Hyperglycaemia, Dyslipidaemia and Diabetes Mellitus
Diabetes is a chronic, complex disease of lifestyle, known to mankind for thousands of years. It is a metabolic disease in which, elevated blood glucose ultimately leads to various clinical complications including, retinopathy, nephropathy, neuropathy, a variety of vascular diseases and, end organ failure. According to the experts, high blood sugar is just a symptom and not the cause for the disease. Major cause for this disease is, impaired insulin production, or insulin insensitivity. Diabetes is supposed to usually begin with insulin resistance, a condition in which, muscle, liver and fat cells do not use insulin efficiently. Sedentary nature, diet and excess weight, seem to contribute significantly to the development of diabetes. A quick Internet search on diabetes management reveals that by and large clinicians focus on fasting glucose, glucose intolerance, postprandial glucose peaks, or glycosylated haemoglobin (HBA1c) levels. Experts are of the opinion, that there is no cure for the diabetes, but it can be managed and controlled. The guidelines and guidance statements from professional societies, also emphasize heavily on the management of blood glucose levels and suggest that these levels be kept at as near to normal levels as possible, by balancing food intake and medication.In this short overview, we will discuss some salient features related to chronic complications of diabetes and express our point of view, on the two major players, hyperglycaemic load and dyslipidaemia, that contribute significantly to the chronic complications associated with diabetes.
Introduction
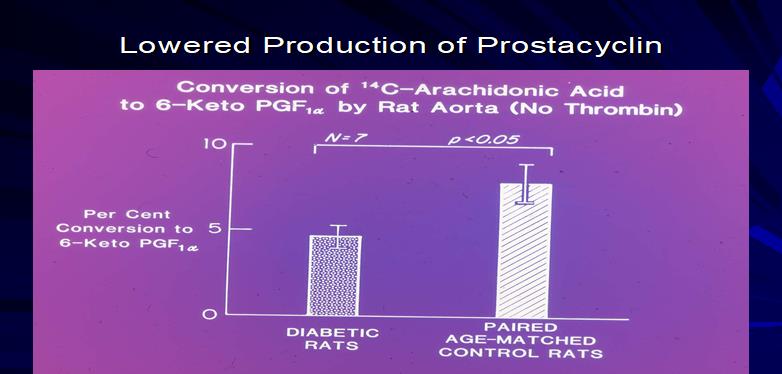
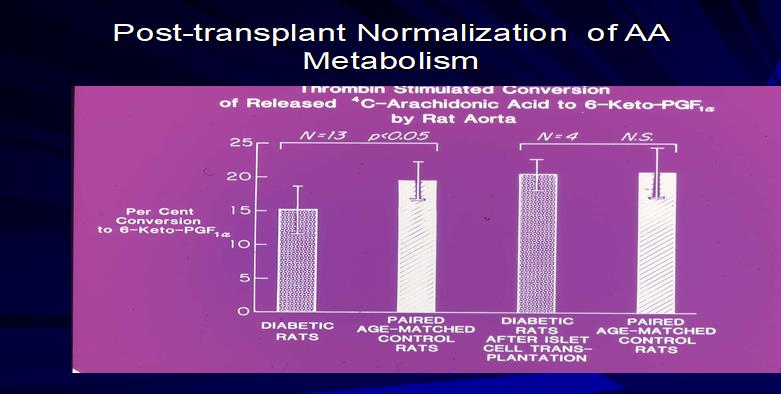
Diabetes mellitus is a chronic metabolic disorder, characterized by impaired glucose metabolism with hyperglycaemia. Elevated levels of blood sugars are well recognized as a major factor, in the pathogenesis of diabetes-related chronic complications, including atherosclerosis. Increased blood glucose, has been shown to mediate nonenzymatic glycosylation of proteins and lipids and interfere with normal physiology and function, by disrupting molecular conformation, alter enzymatic activity, reduce degradative capacity and interfere with receptor recognition. Glycosylated proteins are known to interact, with specific receptors on various cells, associated with the process of vascular atherosclerosis. Such interaction with cells, have been shown to initiate oxidative stress and inflammation, early signs of the development of altered metabolism. Furthermore, hyperglycaemic conditions are known to activate protein kinase C (PKC), leading to altered growth factor expression [1]. In addition to these well-known mechanisms, recent studies suggest that circulating exogenous endothelial progenitor cells (APCs), play an important role in endothelial repair and neovascularization, at sites of vascular injury [2]. Hyperglycaemicconditions seem to alter the function of EPCs and the dysfunction of EPCs, seem to correlate with the occurrence and severity of microvascular and macrovascular complications. In view of the fact, that we do not know the exact underlying mechanism, leading to the dysfunction of EPCs, researchers suggest that altered function of the EPCs, are mediated by multiple mechanisms, including oxidative stress, inflammation and alteration in the Akt activity and nitric oxide pathway. There seems to be convincing evidence on the role of Akt It is well known, that one of the early clinical complications of diabetes mellitus is, the impairment of the balanced production of vasodilators and vasoconstrictors. In a drug-induced animal model we demonstrated at the University of Minnesota, that hyperglycaemia induces altered vascular and platelet arachidonic acid metabolism [4]. In these studies, we noticed that vascular tissues synthesized less vasodilatory prostacyclin upon stimulation with arachidonic acid (Figure 1). On the other hand, platelets synthesised increased pro-aggregatory prostaglandins. We also demonstrated in this animal model, that islet cell transplantation, which normalized blood glucose levels, also normalized the arachidonic acid metabolism, in vascular tissue as well as in platelet, suggesting that hyperglycaemia was probably responsible for this altered fatty acid metabolism (Figure 2).
kinase pathway, in the development of insulin resistance as well as endothelial dysfunction [3].
Discussion
Italian researchers have demonstrated using a precursor product for nitric oxide (NO) synthesis and isotope dilution technique, that nitric oxide synthesis is impaired in elderly and diabetes subjects [5]. The authors concluded that, “the whole-body NO production is decreased in aging and type-2 diabetes and that arginine metabolites, not insulin resistance, appear to be negative regulators of in vivo NO production. In a separate study, researchers using a saliva nitrate test and an intravenous glucose tolerance test reported a correlation between insulin sensitivity and NO synthesis [6]. On the other hand, the UK Prospective Diabetes Study showed that metformin intervention, aimed at improving insulin sensitivity and endothelium dependent vasodilation, led to a significant reduction in cardiovascular events in overweight patients with insulin resistance [7].
Excess weight, obesity, oxidative stress, inflammation and insulin resistance often occur in concert. Oxidative stress, inflammation and insulin resistance may contribute to the development of endothelial dysfunction in overweight individuals. Kelly and associates from Minnesota examined the role of exercise in modulation of inflammation, insulin and endothelial function. They found that, just 8 weeks of exercise training, improved arterial endothelial function in overweight children and adolescents [8]. Several other studies, also have demonstrated that short-term exercise in overweight children and adolescents, improves endothelial functions [9, 10, 11].
According to a report by Professor Roy Taylor of the Newcastle University, UK, excess fat deposit is present in the liver, even before the onset of classical type-2 diabetes and in established diabetes; liver fat is supranormal [12]. In the introduction to his article he states, “Within 7 days of instituting a substantial negative calorie balance, by either dietary intervention or bariatric surgery, fasting glucose levels become normal. This rapid change relates to a substantial fall in liver fat content and return of normal hepatic insulin sensitivity. Earlier researchers have suggested that the action of an enzyme called protein kinase C epsilon (PKCε), in the liver may cause diabetes, by acting on insulin receptors. Using knockout mice model, researchers have demonstrated, that these rodents are protected from glucose intolerance and insulin resistance [13]. Schmitz-Peiffer and associates conclude, “What we found is, that if we removed PKCε production solely from the tissue, the mice were protected from becoming glucose intolerant, similar to when we removed PKCε from the entire animal (knockout model). “If PKCε is changing the nature of fat and affecting the overall health of fat cells, it is changing the types of messages it sends and factors it releases, - which could be acting on the liver and possibly other organs, to interfere with glucose metabolism.” The new study just recently (Oct 2018) reported by the Australian researchers, is challenging what we know about the causes of diabetes. The new study points to fat tissue, as a source of disease and widens our understanding beyond the traditional focus on liver, pancreas and elevated level of blood glucose. According to these researchers, “In high-fat-diet (HFD)-fed mice with PKCε removed from the fat tissue, they saw mostly small, healthy fat cells. In HFD-fed mice with intact PKCε, which were the glucose intolerant, they saw more of unhealthy, engorged fat cells, that tend to have less access to oxygen and inflamed.”
Metabolic healthy obesity is a condition, characterized by obesity, without occurrence of any metabolic complications [14, 15]. According to some reports, there seems to be close to 20% or more of the obese subjects, who belong to this category. If this is true, we should study these individuals to find out, as to how these individuals are protected from the ill effects of overweight. Do they lack PKCε in their fat cells? Do they have over expression of Nrf-2? The transcription factor Nrf-2 (nuclear factor erythroid-2-reoated factor-2, Nrf-2) for instance, a master regulator of detoxification, anti-oxidant, anti-inflammatory and other cytoprotective mechanisms, is raised by health promoting factors. This transcription factor activates the transcription of over 500 genes (so called survival genes) in the human genome, most of which have cytoprotective functions. The most healthful diets such as Mediterranean and Okinawa, are rich in Nrf2 raising nutrients. Modern diets are deficient in such nutrients [16].
When considering intervention studies, we always face an important question, as to what is the earliest metabolic risk that we should start with? From the perspective of Asian population, we should concentrate right from the beginning, which is the prevention of fetal origin of adult diseases (FOADs). British epidemiologist, David Barker proposed a hypothesis, based on the epidemiological studies in India and the UK in 1990, that intrauterine growth retardation, low birth weight and premature birth, have a causal relationship to the origins of hypertension, coronary artery disease and non-insulin dependent diabetes, in middle age [17]. Both India and China, with large diabetic populations, should seriously develop appropriate interventions to prevent this known phenomenon. Even to this day, 30% of the children born in this country are of low birth weight and as such are ‘at
risk’ for the development of cardiometabolic diseases [18, 19, 20, 21]. In view of these observations and the serious problem this phenomenon poses for Indian and Chinese populations, we have initiated a bilateral study between the staff of Children’s Hospital, Washington, DC and the staff of Diabetes Clinic, KEM Hospital Pune, to explore alternate mechanisms, for the observed FOADs in these countries.
Dr. Robert Freishtat and his colleagues from the Children’s National Hospital (CNH) Washington, DC, have described exosomes as “biological tweets” (that is expression in terms of short messages) shed by cells, that allow for intercellular communication and altered gene expression [22]. In their studies, they have demonstrated that adipocytes that exist in large quantities of visceral fat, “tweet” signals that cause downregulation of proteins impacting two key signaling pathways; TGF-Beta and Wnt/β catenin, associated with controlling chronic inflammation and fibrotic diseases throughout the body [6]. Since South Asian phenotype is characterized by increased presence of visceral fat, these observations become very important, for exploring their role if any, in the initiation and promotion of CMDs. With this specific goal/objective in mind, we have initiated bilateral studies between the CNH and KEM Hospital, Pune. Preliminary studies done at these centers are encouraging and currently these bilateral studies are funded by the prestigious National Institutes of Health, USA. This type of early detection of gene expression could be really a game changer for millions of Asians, who are at risk for developing CMDs and other obesity-related clinical complications.
We have articulated in our earlier publications the need to initiate prevention strategies at the earliest possible stage of the pathogenesis of metabolic disorders. Having said that, by large clinicians focus primarily on the management of blood glucose levels. Even the current consensus statements by professional societies, emphasize glycemic control of patients as a primary objective [23]. In addition, they advocate glycemic control, to reduce microvascular complications, they also advocate the management of obesity and prediabetes, as these conditions also are considered as underlying risk factors, for the development of type-2 diabetes. In this overview, we have discussed two important risk factors related to diabetes, hyperglycaemic load and excess of fat. Both of these observed risks, seem to promote the development of endothelial dysfunction, hardening of the arteries and the development of subclinical atherosclerosis. Although we have mentioned, other earlier metabolic alterations such as oxidative stress, low grade inflammation, no serious efforts have been made to address these risks in clinical practice. We feel strongly, that it is time we address these issues anddevelop comprehensive, complementary therapies to reduce, reverse, or prevent these metabolic risks.
Low levels of nitric oxide are associated with impaired endothelial dysfunction. It has been shown, that asymmetric dimethylarginine (ADMA), is a naturally occurring product of metabolism, found in the circulating blood. Elevated levels of ADMA are found, in people with hypercholesterolemia, atherosclerosis, type-2 diabetes and chronic renal failure [24]. ADMA is a novel risk marker, for cardiovascular disease. Prof Jay. Cohen, a pioneer cardiologist at the University of Minnesota, says, “No heart disease, without endothelial dysfunction.” In our opinion, all the clinical complications of diabetes, whether it is nephropathy, neuropathy, retinopathy, or various other vasculopathies, are to a great extent, mediated by the altered flow dynamics and endothelial dysfunction. Professor Ignarro, in his overview on ‘Nitric oxide as a signalling molecule in the vascular system’, writes, “In fact, our original observations on the vaso- relaxant properties of NO were published one year before (1979), the discovery of endothelium-dependent vaso- relaxation and endothelium -derived relaxing factor [25]. At the same time period, other groups were working on prostanoids as possible modulators of vasodilation and vasoconstriction [26, 27].
The discovery by Dyerberg and Bang that Eskimos had lower incidence of cardiovascular disease and increased bleeding tendencies, suggested a role for fish diet in the modulation of platelet and coagulation functions, which by and large, are responsible for acute vascular events [28, 29]. It was assumed that the dietary fatty acids, eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) will shift the balance in the vessel wall arachidonic metabolism and platelet arachidonic acid metabolism, in favour of vasodilation, by producing bioactive prostacyclin and not so very active thromboxanes (TXA) of the three series (TXA3). Contrary to this expectation, studies from our laboratory demonstrated that EPA and DHA are not very well metabolized by the platelets and the preferred substrate for the platelet enzymes are arachidonic acids [29]. Some experts were of the opinion, that a low dose of aspirin also will induce altered arachidonic acid metabolism, by the vascular tissue and platelet, in favour of vasodilation, by inhibiting platelet enzymes and sparing the endothelial cell enzymes. Although a great concept, clinical studies did not support this hypothesis. However, we and others have shown the possibilities, of using dietary substrates for the NO synthesis, as therapeutic agents. Oral supplementation of both L-arginine and L-Citrulline, have been shown to improve endothelial dysfunction in diabetic subjects.
Conclusion
Sugars and Fats seem to be the major determinants for the development of excess weight, obesity and type-2 diabetes [29]. Excess of sugars in the blood as well as fats, initiate a series of metabolic disturbances, such as oxidative stress, low grade inflammation, altered blood flow, endothelial dysfunction, hardening of the arteries and subclinical atherosclerosis. Despite this awareness, clinicians by and large, manage diabetes by administering antiglycemic drugs and pay very little attention, to the associated metabolic risks. Even current guidelines and guidance statements, recommend this approach to the management of diabetes. Of course, these guidelines, also suggest management of blood pressureand blood lipids to prevent the development of cardiovascular risks. As discussed in this overview, looks like both the excess sugars and excess fats, lead to the development of a common risk, which results in the development of endothelial dysfunction.Since this is one of the earliest vascular abnormality that can be detected, by using emerging diagnostic technologies, we suggest development and implementation of complementary therapies to reduce, reverse, or prevent this early risk of vascular dysfunction.
References
-
Aronson D (2008) Hyperglycaemia and the pathobiology of diabetic complications. Adv Cardiol45:1-16.
-
Yiu K, Tse H (2014) Specific role of impaired glucose metabolism and diabetes mellitus in endothelial progenitor cells characteristics and function. Areterioscl Thromb & Vasc Biol34(6): 1136-1143.
-
Zdychova J, Komers R (2005) Emerging role of Akt kinase/protein kinase B signaling in pathophysiology of diabetes and its complications. Physiol Res 54(1): 1-16.
-
Gerrard JM, Stuart MJ, Rao GHR, Steffes MW, Mauer SM, et al. (1980) Alteration in the balance of prostaglandin and thromboxane synthesis in diabetic rats. J Lab and Clin Med95(6): 950-958.
-
Tessari P, Cecchet D, Artusi C, Vettore M, Millioni R, et al. (2013) Roles of insulin, age and asymmetric Dimethylarginine on nitric oxide synthesis in vivo. Diabetes 62(8): 2699-2708.
-
Siervo M, Bluck LJ (2012) In vivo nitric oxide synthesis, insulin sensitivity and asymmetric dimethylarginine in obese subjects without and with metabolic syndrome. Metabolism 61(5): 680-688.
-
UK Prospective Diabetes Study (UKPDS) Group (1998) Effect of intensive blood-glucose control with metformin on complications in overweight patients with type 2 diabetes (UKPDS 34). UK Prospective Diabetes Study (UKPDS) Group. Lancet 352(9131): 854-865.
-
Kelly AS, Wetzsteon RJ, Kaiser DR, Steinberger J, Bank AJ, et al. (2004) Inflammation, insulin and endothelial function in overweight children and adolescents: The role of exercise. J Pediatr 145(6): 731-736.
-
Woo KS, Chook P, Yu CW, Sung RY, Qiao M, et al. (2004) Effect of diet and exercise on obesity-related vascular dysfunction in children. Circ 109(16): 1981- 1986.
-
Watts K, Beye P, Siafarikas A, O'Driscoll G, Jones TW, et al. (2004) Effects of exercise training on vascular function in obese children. J Pedaitr 144(5): 620-625.
-
Watts K, Beye P, Siafarikas A, Davis EA, Jones TW, et al. (2004) Exercise training normalizes vascular dysfunction and improves central adiposity in obese adolescents. J Am Col Cardiol 43(10): 1823-2827.
-
Taylor R (2013) Type-2 diabetes: Etiology and reversibility. Diab Care 36(4): 1047-1055.
-
Brandon AE, Liao BM, Diakanastasis B, Parker BL, Raddatz K, et al. (2019) Protein kinase C epsilon deletion in adipose tissue, but not in liver, improves glucose tolerance. Cell Metab 29(1): 183-191.
-
Acharya S, Shukla S (2018)Metabolic healthy obesity- A paradoxical fallacy? J Cliand Diag Res 12(10): OE07- OE10.
-
Stefan N, Häring HU, Hu FB, Schulze MB (2013) Metabolically healthy obesity: epidemiology, mechanisms and clinical implications. Lancet Diab Endocrinol 1(2): 152-162.
-
Hybertson BM, Gao B, Bose SK, McCord JM (2011) Oxidative stress in health and disease: The therapeutic potential of Nrf2 activation. Mol Aspects of Med 32(4-6): 234-246.
-
Calkins K, Devaskar SU (2011) Fetal origin of adult disease. Curr Probl Pediatr Health Care 41(6): 158- 176.
-
Rao GHR (2018) Excess weight, obesity, diabetes type-2 and clinical complications. Arch Diab& Obesity 1(1).
-
Rao GHR (2018) Novel sub-groups of adult onset diabetes and its clinical complications. Editorial Arch Endocrinol and Diab Care 1(1):11-12.
-
Gundu H R Rao(2018) Integration of Novel emerging technologies for the management of type-2 diabetes. Arch Diab & Obesity 1(1).
-
Rao GHR, Gandhi PG, Sharma V (2014) Clinical complications of type-2 diabetes mellitus in South Asian and Chinese populations. An overview. J Diab Metab 5:420.
-
Ferrante SC, Nadler EP, Pillai D, Hubal MJ, Wang Z, et al. (2015) Adipocyte-derived exosomalmiRNAs: a novel mechanism for obesity-related disease. Ped Res 77(3): 447-454.
-
Garber AJ, Abrahamson MJ, Barzilay JI, Blonde L, Bloomgarden ZT, et al. (2018) Consensus statement by the American Association of Clinical Endocrinologists and American College of Endocrinology on the comprehensive type2 diabetes management algorithm-2018 Executive Summary. Endocrine Pract 24(1): 91-120.
-
Sibal L,Agarwal SC, Home PD, Boger RH (2010) The role of asymmetric dimethylarginine (ADMA) in endothelial dysfunction and cardiovascular disease. Curr Cardiol Rev 6(2): 82-90.
-
Ignarro L, Giuseppe C, Alessandro C, Napoli C (1999) Nitric oxide as a signalling molecule in the vascular system: An overview. J Cardiovasc Pharmacol 34(6): 879-886.
-
Rao GHR (2018) Arachidonic acid metabolism, thrombosis and stroke. J of CardiolCardiovascTher 11(1): JOCCT.MS.ID.555803.
-
Rao GHR (2018) Omega-3 fatty acids: Cardiovascular Disease. CardiolCardiovascTher 10(5): JOCCT. MS. ID.555797.
-
DybergJ, Bang HO (1979) Haemostatics function and platelet polyunsaturated fatty acids in Eskimos. The Lancet 2(8140): 433-435.
-
Ambrosini GL, Johns DJ, Northstone K, Emmett PM, Jebb SA (2016) Free sugars and total fat are important characteristics of a dietary pattern associated with adiposity across childhood and adolescence. J Nutr Epidemiol 146: 778-784.
- Investigation of Polymorphisms in PPAR-Ɣ and TRHR Genes and their Impact on Turkish Diabetic and Obese Individuals
- The Impact of Aircraft Noise Exposure on the Efficacy of Empagliflozin Therapy in an Animal Model of Obesity
- Rooibos Mitigates Metabolic and Inflammatory Dysfunctions in Mice Fed a High-Carbohydrate Diet
- Synergistic Effect of Combined Leaf Extract of Vernonia amygdalina, Ocimum gratissimum, and Zingiber officinale Tuber on Phytochemical Profile, Antioxidant Activity, Serum Insulin, and Biochemical Parameters in Streptozotocin-Induced Diabetic Rats
- Investigation of Cardiovascular Responses to Aerobic Exercise in Obese University Students
- A Look at the Phase Angle Obtained by Electrical Bioimpedance