Effect of Liraglutide on Weight Reduction in Euthyroid, Non Diabetic Obese Patients
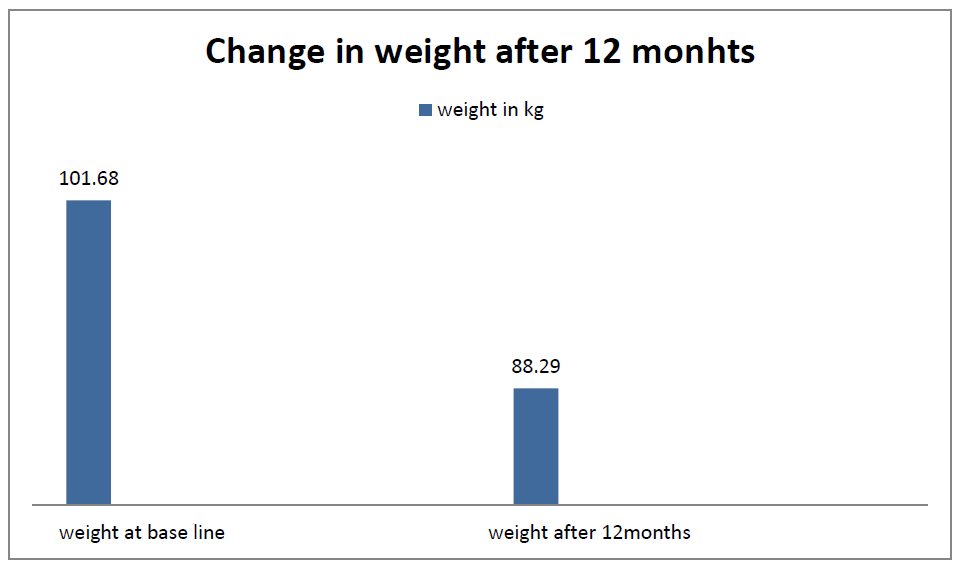
Introduction: Liraglutide is an effective drug for the treatment of type 2 diabetes mellitus (T2DM). Liraglutide 3 mg is approved for obesity. We assessed the effect of liraglutide on body weight and tolerability in obese individuals with lesser dose. Objective: To evaluate the effect of the liraglutide on weight loss in overweight and obese Indian patients. Material and methods: Data was collected from 15 patients over 12 month duration from case record section retrospectively. Patient’s weight and dose of liraglutide were studied. Result: Mean weight at baseline was 101.68 kg, minimum dose of liraglutide at the beginning was 0.3 mg .The mean change in body weight after 1 year was 13.39 kg and maximum dose of liraglutide was 2.4 mg. The most common side effect was nausea. Conclusion: Liraglutide treatment, at a much lower dose than 3 mg daily, significantly improves weight loss in obese non diabetic Indian subjects.
Kangude4 and Nikita Jitkar5
physician, Noble Hospital, Pune, Maharashtra, India, Email: kb21084@gmail.com dose.
retrospectively. Patient’s weight and dose of liraglutide were studied.
effect was nausea.
diabetic Indian subjects.
Keywords: Liraglutide; Obesity; Type 2 Diabetes Patients; Weight Loss
Introduction
According to the World Health Organization (WHO), obesity is one of the most common, yet among the most neglected, public health problems in both developed and developing countries [1]. India, with 1.2 billion people is the second most populous country in the world and is currently experiencing rapid epidemiological transition. Under nutrition due to poverty which dominated in the past, is being rapidly replaced by obesity associated with affluence [2].
World Health Organization (WHO) defines overweight and obesity as “An abnormal or excessive fat accumulation that presents a risk to health.
The body mass index (BMI) is an attempt to quantify the amount of tissue mass (muscle, fat and bone) individually and BMI categories are defined as follows: lean when BMI below 18.5, normal weight when BMI of 18.5–24.9, overweight when BMI of 25– 29.9, and obese when BMI over 30 kg / m2 [3]. In accordance with WHO, normal weight East Asians have a BMI of 18.5–23, overweight when BMI of 23–27.4 and obese with BMI over 27.5 kg / m2 [4].
There are numerous causes of obesity depending on age, lifestyle, profession, and medical circumstances. Treatment of overweight is suggested only when patients have two or more risk factors (hypertension, high blood cholesterol, type 2 diabetes, coronary heart disease, and asthma, etc.) or a high waist circumference.
The inability to limit excessive food intake contributes to uncontrolled weight gain, mainly because it seems to be satisfying to eat a more palatable energetic and obesogenic type of food. The high hedonic value and tempting foods are the main culprits to overeat or eat beyond the immediate metabolic need (food reward behaviour) [5].
The relationship between energy intake and expenditure is modulated not only by environmental and behavioural factors but also by genetic determinants and neuroendocrine feedback mechanisms. These mechanisms are regulated by the hypothalamus, the central site for the homeostatic regulation of body weight. The hypothalamus integrates peripheral hormonal signals from the gastrointestinal tract [ghrelin, cholecystokinin, peptide YY, pancreatic polypeptide (PP), GLP-1], pancreas (insulin) and adipose tissue (leptin), that modify central orexigenic [e.g. neuropeptide Y (NPY)], agouti-related peptide (AgRP) and anorexigenic [e.g. alpha-melanocyte stimulating hormone (α-MSH), a proopiomelanocortin (POMC)-derived peptide], cocaine- and amphetamine- regulated transcript [CART]) neuropeptides [6].
The hedonic appetite regulation is carried out in the limbic regions such as the hippocampus, amygdala, nucleus accumbens, ventral tegmental area, cingulate Reema Kashiva, et al. Effect of Liraglutide on Weight Reduction in Euthyroid, Non Diabetic Obese Patients. Diabetes Obes Int J 2019, 4(3): 000204.
gyrus, orbitofrontal cortex, insula and prefrontal cortex. These areas are involved in the development of the conditioned response and reward. Although classical neurotransmitters involved in this network are dopamine, serotonin, and GABA, several animal studies emphasize the contribution of GLP-1 in the system [7].
Combination therapies are always applicable when the single mode is unable to generate the desired results. In the treatment of obesity combination of diet and physical activities such as brisk walking, jogging, riding a stationary bicycle, swimming may provide the results better than individual treatment. This combination of reduced-calorie diet and increased physical activity reduces the fat stored within the body and also prevents the regaining of weight. When the combination therapy fails then pharmacotherapy plays an important role. Anti- obesity medication or weight loss drugs are pharmacological agents that reduce or control weight. These drugs alter one of the fundamental processes of the human body, weight regulation, by altering either appetite, or absorption of calories [8]. There are several drugs available in the market for the treatment of obesity and overweight. Most of the drugs have established its practical effectiveness in the treatment of obesity. However, the associated adverse drug reactions confined the use of many drugs and may even have resulted in withdrawal.
The only anti-obesity medication approved for long- term treatment of obesity is orlistat in the USA, other than orlistat, phentermine-topiramate (PHEN/TPM) is also available, but only for short term. Topiramate- phentermine (PHEN/TPM) combination use is also associated with serious harm as its label include warning about memory, attention, or language problems and depression, label also warn about metabolic acidosis, increased heart rate, anxiety, insomnia, and elevated creatinine levels [9]. European Medicines Agency (EMA) said approval was unlikely, and the EMA rejected phentermine-topiramate. In 2012 676 patients were studied for 108 weeks utilising 7.5 mg phentermine / 46 mg controlled-release topiramate (7.5/46), or 15 mg phentermine / 92 mg controlled-release topiramate (15/92) and concluded that, PHEN/TPM CR in conjunction with lifestyle modification may provide a well-tolerated and effective option for the sustained treatment of obesity complicated by cardio-metabolic disease [10].
Copyright© Reema Kashiva, et al.
A higher percentage of total body weight is lost with use of combination phentermine / topiramate compared to orlistat, lorcaserin, and bupropion/naltrexone but there are more contraindications to its use and potential cardiovascular adverse effects due to adrenergic agonism [11].
Gadde K, et al. [12] in 2012 also studied PHEN-TPM in patients with BMI ≥ 35 kg/m2 and concluded that PHEN/TPM CR demonstrated dose‐dependent effects on weight and metabolic variables. The most common adverse events were paresthesia, dry mouth, constipation, dysgeusia, and insomnia. Dropout rate from the study was 47.1% for placebo patients, 39.0% for 3.75/23 PHEN/TPM CR patients, and 33.6% of 15/92 PHEN/TPM CR patients [12]. Orlistat reduces intestinal fat absorption by inhibiting pancreatic lipase. Some side-effects of using orlistat include frequent, oily bowel movements (steatorrhea). But if fat in the diet is reduced, symptoms often improve [13]. Lorcaserin was approved June 28, 2012 for obesity with other co-morbidities. The average weight loss by study participants was modest; It reduces appetite by activating a type of serotonin receptor known as the 5-HT2C receptor in a region of the brain called the hypothalamus, which is known to control appetite [13]. Also lorcaserin and bupropion / naltrexone yielded similar weight loss but carry different adverse effect profiles and interactions with other psyciatric medications which may preclude use of one over the other [11].
Sibutramine is an anorectic or appetite suppressant, reducing the desire to eat. It may increases blood pressure and may cause dry mouth, constipation, headache, and insomnia, and more rarely stroke or heart attack. Sibutramine has been withdrawn from the market due to its cardiovascular side effects. Rimonabant was an anorectic antiobesity drug that was first approved in Europe in 2006 but was withdrawn worldwide in 2008 due to serious psychiatric side effects. In people with Diabetes mellitus type 2, the drug metformin can reduce weight by limiting the amount of glucose that is produced by the liver as well as increases muscle consumption of glucose. It also helps in increasing the body's response to insulin [14].
Hormone GLP-1, is secreted in intestine in response to the presence of food. Among other effects, GLP-1 delays gastric emptying and promotes a feeling of satiety. Liraglutide 3.0 mg was first approved in December 2014 for the treatment of obesity in the United States of Reema Kashiva, et al. Effect of Liraglutide on Weight Reduction in Euthyroid, Non Diabetic Obese Patients. Diabetes Obes Int J 2019, 4(3): 000204.
America, being a higher dose than that already approved for second-line treatment of Type 2 diabetes melitus which is maximum of 1.8 mg [15].
Kumar R, et al. [11] studied obese individuals without diabetes mellitus and demonstrated that liraglutide 3.0 mg/day suppressed acute food intake (-16% reduction), subjective hunger (evaluated based on subject‐reported satiety, fullness, hunger and prospective food consumption), and delayed gastric emptying.
GLP-1 receptors (GLP-1R) on POMC/CART-expressing arcuate (ARC) neurons likely mediate liraglutide-induced weight loss. The weight loss is reduced by local blockade of GLP-1R on ARC neurons with an antagonist of GLP-1R [16]. Peripheral and central activation of GLP-1 receptors (GLP-1Rs) produces incretin effects (increased insulin secretion) and reduces food intake and body weight [17]. Anorectic effects following GLP-1R activation in mesolimbic pathway nuclei, including the ventral tegmental area (VTA) and nucleus accumbens suggest that GLP-1R signaling has a role in higher-order, motivational aspects of feeding behaviour [18, 19]. GLP-1R signaling reduces food intake and body weight via action at multiple brain regions, including hypothalamic, hindbrain, and mesolimbic nuclei [20]. Hsu T, et al. [21] Hypothalamus has a critical role in feeding behaviour. Central nervous system GLP-1R signaling influences feeding via action not only on receptors expressed in traditional feeding centers (ie, hypothalamus and caudal brainstem), but also in various midbrain and forebrain nuclei that control learned and motivational behaviors [22]. As a result, liraglutide was also developed as a weight loss agent and its 3.0 mg daily dose has shown encouraging results in multiple clinical trials [23]. Liraglutide 3.0 mg daily subcutaneous injection is the newest FDA approved drug for chronic weight management in patients with obesity or who are overweight with a BMI ≥27 kg/m2 and have a weight related comorbid condition [24]. • Glucagon-Like Peptide-1 GLP-1 is primarily synthesized by and secreted from the L-cells, which are mainly located in the distal ileum and colon.(24) Secretion of GLP-1 from the gut in response to food intake is biphasic: the early phase occurs within 10–15 min after food ingestion and this is followed by a longer second phase peaking at 30–60 min. Once released, GLP-1 is rapidly inactivated in the circulation by the enzyme dipeptidyl peptidase-4 (DPP-4), resulting in a plasma half-life of less than 2 min [25].
Copyright© Reema Kashiva, et al.
Only about 10–15% of the GLP-1 secreted from intestinal L-cells reaches the peripheral tissues, and the pancreatic β- and α-cells; the majority of GLP-1 is inactivated in the intestine, portal vein and in the liver therefore, liraglutide was created by substituting arginine for lysine at position 34 in the GLP‐1 peptide and adding a palmitic acid chain with a glutamic acid spacer on the lysine residue at position 26 to improve the pharmacokinetic effects [26]. Following subcutaneous injection of liraglutide, peak absorption occurs at 11 hours and absolute bioavailability is 55% [26]. Liraglutide is highly protein bound (98%) due to the fatty acid chain and has a large volume of distribution. Its half‐life in healthy individuals and in those with type 2 diabetes is 13 hours, allowing for once daily subcutaneous administration. It causes a glucose dependent stimulation of insulin secretion, reduction in plasma glucagon concentrations [27]. The underlying mechanisms that mediate the effects of weight reduction of liraglutide are most probably a combination of effects on the gastrointestinal tract and the brain. Appetite suppression and delayed gastric emptying are thought to be responsible for the weight lowering effects of GLP‐1 [28]. Liraglutide 3.0 mg is not approved in India.
Materials & Methods
Aim
Indian observational study to evaluate efficacy for weight loss and adverse consequences of liraglutide in euthyroid, non-diabetic overweight or obese patients.
Objective
The study objective was to study effect of liraglutide at therapeutic doses approved to treat diabetes which can
Results
be used for weight loss in euthyroid, non-diabetic obese patients in India.
Study Type – Retrospective
Inclusion criteria: study included patients from age group 18-65 years 1) BMI of more than 27.5 kg/m2 2) Euthyroid patients 3) Non dyslipidemic patients 4) Patients not willing for fat reduction surgery / surgical intervention for weight loss. Exclusion crieteria 1) Patients taking drugs for weight loss as metformin, phentermine-topiramate, lorcaserin, orlistat. 2) Patients with HbA1c level more than 6.4 Before starting a patient on liraglutide, every patient was subjected to 500 calorie deficient diet of their prescribed diet per day with the help of nutritionist. Their diet plan was monitored over the phone, through whatsapp messaging application and at clinic visit by nutritionist. Every patient was also subjected to physiotherapy in the form of moderate aerobic exercises at least for 150 minutes per week. Diet modification and physiotherapy was carried for at least 6 months before starting these patients on liraglutide. The data was collected from patient case records. Ethical approval was taken from institutional ethical committee. Patient’s demographic characteristics, weight, height, BMI, co morbid conditions if any, starting dose of liraglutide, HBA1C, fasting plasma and random blood sugar were noted.
| Dose of Liraglutide | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Body Weight (Kg) | BMI (Cm/m2) | HBA1C (%) | ||||||||||
| (mg) (Starting) | ||||||||||||
| CASE 1 | 83 | 34.5 | 5.4 | 0.3 | ||||||||
| CASE 2 | 105.3 | 43.3 | 5.6 | 0.6 | ||||||||
| CASE 3 | 88 | 33.1 | 5.4 | 0.6 | ||||||||
| CASE 4 | 115 | 44.9 | 5 | 0.6 | ||||||||
| CASE 5 | 119.6 | 33.7 | 5.7 | 0.6 | ||||||||
| CASE 6 | 90 | 35.2 | 5.1 | 0.6 | ||||||||
| CASE 7 | 86 | 35.3 | 5.5 | 0.6 | ||||||||
| CASE 8 | 173 | 72.9 | 4.5 | 0.6 | ||||||||
| CASE 9 | 89 | 33.1 | 5.5 | 0.3 | ||||||||
| CASE 10 | 84 | 32.8 | 5 | 0.6 |
Reema Kashiva, et al. Effect of Liraglutide on Weight Reduction in Euthyroid, Non Diabetic Obese Patients. Diabetes Obes Int J 2019, 4(3): 000204.
Copyright© Reema Kashiva, et al.
| CASE 11 | 98 | 29.6 | 5.4 | 0.6 |
|---|---|---|---|---|
| CASE 12 | 106 | 36.7 | 4.5 | 0.6 |
| CASE 13 | 112 | 51.8 | 5.3 | 0.6 |
| CASE 14 | 90 | 33.1 | 5.1 | 0.6 |
| CASE 15 | 86.4 | 35.5 | 5.2 | 0.6 |
Table1: Shows baseline characteristic of patients. Average age of patient in the study was 44.7 year. Mean height of the patient was 162.4 cm. Mean BMI of the patient was 39.03. Mean weight at baseline was 101.68 kg. Minimum dose of liraglutide as the beginning was 0.3 mg. Mean change in body weight after 1 year was 13.39 kg.(Figure 1 ) Maximum dose of liraglutide was 2.4 mg. The most common adverse effect was nausea.
Discussion
Liraglutide has been shown to be effective at inducing and sustaining weight loss among obese patients, and a 3 mg dosage has been approved for chronic weight management in patients with obesity or who are overweight with a BMI ≥27 kg/m2 [26].
Liraglutide once daily maximum 1.8 mg was approved for type 2 diabetics’ patients. When used as adjuvant in obese and overweight patients who did not have diabetes was associated with weight loss.
Among the studies of liraglutide reported from India, three initial studies reported by Kesavadev, et al. [29] & Sanyal, et al. [30] and Kesavadev, et al. [31] were for a period of 24 weeks. However, as time has progressed, it became relatively easier for the clinicians to gather data of subjects continuing liraglutide for a year and more.
Results from Indian observational studies have demonstrated the ability of liraglutide to induce weight loss. A weight loss of 8 kg (±2.4 kg) from a baseline weight of 110 kg (±12.5 kg) was observed in 25 obese non diabetic subjects after 12 weeks of liraglutide therapy, with a dose of 1.2 mg [32]. Significant reduction of mean body weight (from 96.33 ± 14.45 at baseline to 90 ± 13.47at 3 months and to 86.25 ± 13.19 at 9 months, P < 0.001) were reported after 3 and 9 months of liraglutide treatment, with a dose of 1.8 mg [33]. Even a low dose (0.6 mg) of liraglutide showed a reduction of 6.03 kg over 24 weeks.
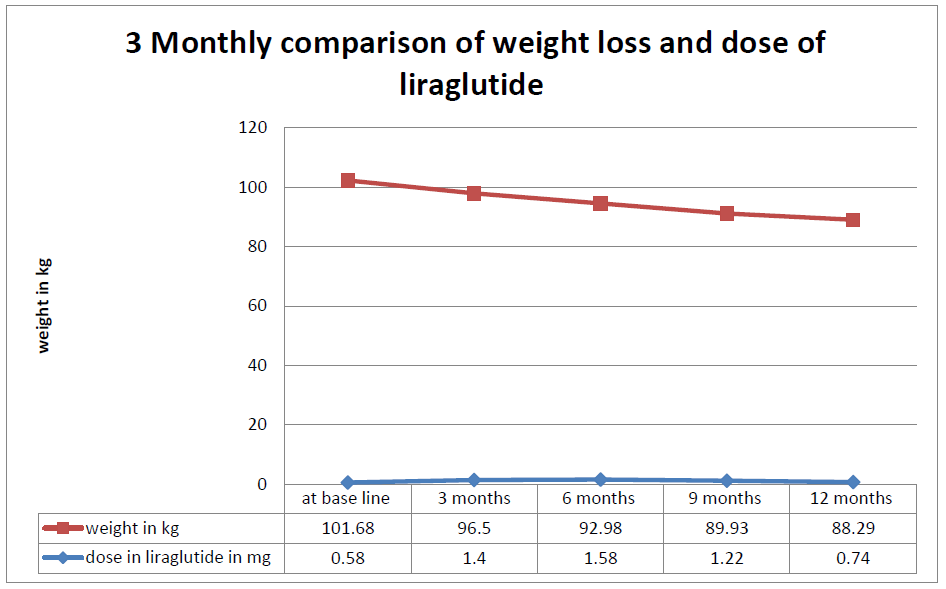
In our study the mean change in weight was 13.39 kg over the period of 12 months with a maximum dose of 2.4 mg. (Table 2 & Figure 1). Only 1 patient received maximum dose of liraglutide 2.4 mg, rest all were managed on minimum dose of 0.6 mg, 1.2 mg and 1.8 mg dosage. Our result is in consistent with the short duration studies mentioned above. The safety profile of liraglutide was consistent with findings in previous reports. Gastrointestinal complains are common and mostly nausea and that too occurred especially when dosage of liraglutide was escalated. Nausea subsided after few days after continuing liraglutide. Starting with the lower dose and up titrating it slowly will reduce the gastrointestinal side effects.
| Weight (Kg)at base line | Weight (Kg) after 12 months | Change in weight (Kg) after 12 months | |||||||
|---|---|---|---|---|---|---|---|---|---|
| CASE 1 | 83 | 70 | 13 | ||||||
| CASE 2 | 105.3 | 95 | 10.3 | ||||||
| CASE 3 | 88 | 74 | 14 | ||||||
| CASE 4 | 115 | 98 | 17 | ||||||
| CASE 5 | 119.6 | 99 | 20.6 | ||||||
| CASE 6 | 90 | 83 | 7 | ||||||
| CASE 7 | 86 | 79 | 7 | ||||||
| CASE 8 | 173 | 160 | 13 | ||||||
| CASE 9 | 89 | 77 | 12 |
Table 3: Change in weight after 12 months.
Reema Kashiva, et al. Effect of Liraglutide on Weight Reduction in Euthyroid, Non Diabetic Obese Patients. Diabetes Obes Int J 2019, 4(3): 000204.
Copyright© Reema Kashiva, et al.
| CASE 10 | 84 | 73 | 11 |
|---|---|---|---|
| CASE 11 | 98 | 85.5 | 12.5 |
| CASE 12 | 106 | 90 | 16 |
| CASE 13 | 112 | 90 | 22 |
| CASE 14 | 90 | 81 | 9 |
| CASE 15 | 86.4 | 69.9 | 16.5 |
Table 4: Change in weight after 12 months.
| At base line | 3 months | 6 months | 9 months | 12 months | ||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Weight | l | iraglutid | e | Weigh | t | liraglutide | Weigh | t | l | iraglutide | Weight | l | iraglutide | Weight | l | iraglutid | e | |||||||||||||
| (Kg) | (mg) | (Kg) | (mg) | (Kg) | (mg) | (Kg) | (mg) | (Kg) | (mg) | |||||||||||||||||||||
| CASE 1 | 83 | 0.6 | 78 | 0.9 | 71.5 | 0.6 | 70 | 0.6 | 70 | 0.6 | ||||||||||||||||||||
| CASE 2 | 105.3 | 0.6 | 100 | 1.8 | 98 | 1.8 | 96 | 1.8 | 95 | 1.8 | ||||||||||||||||||||
| CASE 3 | 88 | 0.6 | 80 | 1.2 | 76 | 1.2 | 74 | 0.6 | 74 | 0.6 | ||||||||||||||||||||
| CASE 4 | 115 | 0.6 | 107 | 1.8 | 104 | 1.8 | 101 | 1.2 | 98 | 0.6 | ||||||||||||||||||||
| CASE 5 | 119.6 | 0.6 | 112 | 1.8 | 105 | 1.8 | 100 | 1.2 | 99 | 0.6 | ||||||||||||||||||||
| CASE 6 | 90 | 0.6 | 88 | 1.8 | 86 | 1.8 | 84 | 1.2 | 83 | 1.2 | ||||||||||||||||||||
| CASE 7 | 86 | 0.6 | 80 | 0.3 | 79 | 0.3 | 79 | 0.3 | 79 | 0.3 | ||||||||||||||||||||
| CASE 8 | 173 | 0.3 | 165 | 1.2 | 162 | 1.2 | 160 | 1.2 | 160 | 1.2 | ||||||||||||||||||||
| CASE 9 | 89 | 0.6 | 86 | 1.8 | 82 | 3 | 78.1 | 1.2 | 77 | 0.6 | ||||||||||||||||||||
| CASE 10 | 84 | 0.6 | 82 | 1.2 | 79 | 1.2 | 76 | 1.2 | 73 | 0.6 | ||||||||||||||||||||
| CASE 11 | 98 | 0.6 | 94 | 1.8 | 90 | 1.8 | 87.5 | 1.2 | 85.5 | 0.6 | ||||||||||||||||||||
| CASE 12 | 106 | 0.6 | 100.5 | 1.8 | 98.5 | 1.8 | 90.5 | 1.2 | 90 | 0.6 | ||||||||||||||||||||
| CASE 13 | 112 | 0.6 | 107 | 1.2 | 100 | 1.2 | 96 | 1.2 | 90 | 0.6 | ||||||||||||||||||||
| CASE 14 | 90 | 0.6 | 88 | 1.2 | 85 | 2.4 | 83 | 2.4 | 81 | 0.6 | ||||||||||||||||||||
| CASE 15 | 86.4 | 0.6 | 80 | 1.2 | 78.8 | 1.8 | 73.9 | 1.8 | 69.9 | 0.6 |
Table 5: Monthly comparison of weight loss and dose of liraglutide.
Case 16 Lost only 2 kg of her baseline body weight with a maximum dosage of 2.4 mg of liraglutide over a period of 3 months so liraglutide was stopped in this patient. Table 3: Monthly comparison of weight loss and dose of liraglutide.
Reema Kashiva, et al. Effect of Liraglutide on Weight Reduction in Euthyroid, Non Diabetic Obese Patients. Diabetes Obes Int J 2019, 4(3): 000204.
Copyright© Reema Kashiva, et al.
Liraglutide at a dose much lower than that of 3 mg (as the approved anti-obesity dose) produced a substantial reduction body weight of obese non-diabetic Indian subjects, which can make it a relatively less expensive anti-obesity agent compared to 3 mg liraglutide.
In Conclusion Liraglutide treatment, at a much lower dose than 3 mg daily, significantly helps in weight loss in obese/ overweight euthyroid non diabetic Indian subjects. Limitation of the study was sample size. Sample size was small, to generalise the liraglutide effect on weight loss.
References
-
Pradeepa R, Anjana RM, Joshi SR, Bhansali A, Deepa M, et al. (2019) Prevalence of generalized & abdominal obesity in urban & rural India--the Reema Kashiva, et al. Effect of Liraglutide on Weight Reduction in Euthyroid, Non Diabetic Obese Patients. Diabetes Obes Int J 2019, 4(3): 000204. ICMR-INDIAB Study (Phase-I) [ICMR- NDIAB-3]. Indian J Med Res 142(2): 139-150.
-
Mohan V, Deepa R (2006) Obesity and abdominal obesity in Asian Indians. Indian J Med Res 123(5): 593-596.
-
WHO (2018) Obesity and overweight. World health organisation.
-
WHO Expert Consultation (2004) Appropriate body- mass index for Asian populations and its implications for policy and intervention strategies. Lancet 363(9403): 157-163.
-
Buhmann H, le Roux CW, Bueter M (2014) The gut– brain axis in obesity. Best Pract Res Clin Gastroenterol 28(4): 559-571.
-
Sweeting AN, Hocking SL, Markovic TP (2015) Pharmacotherapy for the treatment of obesity. Mol Cell Endocrinol 418: 173-183.
-
Hsu TM, Hahn JD, Konanur VR, Lam A, Kanoski SE (2015) Hippocampal GLP-1 Receptors Influence Food Intake, Meal Size and Effort-Based Responding for Copyright© Reema Kashiva, et al. Food through Volume Transmission. Neuropsychopharmacology 40(2): 327-337.
-
(2019) Obesity prevention. Guidance and guidelines, NICE.
-
Woloshin S, Schwartz LM (2014) The New Weight- Loss Drugs, Lorcaserin and Phentermine-Topiramate. JAMA Intern Med 174(4): 615-619.
-
Allison DB, Gadde KM, Garvey WT, Peterson CA, Schwiers ML, et al. (2012) Controlled-Release Phentermine/Topiramate in Severely Obese Adults: A Randomized Controlled Trial (EQUIP). Obesity 20(2): 330-342.
-
Kumar RB, Aronne LJ (2015) Efficacy comparison of medications approved for chronic weight management. Obesity 23(S1): S4-S7.
-
Garvey WT, Ryan DH, Look M, Gadde KM, Allison DB, et al. (2012) Two-year sustained weight loss and metabolic benefits with controlled-release phentermine/topiramate in obese and overweight adults (SEQUEL): a randomized, placebo-controlled, phase 3 extension study. Am J Clin Nutr 95(2): 297- 308.
-
Bray GA, Frühbeck G, Ryan DH, Wilding (2016) JPH Management of obesity. Lancet, pp: 1947-1956.
-
Bray GA, Greenway FL (1999) Current and Potential Drugs for Treatment of Obesity. Endocr Rev 20(6): 805-875.
-
Novo Nordisk (2015) Novo Nordisk News & amp; Media-Diabetes Care.
-
Secher A, Jelsing J, Baquero AF, Hecksher Sørensen J, Cowley MA, et al. (2014) The arcuate nucleus mediates GLP-1 receptor agonist liraglutide- dependent weight loss. J Clin Invest 124(10): 4473- 4488.
-
Rüttimann EB, Arnold M, Hillebrand JJ, Geary N, Langhans W (2009) Intrameal Hepatic Portal and Intraperitoneal Infusions of Glucagon-Like Peptide-1 Reduce Spontaneous Meal Size in the Rat via Different Mechanisms. Endocrinology 150(3): 1174-81.
-
Alhadeff AL, Rupprecht LE, Hayes MR (2012) GLP-1 Neurons in the Nucleus of the Solitary Tract Project Directly to the Ventral Tegmental Area and Nucleus Reema Kashiva, et al. Effect of Liraglutide on Weight Reduction in Euthyroid, Non Diabetic Obese Patients. Diabetes Obes Int J 2019, 4(3): 000204. Accumbens to Control for Food Intake. Endocrinology 153(2): 647-658.
-
Dossat AM, Lilly N, Kay K, Williams DL (2011) Glucagon-like peptide 1 receptors in nucleus accumbens affect food intake. J Neurosci 31(41): 14453-14457.
-
Hayes MR, Skibicka KP, Grill HJ (2008) Caudal Brainstem Processing Is Sufficient for Behavioral, Sympathetic, and Parasympathetic Responses Driven by Peripheral and Hindbrain Glucagon-Like-Peptide-1 Receptor Stimulation. Endocrinology 149(8): 4059- 68.
-
Kanoski SE, Fortin SM, Ricks KM, Grill HJ (2013) Ghrelin signaling in the ventral hippocampus stimulates learned and motivational aspects of feeding via PI3K-Akt signaling. Biol Psychiatry 73(9): 915-23.
-
Dickson SL, Shirazi RH, Hansson C, Bergquist F, Nissbrandt H, et al. (2012) The Glucagon-Like Peptide 1 (GLP-1) Analogue, Exendin-4, Decreases the Rewarding Value of Food: A New Role for Mesolimbic GLP-1 Receptors. J Neurosci 32(14): 4812-4820.
-
Lean MEJ, Carraro R, Finer N, Hartvig H, Lindegaard ML, et al. (2014) Tolerability of nausea and vomiting and associations with weight loss in a randomized trial of liraglutide in obese, non-diabetic adults. Int J Obes 38(5): 689-697.
-
Eissele R, Göke R, Willemer S, Harthus HP, Vermeer H, et al. (1992) Glucagon-like peptide-1 cells in the gastrointestinal tract and pancreas of rat, pig and man. Eur J Clin Invest 22(4): 283-291.
-
Herrmann C, Göke R, Richter G, Fehmann HC, Arnold R, et al. (1995) Glucagon-Like Peptide-1 and Glucose- Dependent Insulin-Releasing Polypeptide Plasma Levels in Response to Nutrients. Digestion 56(2): 117-126.
-
www.fda.gov/medwatch.
-
Holst JJ, Deacon CF (2005) Glucagon-like peptide-1 mediates the therapeutic actions of DPP-IV inhibitors. Diabetologia 48(4): 612-615.
-
Astrup A, Rössner S, Van Gaal L, Rissanen A, Niskanen L, et al. (2009) Effects of liraglutide in the treatment Copyright© Reema Kashiva, et al. of obesity: a randomised, double-blind, placebo- controlled study. Lancet 374(9701): 1606-1616.
-
Kesavadev J, Shankar A, Krishnan G, Jothydev S (2012) Liraglutide therapy beyond glycemic control: an observational study in Indian patients with type 2 diabetes in real world setting. Int J Gen Med 5: 317- 322.
-
Sanyal D, Majumdar A (2013) Low dose liraglutide in Indian patients with type 2 diabetes in the real world setting. Indian J Endocrinol Metab pp: S301-S303. Reema Kashiva, et al. Effect of Liraglutide on Weight Reduction in Euthyroid, Non Diabetic Obese Patients. Diabetes Obes Int J 2019, 4(3): 000204.
-
Kesavadev J, Shankar A, Gopalakrishnan G, Jothydev S (2015) Efficacy and safety of liraglutide therapy in 195 Indian patients with type 2 diabetes in real world setting. Diabetes Metab Syndr Clin Res Rev 9(1): 30- 33.
-
Verma A (2012) Non-diabetic use of liraglutide. Indian J Endocrinol Metab 16(5): 864-865.
-
Anirban M, Soumyabrata R, Debmalya S, Bhattacharjee K (2018) Liraglutide-Indian experience. Indian J Endocrinol Metab 22(6): 818- 826. Copyright© Reema Kashiva, et al.
- Investigation of Polymorphisms in PPAR-Ɣ and TRHR Genes and their Impact on Turkish Diabetic and Obese Individuals
- The Impact of Aircraft Noise Exposure on the Efficacy of Empagliflozin Therapy in an Animal Model of Obesity
- Rooibos Mitigates Metabolic and Inflammatory Dysfunctions in Mice Fed a High-Carbohydrate Diet
- Synergistic Effect of Combined Leaf Extract of Vernonia amygdalina, Ocimum gratissimum, and Zingiber officinale Tuber on Phytochemical Profile, Antioxidant Activity, Serum Insulin, and Biochemical Parameters in Streptozotocin-Induced Diabetic Rats
- Investigation of Cardiovascular Responses to Aerobic Exercise in Obese University Students
- A Look at the Phase Angle Obtained by Electrical Bioimpedance