The Level of Knowledge and Practice of Secondary Prevention among Type 2 Diabetes Mellitus Patients at Selected Healthcare Facilities in Meru County, Kenya
Diabetes mellitus (DM) is a chronic metabolic disease of multiple etiologies that results from a deficit in insulin production, insulin action or both. Diabetes affects millions of people globally and is among the chronic diseases that take a huge toll on human health as well as resources, and regardless of this, the condition continues to face neglect by individuals, communities and states. The disorder is associated with significant disability, premature deaths and enormous medical costs often resulting from the chronic complications. Chronic complications of diabetes result from inadequate secondary revention practices and they include both micro-vascular and macro-vascular complications affecting the kidneys, eyes, neurons, heart, and the circulation. Upon diagnosis with T2DM, secondary preventive practices are fundamental in the prevention of the occurrence of chronic complications. However, inadequate knowledge on these measures among the patients and healthcare providers has been indicated as a major reason for the development of complications. Thus, the study sought to assess the level of knowledge and practice of the secondary prevention among patients with type 2 diabetes mellitus at Consolata Nkubu and Meru Level Five Hospital in Meru County. A descriptive correlational study design was adopted to collect data from 357 purposively sampled participants with T2DM using questionnaires and Focus Group Discussion Guide. Quantitative data was analyzed at 95% confidence interval and a significance level p≤0.05. Most respondents had T2DM for 5-10 years and the main co-morbidity that affected 79% of the respondents was hypertension. The last BP measurements for most respondents was >140/90mmHg and blood glucose level of >7.8mmol/L with 53.7% having a BMI score of more than 25kg/m2. Concerning secondary prevention 70.6% (n=250) did foot examination during every visit, 56.5% (n=200) had their eyes examined annually, 26% (n=92) had urine checks annually, 18.9% (n=67) had body cholesterol level check-up regularly and 69.5%(n=246) had regular blood pressure monitoring. The mean score was 48.3% and SD was 30.1. Most respondents had overall poor knowledge of prevention practices. Knowledge level significantly influenced T2DM secondary prevention at a p value ≤0.05. Measures to improve the knowledge and practice of secondary prevention should be instigated.
Introduction
Diabetes mellitus (DM) is a chronic metabolic disease of multiple etiologies that results from a deficit in insulin production, insulin action or both [1]. Diabetes is classified into two primary classes that are Type 1 diabetes, also referred to as juvenile onset diabetes or insulin-dependent diabetes mellitus (IDDM). This type of DM accounts for 5 percent to 10 percent of all DM diagnosed cases. Risk factors are less well defined for Type 1 DM as compared to Type 2 DM. Among the defined risk factors for Type 1 DM include autoimmune disorders, genetic predisposition, defects as well as environmental factors. On the other hand, Type 2 DM also referred to as adult onset DM or non-insulin- dependent diabetes mellitus (NIDDM) is responsible for 90 percent to 95 percent of all DM diagnosed cases [2, 3]. Risk factors for T2DM include genetic predisposition, advanced age, overweight and obesity, impaired glucose tolerance, sedimentary lifestyle, and race or ethnicity. Another type of DM gestational diabetes usually develops in 2 percent to 5 percent of pregnant women but often disappears when the pregnancy is over is considered the third type of DM [4].
Complications of T2DM are classified into two categories; acute complications and chronic complications [2]. The hyperglycemic state in T2DM leads to long lasting damage of various body organs that is; the eyes, nerves, blood vessels and kidneys in approximately a third to a half of the individuals diagnosed with the condition [5]. Poorly controlled T2DM is associated with an array of neuropathic, macro vascular and micro vascular complications. Macro vascular complications entail peripheral vascular diseases, cardiovascular diseases (CVD) and coronary artery ailments while the micro vascular complications include neuropathic, renal and retinal diseases [5, 6].
Chronic complications of DM can be controlled effectively through the diabetic secondary preventive measures that include eye examinations, cardiovascular care, kidney care and foot care. However, these services are underutilized due to inadequate knowledge [7]. Among patients with type 1 or type 2 diabetes mellitus improvements in glycaemic control and adoption of secondary measures significantly reduces the incidences and the cost of macro vascular and, micro vascular complications [8, 9]. This provides clear evidence for support of prioritized and sustained measures during early diabetes diagnosis to prevent the development of diabetes complications [8].
Asia has been identified as a major continent of the rapidly emerging T2DM, with India and China the top two epicentres. Although genetics significantly determines a person’s susceptibility to T2DM, a sedimentary lifestyle coupled with unhealthy diet and lack of exercise are crucial drivers of the current global disease epidemic [10]. The situation is not different in Africa where diabetes mellitus poses a significant health and socio-economic challenge in the continent, a continent facing simultaneously other healthcare problems that include infectious diseases such as HIV, respiratory infections such as tuberculosis, and malaria. In the Africa continent, the number of individuals ailing from the disease is at 14.2 million. This number is expected to double to 34.2 million by the year 2040 implying that diabetes mellitus is a common chronic disease with an escalating prevalence globally [11]. The burden of T2DM complications and comorbidity is substantial among sub- Saharan African [12]. Kenya being one of the sub-Saharan African countries is no exception to these challenges. The largest burden of diabetes mellitus results from the chronic complications, yet a majority of the individuals suffering from the ailment lack inadequate knowledge on diabetes and the secondary preventive approaches thus, end up not utilizing the services [7, 13]. Therefore, the study sought to assess the level of knowledge and practice of the secondary prevention among patients with type 2 diabetes mellitus at Consolata Nkubu and Meru Level Five Hospital in Meru County.
Methodology (Materials and Methods)
The study was conducted at two selected healthcare facilities that is: Consolata Hospital Nkubu a private hospital and Meru Level Five Hospital a public based facility both in Meru County. The design employed was a descriptive correlational study with an aim of assessing the level of knowledge and practice of the secondary prevention among patients with type 2 diabetes mellitus at Consolata Nkubu and Meru Level Five Hospital in Meru County. A total of 357 participants were involved in the study where data was collected using interviewer administered questionnaires and focus group discussion guide.
Purposive sampling method was used to sample type 2 DM patients in both hospitals. Stratified sampling was then used to get both representation of men and women in the study. Simple random sampling was then used to get the actual respondents as they attended diabetic clinic. Data collection was done as the T2DM patients attended their diabetic clinic for a period of two months. The researcher sought permission for conducting the research from National Commission for Science, Technology and Innovation (NACOSTI) through the Chuka University Ethics and Research Committee for review and approval. Permission was also sought from Consolata Hospital Nkubu and Meru Level Five Hospital prior to data collection. Quantitative data was cleaned, coded and analyzed at a significance p≤0.05. Frequencies and percentages were used to describe the quantitative data. Chi squares was used to test the relationship between variables of association at
95% significance level. For qualitative analysis, data was categorized into emerging themes and analyzed using N-Vivo Version 11. The study results were presented inform of bar graphs, narrations, tables, and pie charts.
Results
Table 1 presents demographic characteristics of the respondents. Table 1 shows that 117 (33.1%) had been sick for less than 5 years, 125 (35.3%) had been sick for 5-10 years and 112 (31.6%) had been sick for more than 10 years. Concerning diabetes co-morbidities, 283 (79.9%) had hypertension, 8 (2.3%) had asthma, 4 (1.1%) had heart failure and 59 (16.7%) had no co-morbidities. The body mass indices ranged from 18 to greater than 30 whereby, 164 (46.3%) had BMI of 18-24, 166 (46.9%) had BMI of 25-29 while 24 (6.8%) had BMI of over 30kg/m2.
| Frequency (n) | Percentage (%) | |
|---|---|---|
| Duration of illness | ||
| Less than 5 years | 117 | 33.1 |
| 5-10 years | 125 | 35.3 |
| More than 10 years | 112 | 31.6 |
| Total | 354 | 100 |
| Co-morbidities | ||
| Hypertension | 283 | 79.9 |
| Asthma | 8 | 2.3 |
| Heart failure | 4 | 1.1 |
| 59 | 16.7 | |
| Total | 354 | 100 |
| BMI(Kg/M2) | ||
| 18-24 | 164 | 46.3 |
| 25-29 | 166 | 46.9 |
| 30 and above | 24 | 6.8 |
| Total | 354 | 100 |
| Last BP measurement (mmHg) | ||
| 100/60-130/80 | 74 | 20.9 |
| 131/81-140/90 | 62 | 17.5 |
| Over 140/90 | 218 | 61.6 |
| Total | 354 | 100 |
| Last blood sugar measurement (mmol/L) | ||
| 7.8 and below | 23 | 6.5 |
| Above 7.8 | 331 | 93.5 |
| Total | 354 | 100 |
| Evidence of DM complication | ||
| Leg ulcer | 73 | 20.6 |
| Nerve problem | 1 | 0.3 |
| Renal disease | 2 | 0.6 |
| Eye disease | 6 | 1.7 |
| Cardiovascular disease | 209 | 59 |
| Arthritis | 1 | 0.3 |
| 62 | 17.5 | |
| Total | 354 | 100 |
| Harmful social habits | ||
| Cigarette smoking | 51 | 14.4 |
| Harmful alcohol use | 11 | 3.1 |
| Both smoking and alcohol use | 11 | 3.1 |
| 281 | 79.4 | |
| Total | 354 | 100 |
Table 1: The demographic characteristics.
Concerning the last blood pressure measurements, 74 (20.9%) had a BP of between 100/60-130/80mm/Hg, 62 (17.5%) had BP of between 131/81-140/90 mm/Hg and 218 (61.6%) had BP of over 140/90mm/Hg. Most respondents i.e. 330 (93.2%) had the last blood glucose levels above 7.8 mmol/L while 23 (6.5%) had 7.8 mmol/L and below.
After assessing the respondents for any evidence of DM complications, 73 (20.6%) were found to have leg ulcers, 1(0.3%) had nerve problems, 2 (0.6%) had renal disease, 6 (1.7%) had eye disease, 209 (59%) had cardiovascular disease, 1 (0.3%) had arthritis and 62 (17.5%) did not have evidence of any complication. With regard to harmful social habits, 51 (14.4%) were cigarette smokers, 11(3.1%) were using alcohol, 11 (3.1%) were using both cigarettes and alcohol while majority i.e. 281 (79.4%) did not engage in any harmful social habits.
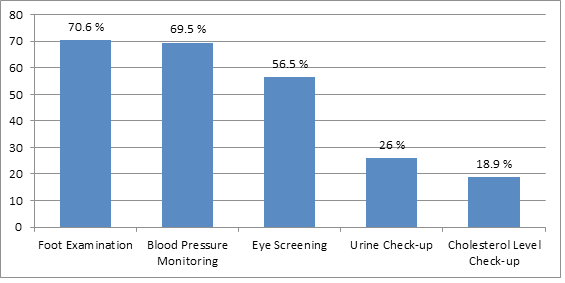
Secondary Preventive Measures Practiced among Patients
Figure 1 illustrates the various secondary preventive measures sought by the respondents. Figure 1 shows that 70.6% (n=250) of the respondents did foot examination during every visit to the clinic, 56.5% (n=200) had their eyes examined annually, 26% (n=92) had urine checks annually, 18.9% (n=67) had body cholesterol level check-up regularly and 69.5% (n=246) had regular blood pressure monitoring. The mean score was 48.3% and SD was 30.1.
Level of Practice of Secondary Preventive Measures
The level of practice was determined by the number of practice items that respondents adhered to. Figure 2 illustrates the secondary prevention practice level. Those respondents who adhered to at least three items were considered to have good secondary prevention practice while those who adhered to less than three were considered to have poor secondary prevention practice.
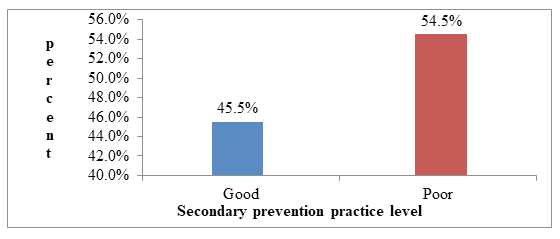
Figure 2 shows that 45.5% (161) had good secondary prevention practice while 54.5% (193) had poor secondary prevention practice. The level of practice was the dependent variable in this study and all independent variables were cross-tabulated against it to check for any statistical significance.
Knowledge on Secondary Prevention Practice among Respondents
Knowledge was assessed through a set of six knowledge items, and based on the responses given; they were categorized as either “correct response” or “incorrect response”.
Table 2 shows that only 2.3% (n=8) understood what secondary prevention practices were all about. Most of them were talking about living positively with DM and general management of diabetes rather than secondary prevention. Majority of the respondents i.e. 97.2% (n=344) knew the complications of DM, 45.8% (n=162) knew how frequent eye check-ups should be done, 33.1% (n=117) knew how frequent urine check-ups should be done, 53.7% (n=190) knew the importance of regular blood pressure check-ups and 54.8% (n=194) knew that cholesterol levels should be checked regularly. The mean score was 47.8% and standard deviation was 26.4.
| Knowledge Item | Correct Response (%) |
| What is your understanding of self-care secondary prevention practices? | 2.30% |
| Which complications are associated with diabetes? | 97.20% |
| How frequent should you go for eye check-up? | 45.80% |
| How frequent should you go for urine check-up? | 33.10% |
| Why do you think it is necessary to have regular blood pressure check-up? | 53.70% |
| Do you think diabetic patients should have their cholesterol levels checked? | 54.80% |
| Mean score | 47.80% |
| Standard deviation | 26.4 |
Table 2: Knowledge on secondary prevention practice of diabetes complications.
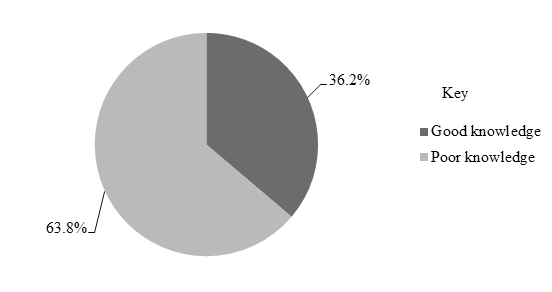
General Level of Knowledge on Secondary Preventive Measures
Knowledge level was determined based on the number of items respondents answered correctly, whereby, those who answered at least 4 items correctly were considered as having good knowledge while those who answered 3 items and below correctly were considered as having poor knowledge.
Figure 3 show that 36.2% (n=128) had good knowledge of secondary preventive practices while 63.8% (n=226) had poor knowledge. It is evident that majority of the respondents knew what diabetes is, and its complications.
However, less than half of the respondents had the knowledge on secondary preventive measures for diabetic complications. This squarely affected the level of practice of the secondary preventive measures for diabetic mellitus type 2 complications.
Influence of Knowledge on Diabetic Secondary Prevention Practice
Knowledge level was cross-tabulated against the practice levels and chi squared tests performed.
Table 3 shows that knowledge significantly influenced the practice level for DM secondary prevention (χ2 (1, N=354) =63.20, p=<0.001, OR=6.56) whereby, those with good knowledge were 6.561 times more likely to practice secondary prevention. Therefore, the level of knowledge had statistical significance on practice of the secondary prevention among patients with type 2 diabetes mellitus at Consolata Nkubu and Meru Level Five Hospital in Meru County.
| Good vs poor knowledge | Total | ||
|---|---|---|---|
| Total | Good knowledge | Poor knowledge | |
| DM complications | 94 | 67 | 161 |
| secondary prevention practice | 34 | 159 | 193 |
| Total | 128 | 226 | 354 |
Table 3: ** Association between knowledge and secondary prevention practice.
χ2 (1, N=354) = 63.2, p=0.000. Table 3: Association between knowledge and secondary prevention practice.
Discussion
In this study, having good knowledge on the specific secondary preventive measures for diabetic complications was associated with good practice of the measures. This is supported by Herath, et al. (2017) who states that increased awareness of diabetes is a major determinant for the prevention of diabetes related complications [14]. Unfortunately, the proportion with good knowledge was less than half of the respondents. This clearly indicates that most of the T2DM patients in Meru County have knowledge deficit on secondary preventive measures for diabetic complications. The respondents knew about the complications but lacked in-depth knowledge on the prevention of the complications indicating a need for strengthening knowledge especially on the secondary preventive measures in DM care. These results agree with the findings of a study done in Ghana where the respondents knew individual complications of T2DM, which included; heart disorders, eye disease, foot ulceration, arousal disorder, neuropathy, and renal disease. The same study reported that the respondents had a deficit in knowledge on specific measures to be taken in prevention of diabetic complications [15].
The results in this study are also in line with another study conducted in Saudi Arabia, where the diabetic patients had diabetic complications and were aware of the complications but had little knowledge on prevention of the complications as evidenced in the research study. This was reported in a study on awareness of diabetic mellitus complications and perceived knowledge on the complications in Saudi Arabia [16, 17]. Positive attitude, knowledge, as well as practice are all critical for DM patients in the utilization of the secondary preventive approaches. Newly diagnosed type 2 diabetes patients who don’t receive proper diabetes education on the secondary preventive approaches have poor knowledge on these DM approaches leading to poor practice. Insufficient knowledge as well as inadequate DM secondary preventive is associated with the development of diabetes mellitus complications [7]. In assisting patients to live a positive, productive life, structure educational programs on DM and measures to prevent complications are vital.
In the current study in Meru County, 45.8% of the patients had knowledge on diabetic retinopathy (DR), this was less than average. Similar results were revealed in a study on diabetes retinopathy in St Elizabeth clinic in Jamaica. The patients from the study had moderate knowledge on diabetic retinopathy and positive attitude towards the importance of diabetic care practices. However, in this study patients’ attitude was not assessed [18]. In Ethiopia, a study on diabetic complications among adult DM patients of a tertiary healthcare center showed high prevalence of diabetic complications (59.7%) which were associated with non-compliance to medication. These results differ with the findings of the current study. This may be due to assumptions made in the current study that the patients were compliant to medication [19].
Conclusion
The level of knowledge was poor because the mean score was 47.8% which meant that a lot was yet to be learnt by the respondents. Knowledge was the main predictor of secondary prevention practice. In addition, the level of secondary prevention was poor since the mean score was 48%.
Recommendation
- In averting the burden posed by DM, massive public education on secondary preventive measures for diabetes complications to be done by healthcare workers to enhance the patient practice and level of knowledge.
- Patients to be educated on the ways of preventing chronic complications when they visit the diabetes clinic.
- The government of Kenya, through the county government, to establish diabetic support groups in all hospitals to boost the management of diabetes.
References
-
IDF (2017) IDF Diabetes Atlas, 10th (Edn.), International Diabetes Federation, Brussels.
-
Brunner LS, Smeltzer SCOC (2010) Brunner & Suddarth’s textbook of medical- surgical nursing. Wolters Kluwer Health/Lippincott Williams & Wilkins, Philadelphia.
-
WHO (2016) Global report on diabetes. World Health Organization, Geneva.
-
Chatterjee S, Khunti K, Davies MJ (2017) Type 2 diabetes. The Lancet 389(10085): 2239-2251.
-
Gray SP, Jandeleit-Dahm K (2014) The pathobiology of diabetic vascular complications-cardiovascular and kidney disease. J Mol Med (Berl) 92(5): 441-452.
-
Alaboud AF, Tourkmani AM, Alharbi TJ, Alobikan AH, Abdelhay O, et al. (2016). Microvascular and macrovascular complications of type 2 diabetic mellitus in Central, Kingdom of Saudi Arabia. Saudi medical journal 37(12): 1408-1411.
-
Rahaman KS, Majdzadeh R, Holakouie Naieni K, Raza O (2017) Knowledge, Attitude and Practices (KAP) regarding chronic complications of diabetes among patients with type 2 diabetes in Dhaka. Int J Endocrinol Metab 15(3): e12555.
-
Baxter M, Hudson R, Mahon J, Bartlett C, Samyshkin Y, et al. (2016) Estimating the impact of better management of glycaemic control in adults with type 1 and type 2 diabetes on the number of clinical complications and associated financial benefit. Diabetic Medicine 33(11): 1575-1581.
-
Psaltopoulou T, Ilias I, Alevizaki M (2010) The role of diet and lifestyle in primary, secondary, and tertiary diabetes prevention: a review of meta-analyses. Rev Diabet Stud 7(1): 26-35.
-
Zheng Y, Ley SH, Hu FB (2018) Global aetiology and epidemiology of type 2 diabetes mellitus and its complications. Nat Rev Endocrinol 14(2): 88-98.
-
IDF (2015) IDF Diabetes Atlas, 7th (Edn.), International Diabetes Federation, Brussels.
-
Ekoru K, Doumatey A, Bentley AR, Chen G, Zhou J, et al. (2019) Prevalence and risk factors for type 2 diabetes complications and comorbidity in Sub-Saharan Africans. E Clinical Medicine 16: 30-41.
-
Wu Y, Ding Y, Tanaka Y, Zhang W (2014) Risk factors contributing to type 2 diabetes and recent advances in the treatment and prevention. Int J Med Sci 11(11): 1185-1200.
-
Herath HMM, Weerasinghe NP, Dias H, Weerarathna TP (2017) Knowledge, attitude and practice related to diabetes mellitus among the general public in Galle district in Southern Sri Lanka: a pilot study. BMC Public Health 17(1): 535.
-
Obirikorang Y, Obirikorang C, Anto EO, Acheampong E, Batu EN, et al. (2016) Knowledge of complications of diabetes mellitus among patients visiting the diabetes clinic at Sampa Government Hospital, Ghana: A descriptive study. BMC Public Health 16(1): 637.
-
Fatani E, Gari L, Alharbi A, Alzahrani A, Almasoudi A, et al. (2018) Awareness of diabetic complications, perceived knowledge, compliance to medications and control of diabetes among diabetic population of Makkah city, Kingdome Saudi Arabia. The Egyptian journal of hospital medicine 70(7): 1190-1195.
-
Menezes S, Bava M, Roshan M (2015) A study on awareness of diabetic complications among type 2 diabetes patients. IOSR journal of dental and medical sciences 14(11): 13-16.
-
Zahra M (2015) Knowledge, attitude & practices on diabetes and diabetic retinopathy in st Elizabeth, Jamaica. World Diabetes Fedration.
-
Abejew A, Belay A, Kerie M (2015) Diabetic complications among adult diabetic patients of a tertiary hospital in Northeast Ethiopia. Hindawi journal 2015: 290920.
- Investigation of Polymorphisms in PPAR-Ɣ and TRHR Genes and their Impact on Turkish Diabetic and Obese Individuals
- The Impact of Aircraft Noise Exposure on the Efficacy of Empagliflozin Therapy in an Animal Model of Obesity
- Rooibos Mitigates Metabolic and Inflammatory Dysfunctions in Mice Fed a High-Carbohydrate Diet
- Synergistic Effect of Combined Leaf Extract of Vernonia amygdalina, Ocimum gratissimum, and Zingiber officinale Tuber on Phytochemical Profile, Antioxidant Activity, Serum Insulin, and Biochemical Parameters in Streptozotocin-Induced Diabetic Rats
- Investigation of Cardiovascular Responses to Aerobic Exercise in Obese University Students
- A Look at the Phase Angle Obtained by Electrical Bioimpedance