤7.0% | <25 (M) | <102 (<40) Male | <130/80 |
| CDA 200830 | ≤7.0% | <25 (M) | <80 (<35) Female | <130/80 |
Table 2: Comprehensive anti-diabetic management suggested by guidelines.
Table 2: Comprehensive anti-diabetic management suggested by guidelines. HbA1c: Glycated haemoglobin; BMI: Body Table 2: Comprehensive anti-diabetic management suggested by guidelines. HbA1c: Glycated haemoglobin; BMI: Body Mass Index WHO: World Health Organization; EASD: European Association of Study in Diabetes; ESC: European Society of Cardiology; ADA: American Diabetes Association.
Comparison of results of meta-analysis of SGLT 2 inhibitors and DPP4i indicates superiority of SGLT2 inhibitors over DPP4i in terms of efficacy and extra- glycemic benefits with similar overall safety. Like incretin based therapy, SGLT2 inhibitors also protect against gluco-toxicity-induced apoptosis of pancreatic ß-cells which is remarkable [31, 32].
SGLT2 inhibitors: advantages
SGLT2 inhibitors work through insulin independent mode of action [33]. In addition to this, their efficacy also depends on serum glucose level, due to which chances of developing hypoglycaemia with their usage is negligible [34]. SGLT2 co-transporters are expressed also at alpha cells in pancreas and inhibition of this co-transporter leads to slight increase of serum glucagon level within physiological range that resulted into mild increase endogenous glucose production in liver [11, 35]. SGLT2 inhibitor can be used as1st line agent in mono-therapy in patients who cannot tolerate metformin. By and large this new class of drug has seen widespread use as an add on as second or even third line of anti-diabetic agent to metformin, sulphonyl urea, DPP4i, thiazolidinedione etc.SGLT2 inhibitor can be used as1st line agent in mono- therapy in patients who cannot tolerate metformin. It can be safely used concomitantly with insulin or GLP1a. Such flexibility and compatibility would go a long way in achieving comprehensive diabetes management outcome [33].
Certain challenges SGLT2 inhibitors – myths and reality
Every good thing may come with certain challenges and SGLT2 inhibitors are no exceptions. However it is important to delve deeply and take a holistic view in this regard.
Urinary Tract infection or Genital mycotic infection.
Patients with diabetes are at risk of developing bacterial or fungal infection. These infections are frequently associated with uncontrolled hyperglycaemia. Lower urinary tract infection (UTI), which is common in type 2 diabetes patients has been reported in up to 22% of such patients [36]. Infection risk is directly related to glycaemic status with the risk becoming approximately 2- fold greater (adjusted RR, 1.76; 95% CI, 1.30–2.38) for patients with HbA1c levels in the highest quintile despite on-going anti-hyperglycaemic therapy [37]. Apart from bacterial infections, mycotic infection in diabetes is quite common with uncontrolled hyperglycaemia. Risk of developing vulvo-vaginal infection is 81% greater in females with T2DM (adjusted relative risk [RR], 1.81; 95% CI, 1.64–2.00) [37]. Mycotic infections are definitely higher with the use of SGLT2 inhibitors, mainly because of glucosuria. However, most of such events are mild to moderate in intensity responding promptly to initial course of anti-fungal therapy and once uncontrolled hyperglycemia gets corrected, the rate of recurrence is less [38, 39].
Hyponatremia or Electrolyte Imbalance
Due to the unique mechanism of action, SGLT2 inhibitors blocks sodium glucose co-transporter 2 in proximal convoluted tubule in nephron preventing glucose and sodium (Na+) entry into the tubular epithelial cells. Apart from this SGLT pathway, there are several other pathways responsible for sodium reabsorption in nephron. For example, sodium -hydrogen anti-port system plays major role in sodium reabsorption. Although 60-70% of sodium reabsorption is happening through proximal convoluted tubule, just <5% of that would be mediated by the sodium glucose co-transporter SGLT2 (Figure 1) [40]. No wonder that in 13 placebo controlled trial involving Dapagliflozin, (phase 2b and 3), mean change of serum and potassium from baseline over 24 weeks in the Dapagliflozin arm was similar with the placebo arm [40, 41].
Diabetic Keto-Acidosis (DKA)
Risk of DKA in patients with type 2 diabetes on SGLT2 inhibitors is quite low, probably numbering less than one in 1000 to one in 10,000. [42] There are two types of diabetic keto-acidosis, one with significant hyperglycaemia, and another with euglycaemia or moderate hyperglycaemia (blood glucose<300 mg/dl). The later type is popularly known as eu-glycaemic diabetic keto-acidosis (eu-DKA). This can happen in a background of too less amount of insulin secretion leading to restriction in the usage of glucose as substrate to generate energy.T his triggers exaggerated breakdown of fat to produce free fatty acid to be utilised forketogenesis and finally to enter into process of energy production through Kreb’s cycle. Certain steps are critical to avoid DKA while prescribing SGLT2 inhibitors. If the patient is on insulin, the insulin dose can be reduced as per demand but should not be withdrawn totally. It is mainly for this reason, this new drug should not be prescribed in type 1 diabetes patient till enough clinical data showing its safety are available (Table3) [43].
| Dos | Don’ts |
| Reduce Fluid loss | Don’t use in acute illness |
| Encourage adequate rehydration | Don’t stop ongoing insulin totally |
| Encourage adequate carbohydrate intake | Don’t use in Type 1 diabetes mellitus |
| Stop SGLT2 inhibitors >48hours before surgery | |
| Be on alert for early signs and symptoms of DKA |
Table 3: Measures to prevent diabetes ketoacidosis (DKA) in SGLT2inhibitor treated patients.
Acute Kidney Injury (AKI)
In May 2016, FDA has come up with acute renal failure warning against canagliflozin and dapagliflozinbased on 101 cases reported at FDA adverse effect reporting system during the period from March 2013 to October 2015.These cases were out of 1.5 million SGLT2 inhibitor users. Out of these,73 cases were due to Canagliflozin and 28 cases due to dapagliflozin. No case was reported for empagliflozin. Such differential reporting is obviously due to the fact that in the US, canagliflozin was launched in March 2013 followed by dapagliflozinin January 2014 and empagliflozin in September 2014 [44, 45, 46, 47]. Of the 101 cases, 51 reported concomitant ACE inhibitor use, 26 reported concomitant diuretic uses, and 6 reported concomitant non-steroidal anti-inflammatory drug (NSAID) use. A prior history of chronic kidney disease was reported in 10 of the 101 cases. In some cases, dehydration or hypotension was reported [44]. Regarding renal safety with SGLT2 inhibitors, in phase 2b/3 trial, eGFR data is available with canagliflozin, dapagliflozinand empagliflozin. For canagliflozin, 2 years data, for empagliflozin1 year data and with capagliflozin both 2 and 4 years data of eGFR are available. In Empa- REG trial, 4 years eGFR data is available with empagliflozin. Cutting across all the trials with SGLT2 inhibitors, though there were initial drop of eGFR within 1-2 weeks of initiation of treatment, normalization in the subsequent weeks on continuous usage of the product was a general rule rather than exception [21, 48, 49, 50, 51].The drug safety communication stated that health care professionals should carefully consider certain factors, including state of dehydration; chronic kidney insufficiency; congestive heart failure; and concomitant medications such as diuretics, angiotensin-converting enzyme inhibitors(ACEI), angiotensin receptor blockers (ARBs), and nonsteroidal anti-inflammatory drugs (NSAIDs) [44]. Beyond these precautionary steps, these drugs are considered by and large safe from renal point of view.
Fracture
After anecdotal reports and some clinical trial data evaluation, in September 2015, USFDA enhanced the level of warning for canagliflozin indicating e increased risk of bone fractures, and added new information about decreased bone mineral density [52]. The occurrence of bone fractures was evaluated in nine pooled clinical trials with a mean duration of exposure to canagliflozin of 85 weeks. The incidence rates of adjudicated bone fractures were 1.1, 1.4, and 1.5 per 100 patient-years of exposure in the comparator (placebo or active), canagliflozin 100 mg, and canagliflozin 300 mg groups, respectively. Fractures were observed as early as 12 weeks after treatment initiation, and were more likely to be precipitated by low intensity trauma (e.g., arising after falls from no more than standing height) and affect the upper extremities [52]. There is no significant alteration of bone turnover markers or bone mineral density with dapagliflozin, in men as well as postmenopausal women with T2DM after 50 weeks and 102 weeks of follow-up [22, 53]. No increase in fractures was observed in pooled data from patients with normal to mildly impaired renal function across the dapagliflozin clinical studies [44]. Fracture incidence was comparable in both empagliflozin and placebo arm (3.9% vs 3.8%) in phase 2b/3 f trials [47]. Overall, incidence of fracture is about 3 per 1000 patients treated with SGLT2 inhibitors [46, 51, 54].
Hypovolemia or Dehydration
SGLT2 inhibitor works as osmotic diuretic and due to its mechanism of action there could be fluid loss of ~400 ml/day which is roughly equivalent to just one extra void of urine. This urine output is spread throughout the day, and does not cause nocturia [11]. However, in climatic condition of tropical countries like the Indian subcontinent, especially in the background of excessive heat exhaustion, this may present realistic health challenges such as drug induced hypovolemia and electrolyte imbalance. Counseling must include advice to maintain adequate fluid and electrolyte intake, and awareness about symptoms of dyselectrolytemia. One
should also ensure that SGLT2 inhibitors are not co- prescribed with loop diuretics. However, there is no need to monitor serum electrolytes or renal function tests in persons on long termSGLT2 inhibitors treatment [55]. Safety and efficacy are important considerations during selection of any molecule, and if these are important than even a pioneer molecule like metformin is also having safety issue like lactic acidosis, sulphonylurea is having issues like hypoglycaemia, weight gain, so also other popular anti-diabetic and anti-hypertensives. It is of paramount importance on the part of the clinicians to understand the balance between safety and efficacy, and that is where right selection of patient for SGLT2 inhibitor plays an important role [56, 57].
Best Sglt2 Inhibitor Within Class
Differentiation within the class of SGLT2 inhibitors is inconclusive. First of all, so far,there is no head to head trial comparing the efficacy., Regarding safety analysis, especially for cardiovascular events, ,only Empa-Reg trial of empagliflozin has been published so far. This trial has shown that empagliflozin can significantly reduce cardiovascular death, possibly through haemodynamic benefit. However Empa-Regenrolled patients with T2DM of whom more than 99% had prior cardiovascular event. The ongoing CANVAS trial for canagliflozin and DECLARE -Timi 58 trial for dapagliflozin have enrolled varying number of T2DM patient not only with prior history of prior cardiovascular event(secondary prevention), but also subjects at risk of cardiovascular disease ( primary prevention).The later cohort is a true representative of vast majority of patients encountered in day to day practice. Meanwhile, meta-analysis of cardiovascular outcome of phase 2b/3 trials of both canagliflozin and dapagliflozin has shown trends similar to that of Empa- Reg trial. Overall, such data dispel the doubt regarding cardiovascular safety of SGLT2 inhibitors and make them strong contender for a place in anti diabetic armamentarium at various stages of the disease [45, 46, 58, 59].
Right Selection Of Patient For Sglt2 Inhibitor
SGLT2 inhibitor works through insulin independent pathway and this can be prescribed across the entire disease spectrum of T2DM, as suggested by most of the guidelines. It can be used as add on to metformin, sulphonyl urea, insulin etc as second or third line agent. Few situations where it should not be used are patients with estimated glomerular filtration rate (eGFR) below 45 ml/min (), type 1 diabetes , concomitant acute illness or surgery , severe dehydration, pregnant ladies, reproductive age female planning pregnancy, very frail elderly patient or patient with history of recurrent infection. It can also be considered across the wide spectrum of body mass index (BMI) as glycaemic benefit result is similar irrespective of baseline BMI [60, 61, 62].
Conclusion
SGLT2 inhibitors belong to a class of oral anti-diabetic agent which actually works as poly-pill. Its pleotropic umbrella covers excellent control of hyperglycaemia, along with satisfactory control of hypertension, and reasonable reduction of body weight, each of which is an important objective of comprehensive anti-diabetic management on its own merit. In large clinical trials, there are strong early signals of cardiovascular and renal risk reduction which, it is hoped, will be supported by high quality evidences in the coming years. SGLT2 inhibitors should be considered as an early add to standard anti-diabetic therapy in appropriateT2DM patient.
Disclosure
Financial support: None of the authors received any financial or monetary transfer of value for their participation in the writing of the manuscript from any of the pharmaceutical company so far.
Conflict of interest
All the authors have contributed independently to express their personal views in this paper and there is no conflict of interest.
References
-
NCD Risk Factor Collaboration (NCD-RisC) (2016) Worldwide trends in diabetes since 1980: a pooled analysis of 751 population-based studies with 4.4 million participants. The Lancet 387(10027): 1513- 1530.
-
Kalra S, Ghosh S, Aamir A, Ahmed MT, Amin M, et al. (2017) Safe and pragmatic use of sodium-glucose co- transporter 2 inhibitors in type 2 diabetes mellitus: South Asian Federation of Endocrine Societies consensus statement. Indian Journal of Endocrinology and Metabolism 21(1): 210-230.
-
Garber AJ, Abrahamson MJ, Barzilay JI, Blonde L, Bloomgarden ZT, et al. (2016) consensus statement by the american association of clinical endocrinologists and american college of endocrinology on The Comprehensive Type 2 Diabetes Management Algorithm – 2016 Executive Summary. Endocrine Practice 22(1): 84-113.
-
Anderson JH, Brunelle RL, Koivisto VA, Trautmann ME, Vignati L, et al. (1997) Improved mealtime treatment of diabetes mellitus using an insulin analogue. Clinical Therapeutics 19(1): 62-72.
-
Pei Z (2008) From the bench to the bedside: dipeptidyl peptidase IV inhibitors, a new class of oral anti-hyperglycemic agents. Curr Opin Drug Discov Devel 11(4): 512-532.
-
Smyth S, Heron A (2006) Diabetes and obesity: the twin epidemics. Nature medicine 12(1): 75-80.
-
Hsia DS, Grove O, Cefalu WT (2016) An update on sodium-glucose co-transporter-2 inhibitors for the treatment of diabetes mellitus. Current opinion in endocrinology, diabetes, and obesity 24(1): 73-79.
-
Gerich JE (2010) Role of the kidney in normal glucose homeostasis and in the hyperglycaemia of diabetes mellitus: therapeutic implications. Diabetic medicine: A journal of the British Diabetic Association 27(2): 136-142.
-
Vlotides G, Mertens PR (2015) Sodium-glucose co transport inhibitors: mechanisms, metabolic effects and implications for the treatment of diabetic patients with chronic kidney disease. Nephrology Dialysis Transplantation 30(8): 1272-1276.
-
Rahmoune H, Thompson PW, Ward JM, Smith CD, Hong G, et al. (2005) Glucose transporters in human renal proximal tubular cells isolated from the urine of patients with non-insulin-dependent diabetes. Diabetes 54(12): 3427-3434.
-
Rajeev SP, Cuthbertson DJ, Wilding JP (2016) Energy balance and metabolic changes with sodium-glucose co-transporter 2 inhibition. Diabetes, obesity & metabolism 18(2): 125-134.
-
Moses RG, Colagiuri S, Pollock C (2014) SGLT2 inhibitors: New medicines for addressing unmet needs in type 2 diabetes. The Australasian Medical Journal 7(10): 405-415.
-
Seino Y, Inagaki N, Haneda M, Kaku K, Sasaki T, et al. (2015) Efficacy and safety of luseogliflozin added to various oral antidiabetic drugs in Japanese patients with type 2 diabetes mellitus. Journal of diabetes investigation 6(4): 443-453.
-
Tanizawa Y, Kaku K, Araki E, Tobe K, Terauchi Y, et al. (2014) Long-term safety and efficacy of tofogliflozin, a selective inhibitor of sodium-glucose cotransporter 2, as monotherapy or in combination with other oral antidiabetic agents in Japanese patients with type 2 diabetes mellitus: multicenter, open-label, randomized controlled trials. Expert Opin Pharmacother 15(6): 749-766.
-
Poole RM, Dungo RT (2014) Ipragliflozin: first global approval. Drugs 74(5): 611-617.
-
Syed SH, Gosavi S, Shami W, Bustamante M, Farah Z, et al. (2015) A Review of Sodium Glucose Co- transporter 2 Inhibitors Canagliflozin, Dapagliflozin and Empagliflozin. Cardiovascular & hematological agents in medicinal chemistry 13(2): 105-112.
-
Monami M, Dicembrini I, Mannucci E (2016) Effects of SGLT-2 inhibitors on mortality and cardiovascular events: a comprehensive meta-analysis of randomized controlled trials. Acta diabetologica 54(1): 37-38.
-
Zaccardi F, Webb DR, Htike ZZ, Youssef D, Khunti K, et al. (2016) Efficacy and safety of sodium-glucose co- transporter-2 inhibitors in type 2 diabetes mellitus: systematic review and network meta-analysis. Diabetes, obesity & metabolism 18(8): 783-794.
-
Henry RR, Murray AV, Marmolejo MH, Hennicken D, Ptaszynska A, et al. (2012) Dapagliflozin, metformin XR, or both: initial pharmacotherapy for type 2 diabetes, a randomised controlled trial. International journal of clinical practice 66(5): 446-456.
-
Häring HU ML, Seewaldt-Becker E, Weimer M, Meinicke TT (2013) Empagliflozin as add-on to metformin for 24 weeks improves glycemic control in patients with type 2 diabetes (T2DM). Diabetes 36(11): 3396-3404.
-
Del Prato S, Nauck M, Duran-Garcia S, Maffei L, Rohwedder K, et al. (2015) Long-term glycaemic response and tolerability of dapagliflozin versus a sulphonyl urea as add-on therapy to metformin in patients with type 2 diabetes: 4-year data. Diabetes, obesity & metabolism 17(6): 581-590.
-
Bolinder J, Ljunggren O, Johansson L, Wilding J, Langkilde AM, et al. (2014) Dapagliflozin maintains glycaemic control while reducing weight and body fat mass over 2 years in patients with type 2 diabetes mellitus inadequately controlled on metformin. Diabetes, obesity & metabolism 16(2): 159-169.
-
Hardy E, Ptaszynska P, de Bruin TWA, Johnsson E, Parikh SJ, et al. (2013) Changes in lipid profiles of patients with type 2 diabetes mellitus on dapagliflozin therapy. Diabetologia 56(Poster no #947): s379.
-
Heerspink HJ, Johnsson E, Gause-Nilsson I, Cain VA, Sjostrom CD (2016) Dapagliflozin reduces albuminuria in patients with diabetes and hypertension receiving renin-angiotensin blockers. Diabetes, obesity & metabolism 18(6): 590-597.
-
Merovci A, Solis-Herrera C, Daniele G, Eldor R, Fiorentino TV, et al. (2014) Dapagliflozin improves muscle insulin sensitivity but enhances endogenous glucose production. The Journal of clinical investigation 124(2): 509-514.
-
Khatib OEETPS (2006) Guidelines for the Prevention. Management and Care of Diabetes Mellitus. World Health Organisation.
-
Ryden L, Standl E, Bartnik M, Van den Berghe G, Betteridge J, et al. (2007) Guidelines on diabetes, pre- diabetes, and cardiovascular diseases: executive summary. The Task Force on Diabetes and Cardiovascular Diseases of the European Society of Cardiology (ESC) and of the European Association for the Study of Diabetes (EASD). Eur Heart J 28(1): 88- 136.
-
Executive Summary (2010) Standards of Medical Care in Diabetes-2010. Diabetes Care. 33(S1): S4-S10.
-
Rodbard HW, Blonde L, Braithwaite SS, Brett EM, Cobin RH, et al. (2007) American Association of Clinical Endocrinologists medical guidelines for clinical practice for the management of diabetes mellitus. Endocrine practice 13(S1): 1-68.
-
Canadian Diabetes Association Clinical Practice Guidelines Expert Committee (2008) Canadian Diabetes Association 2008 clinical practice guidelines for the prevention and management of diabetes in Canada. Can J Diabetes 32(S1): S1-S201.
-
Michelle Elaine Orme LQ, Nebibe Varol, Kelly Bell, Jayanti Mukherjee (2016) Network Meta-analysis of DPP-4i/SGLT2i Combination as Add-on to Metformin for T2DM American Diabetic Association (ADA), p- 1131.
-
Min SH, Yoon JH, Hahn S, Cho YM (2016) Comparison between SGLT2 Inhibitors and DPP4 Inhibitors Added to Insulin Therapy in Type 2 Diabetes: A Systematic Review with Indirect Comparison Meta-analysis. Diabetes/metabolism research and reviews 33(1).
-
Plosker GL (2014) Dapagliflozin: a review of its use in patients with type 2 diabetes. Drugs 74(18): 2191- 2209.
-
DeFronzo RA, Hompesch M, Kasichayanula S, Liu X, Hong Y, et al. (2013) Characterization of renal glucose reabsorption in response to dapagliflozin in healthy subjects and subjects with type 2 diabetes. Diabetes Care 36(10): 3169-3176.
-
Bonner C, Kerr-Conte J, Gmyr V, Queniat G, Moerman E, et al. (2015) Inhibition of the glucose transporter SGLT2 with dapagliflozin in pancreatic alpha cells triggers glucagon secretion. Nature medicine 21(5): 512-517.
-
Goswami R, Bal CS, Tejaswi S, Punjabi GV, Kapil A, et al. (2001) Prevalence of urinary tract infection and renal scars in patients with diabetes mellitus. Diabetes research and clinical practice 53(3): 181- 186.
-
Nyirjesy P, Sobel JD (2013) Genital mycotic infections in patients with diabetes. Postgraduate medicine 125(3): 33-46.
-
Johnsson KM, Ptaszynska A, Schmitz B, Sugg J, Parikh SJ, et al. (2013) Urinary tract infections in patients with diabetes treated with dapagliflozin. Journal of diabetes and its complications 27(5): 473-478.
-
Johnsson KM, Ptaszynska A, Schmitz B, Sugg J, Parikh SJ, et al. (2013) Ulvovaginitis and balanitis in patients with diabetes treated with dapagliflozin. Journal of diabetes and its complications 27(5): 479-484.
-
Palmer LG, Schnermann J (2015) Integrated Control of Na Transport along the Nephron. Clinical Journal of the American Society of Nephrology CJASN 10(4): 676-687.
-
Yavin Y, Mansfield TA, Ptaszynska A, Johnsson K, Parikh S, et al. (2016) Effect of the SGLT2 Inhibitor Dapagliflozin on Potassium Levels in Patients with Type 2 Diabetes Mellitus: A Pooled Analysis. Diabetes therapy : research, treatment and education of diabetes and related disorders 7(1): 125-137.
-
Peters AL, Buschur EO, Buse JB, Cohan P, Diner JC, et al. (2015) Euglycemic Diabetic Ketoacidosis: A Potential Complication of Treatment With Sodium- Glucose Cotransporter 2 Inhibition. Diabetes Care 38(9):1687-1693.
-
Rosenstock J, Ferrannini E (2015) Euglycemic Diabetic Ketoacidosis: A Predictable, Detectable, and Preventable Safety Concern With SGLT2 Inhibitors. Diabetes Care 38(9): 1638-1642.
-
Administration USFaD (2016) FDA Drug Safety Communication: FDA strengthens kidney warnings for diabetes medicines canagliflozin (Invokana, Invokamet) and dapagliflozin (Farxiga, Xigduo XR).
-
Administration USFaD (2013) FDA approves Invokana to treat type 2 diabetes.
-
Administration USFaD (2014) FDA approves Farxiga to treat type 2 diabetes.
-
Administration USFaD (2014) FDA approves Jardiance to treat type 2 diabetes.
-
Zinman B, Wanner C, Lachin JM, Fitchett D, Bluhmki E, et al. (2015) Empagliflozin, Cardiovascular Outcomes, and Mortality in Type 2 Diabetes. The New England journal of medicine 374(11): 1094.
-
Perkovic V, Jardine M, Vijapurkar U, Meininger G (2015) Renal effects of canagliflozin in type 2 diabetes mellitus. Current Medical Research and Opinion 31(12): 2219-2231.
-
Kohler S, Salsali A, Hantel S, Kaspers S, Woerle HJ, et al. Safety and Tolerability of Empagliflozin in Patients with Type 2 Diabetes. Clinical Therapeutics 38(6): 1299-1313.
-
Long-term Renal Safety with Dapagliflozin Treatment [Internet]. 2014
-
Administration UFaD (2015) Invokana and Invokamet (canagliflozin): Drug Safety Communication - New Information on Bone Fracture Risk and Decreased Bone Mineral Density.
-
Ljunggren O, Bolinder J, Johansson L, Wilding J, Langkilde AM, et al. (2012) Dapagliflozin has no effect on markers of bone formation and resorption or bone mineral density in patients with inadequately controlled type 2 diabetes mellitus on metformin. Diabetes, obesity & metabolism 14(11): 990-999.
-
Mansfield T (2014) Dapagliflozin Is Safe and Well Tolerated in Older Patients with T2DM. American Diabetic Association (ADA). p269.
-
Kalra S, Baruah MP, Sahay R (2014) Medication counselling with sodium glucose transporter 2 inhibitor therapy. Indian Journal of Endocrinology and Metabolism 18(5): 597-599.
-
Stein SA, Lamos EM, Davis SN (2013) A review of the efficacy and safety of oral antidiabetic drugs. Expert opinion on drug safety 12(2): 153-175.
-
Grossman E, Messerli FH (2006) Long-term safety of antihypertensive therapy. Progress in cardiovascular diseases 49(1): 16-25.
-
Neal B, Perkovic V, de Zeeuw D, Mahaffey KW, Fulcher G, et al. (2013) Rationale, design, and baseline characteristics of the Canagliflozin Cardiovascular Assessment Study (CANVAS)--a randomized placebo- controlled trial. American heart journal 166(2): 217- 223.e11.
-
Sonesson C, Johansson PA, Johnsson E, Gause-Nilsson I (2016) Cardiovascular effects of dapagliflozin in patients with type 2 diabetes and different risk categories: a meta-analysis. Cardiovascular Diabetology 15(1): 37.
-
Singh AK (2015) Sodium-glucose co-transporter-2 inhibitors and euglycemic ketoacidosis: Wisdom of hindsight. Indian Journal of Endocrinology and Metabolism 19(6): 722-730.
-
Kalra S (2014) Sodium Glucose Co-Transporter-2 (SGLT2) Inhibitors: A Review of Their Basic and Clinical Pharmacology. Diabetes Therapy 5(2): 355- 366.
-
Alla Shatskov GR, Traci Mansfield (2016) Efficacy and Safety of Dapagliflozin in Patients with Type 2 Diabetes (T2D): Outcomes by Body Mass Index (BMI). American Diabetic Association (ADA), pp. 1141.
- Investigation of Polymorphisms in PPAR-Ɣ and TRHR Genes and their Impact on Turkish Diabetic and Obese Individuals
- The Impact of Aircraft Noise Exposure on the Efficacy of Empagliflozin Therapy in an Animal Model of Obesity
- Rooibos Mitigates Metabolic and Inflammatory Dysfunctions in Mice Fed a High-Carbohydrate Diet
- Synergistic Effect of Combined Leaf Extract of Vernonia amygdalina, Ocimum gratissimum, and Zingiber officinale Tuber on Phytochemical Profile, Antioxidant Activity, Serum Insulin, and Biochemical Parameters in Streptozotocin-Induced Diabetic Rats
- Investigation of Cardiovascular Responses to Aerobic Exercise in Obese University Students
- A Look at the Phase Angle Obtained by Electrical Bioimpedance