Comparison of Clinical Characteristics and Outcomes between Outpatients and Hospitalized Patients with Diabetes and COVID-19
Background: Patients with diabetes and COVID-19 have higher rates of complications. Objective: To describe and identify the characteristics and outcomes in patients with diabetes and COVID-19. Methods: From March to June 2020, we included patients with diabetes and probable COVID-19 infection. We compared parameters between outpatients and hospitalized patients. A second analysis compared patients who died vs those who survived. Results: 243 patients, 37.6% women, with 56 ±12 years, and BMI 29.6 ±5.3 kg/m2 were included. Risk factors for hospitalization were oximetry <90% (HR 2.29, 95%CI 1.14-4.58) and mean blood pressure (MBP) <80 mmHg (HR 1.75, 95%CI 1.09-2.81). Age (HR 0.93, 95%CI 0.89-0.97), respiratory rate (RR) (HR 1.05, 95%CI 1.00-1.10) and PaFiO2 (HR 0.99, 95%CI: 0.98-1.00) predicted admission to critical areas. Risk factors for mortality were age ≥65 years (HR 2.88, 95%CI 1.61-5.17), RR ≥25 bpm (HR 3.86, 95%CI 1.33-11.12), heart rate (HR 1.82, 95%CI 0.96-3.42), PaFiO2 <100 (HR 3.70, 95%CI 1.06-6.65) and glucose ≥150 mg/dl (HR 2.57, 95%CI 1.05-6.25). Length of hospitalization was 8.5 (6-14) and 6 (2-10) days for discharged and deceased patients (p=0.003), respectively. Conclusion: Oximetry <90% and MBP <80 mmHg were associated with hospitalization requirement. Glucose concentration >150 mg/dl significantly predicted mortality.
Introduction
Prevalence of diabetes in COVID-19 cases ranges from 16 to 33%. The need for hospitalization, intensive care unit (ICU) admission, ventilatory mechanical support and mortality is higher in these patients [1, 2, 3, 4, 5, 6, 7]. Immune dysfunction associated with diabetes might play a role [8, 9]. In addition, comorbidities associated may explain the greater morbidity and mortality. The coexistence of obesity, hyperglycemia at admission, diagnosis of diabetes before 40 years and presence of chronic cardio-renal complications are among the variables associated with a worse prognosis [10, 11, 12, 13]. However, the contribution of diverse diabetes associated factors for having adverse outcomes is not consistent [14, 15, 16, 17]. Discordance may be caused by methodological issues (i.e., retrospective reports) or by the inclusion of heterogeneous samples [18].
Given the current unprecedented situation, prospectively collected data are needed in specific populations. Therefore, the aim of this work is to describe the characteristics associated with the need of hospitalization, admission to critical areas and mortality in patients with diabetes and COVID-19 in a reference center in Mexico City.
Materials and Methods
We included patients with diabetes that seek medical attention at the Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán (INCMNSZ) in Mexico City with possible COVID-19 infection from March 1 to June 30, 2020. We registered information regarding socio-demographic data, symptoms, treatment, and comorbidities. We also registered blood pressure, respiratory rate, heart rate, oximetry, and body mass index (BMI). Patients were divided into those who received outpatient treatment and those who required hospitalization. In hospitalized patients and some of the outpatients, biochemical variables were also recorded including glucose concentration, creatinine, blood urea nitrogen (BUN), complete blood count, liver enzymes, c reactive protein (CRP), lactate dehydrogenase (LDH), ferritin, creatinine phosphokinase (CPK), D-dimer, prothrombin time, troponin I and 25-OH vitamin D. In addition, treatment for COVID-19, antihypertensives and insulin doses were registered. Lung computed tomography (CT) was performed to assess the severity of lung involvement. We recorded whether PCR for COVID-19 was performed and the result.
In hospitalized patients, follow-up was performed, and information was recovered from medical registries. Patients who were not hospitalized were contacted by phone approximately two weeks after attending the Emergency Room for a follow-up evaluation to record outcomes of the COVID-19.
The protocol was approved by the Institute’s Clinical Research Committee and the Research Ethics Committee (reference 3362) and participants gave their informed consent.
Statistical Analysis
Continuous variables with parametric distribution are expressed as mean (±SD) or with medians and interquartile ranges (25-75) in those with non-parametric distribution, according to the Kolmogorov-Smirnov test. Categorical variables are presented as frequencies with their respective percentages. To assess differences among groups we used T tests for independent variables and categorical variables were compared using X2 tests.
We compared outpatients and hospitalized patients to identify factors associated with the need for hospitalization. Additionally, we compared the variables between patients who survived and those who died. The associated factors for a positive COVID-19 test, hospitalization, need for ICU admission, and death were identified with logistic regression analyses adjusting for sex, age, and time since diabetes diagnosis. Statistical analyses were performed using SPSS Statistics (IBM, version 25) and p-value ≤0.05 was considered as statistically significant.
Results
Study Population
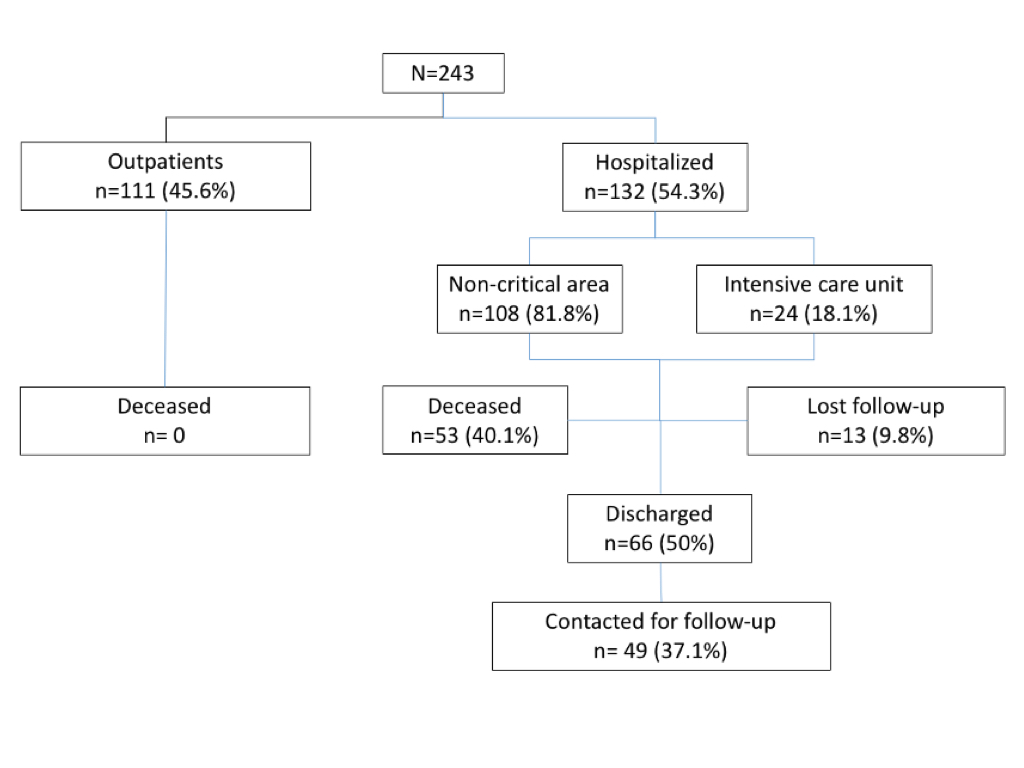
We included 243 patients with diabetes who attended the emergency department with COVID-19 symptoms. Figure 1 shows the patient flow for inclusion and follow- up. The mean age of patients was 56±12 years, 37.6% were women, time since diabetes diagnosis was 10 (5-16) years, and the BMI 29.6±5.3 kg/m2. Three patients (2.27%) were diagnosed with type 2 diabetes at hospitalization. In addition, 3 hospitalized patients and one outpatient had type 1 diabetes mellitus (T1DM).
Forty nine percent of the patients reported a positive COVID-19 contact. The most frequent symptoms were cough (72.4%), fever (68.7%) and dyspnea (64.6%); 4.5% of the patients who were sent home referred to be asymptomatic. The main comorbidities reported were hypertension (43.2%), dyslipidemia (27.6%) and nephropathy (14.8%). Current smoking was reported in 18.1% of patients.
Overall, 45.6% (n=111) were treated as outpatients, while 54.3% (n=132) were hospitalized. Twenty-four patients (18.1%) required management in the ICU and mechanical intubation of whom 50% recovered and 50% died.
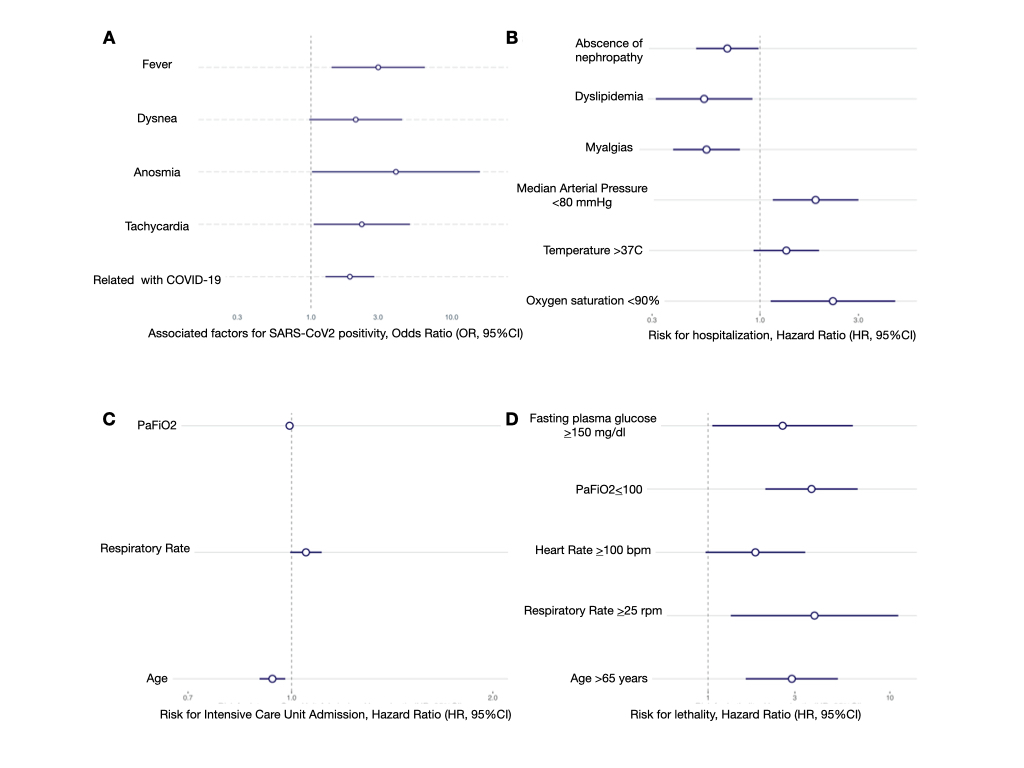
Most hospitalized patients (80.3%) had a positive swab test vs 60.4% of outpatients (p=0.002). In the hospitalized patients with a negative swab test (19.7%) a second test was positive in 42.9%. Associated factors for a positive COVID-19 test were fever (OR 3.00, 95%CI 1.41-6.54), dyspnea (OR 2.08, 95%CI 0.98-4.50), anosmia (OR 4.01, 95%CI 1.14- 19.27), tachycardia (OR 2.29, 95%CI 1.05-5.13) and contact with a confirmed case (OR 1.89, 95%CI 1.32-2.94) (Figure 2A).
Characteristics of Hospitalized and Outpatients
Table 1 shows the characteristics in outpatients and hospitalized patients. The BMI was not different among groups (29.1±7.3 vs 30.1±8 kg/m2, p=0.13). None of the hospitalized patients was asymptomatic whereas 4.5% of the patients sent home referred to be asymptomatic (p=0.01). Twenty-four patients (9.8%) without referring dyspnea as a symptom had low oximetry (<90%), with a mean of 87% (54-89). Smoking status was similar in both groups (21.6 vs 15.2%, p=0.24). Time since diabetes diagnosis was higher in hospitalized patients compared to outpatients (p= 0.06). Supplementary Table I shows the educational level and occupation in both groups. The comorbidities in both groups are shown in table II. Most of the patients who required hospitalization were men, with a higher age and lower educational level. The days since the onset of COVID-19 symptoms were almost twice, and presented with a higher heart rate, respiratory rate, temperature, and lower oximetry compared with outpatients. Risk factors associated with the need for hospitalization were oximetry <90% (HR 2.29, 95%CI 1.14-4.58), mean arterial pressure <80 mmHg (HR 1.75, 95%CI 1.09-2.81) while myalgias (HR 0.56, 95%CI 0.39- 0.81), dyslipidemia (HR 0.52, 95%CI 0.30-0.90) and absence of nephropathy (HR 0.70, 95%CI 0.50-0.99) were protective factors (Figure 2B). The overall length of hospitalization was 8 days (4-12).
| Outpatient N= 111 | Hospitalized N= 132 | p | |
|---|---|---|---|
| Men | 56 (50.4) | 95 (71.9) | 0.001 |
| Age (years) | 54.01 ± 12 | 57.8 ± 12 | 0.013 |
| Time since diagnosis of diabetes (years) | 7 (4-15) | 10 (5-18) | 0.065 |
| Smoking | 24 (21.6) | 20 (15.2) | 0.24 |
| Days with symptoms | 4 (2-7) | 8 (5.2-18) | <0.001 |
| Symptoms | |||
| - Fever | 64 (57.7) | 103 (78) | 0.001 |
| - Cough | 67 (60.4) | 132 (100) | <0.001 |
| - Headache | 49 (44.1) | 64 (48.9) | 0.518 |
| - Dyspnea | 37 (33.3) | 120 (90.9) | <0.001 |
| - Chest pain | 14 (12.6) | 22 (16.7) | 0.469 |
| - Anosmia | 18 (16.2) | 11 (8.3) | 0.074 |
| - Myalgias / arthralgias | 60 (54.1) | 64 (48.5) | 0.44 |
| - Asthenia / adynamia | 16 (14.4) | 48 (36.4) | <0.001 |
| - Diarrhea | 17 (15.5) | 22 (16.8) | 0.861 |
| - Without symptoms | 5 (4.5) | 0 | |
| Weight (kg) | 76.5 ± 16.7 | 80.1 ± 15 | 0.082 |
| Body mass index (kg/m2) | 29.1 ±5.2 | 30.1 ± 5.15 | 0.135 |
| Systolic blood pressure (SBP) (mmHg) | 131.3 ± 18.2 | 125.9 ± 17.1 | 0.019 |
| Diastolic blood pressure (DBP) (mmHg) | 78.8 ± 13.0 | 74.1 ± 12.3 | 0.005 |
| Heart rate (beats/minute) | 95.7 ± 16.9 | 105.6 ± 16 | <0.001 |
| Respiratory rate (breaths/minute) | 21.8 ± 5.6 | 31.05 ± 7.7 | <0.001 |
| Temperature (°C) | 36.7 ± 0.8 | 37.0 ± 0.8 | 0.004 |
| Oximetry (%) | 91.5 ± 5.1 | 71.7 ± 16.3 | <0.001 |
| Basal drug therapy | |||
| - Metformin | 88 (79.3) | 98 (74.8) | 0.447 |
| - Sulphonylurea | 22 (19.8) | 38 (29) | 0.099 |
| - Insulin | 37 (33.3) | 51 (38.9) | 0.367 |
| - DPP-4 inhibitor | 9 (8.1) | 13 (9.9) | 0.624 |
| - SGLT-2 inhibitor | 9 (8.1) | 2 (1.5) | 0.026 |
| - GLP1 agonist | 2 (1.8) | 2 (0.8) | 0.211 |
| - Thiazolidinedione | 7 (6.3) | 3 (2.3) | 0.118 |
| - Angiotensin converting enzyme inhibitors (ACEi) | 16 (14.4) | 19 (14.4) | 1 |
| - Angiotensin-II receptor antagonist (ARA) | 24 (21.6) | 29 (22) | 1 |
| - Calcium channel blockers | 10 (9) | 12 (9.1) | 1 |
| - Beta blockers | 6 (5.4) | 6 (4.5) | 0.775 |
| - Diuretics | 12 (10.8) | 13 (9.8) | 0.806 |
Table 1: Characteristics of patients with diabetes and COVID-19 in outpatient versus hospitalized patients. Data expressed as n (
Complementary studies were performed in 21 patients (18.9%) before deciding on their outpatient treatment. BUN, creatinine, AST, CRP, DHL, ferritin, CPK, D-dimer and troponin were higher while albumin, 25-OH vitamin D and lymphocytes were lower in hospitalized vs outpatients (Table 2).
We analyzed the differences in parameters between women and men, where significant differences were observed. These results are shown in Supplementary Table II.
| Outpatient N=111 | Hospitalized N=132 | p | |
|---|---|---|---|
| Comorbidities | |||
| Obesity | 42 (37.8) | 60 (45.8) | 0.24 |
| Overweight | 44 (39.6) | 50 (37.8) | 0.473 |
| Dyslipidemia | 50 (45) | 17 (12.9) | <0.001 |
| Hypertension | 44 (39.6) | 61 (46.2) | 0.363 |
| Hepatic steatosis | 24 (21.6) | 2 (1.5) | <0.001 |
| Nephropathy | 10 (9) | 16 (12.3) | 0.004 |
| Neuropathy | 6 (5.4) | 13 (9.9) | 0.235 |
| Retinopathy | 6 (5.4) | 14 (10.7) | 0.002 |
| Stroke | 0 | 2 (1.51) | |
| Cardiovascular disease | 7 (6.3) | 8 (6.3) | 0.874 |
| Peripheral artery disease | 0 | 1 (0.75) |
Table 2: Comorbidities in outpatients and hospitalized patients.
There were 24 patients who required hospitalization in ICU (18.1%), with a stay of 13.5 days (6.5-17.2). Age (HR 0.93, 95%CI 0.89-0.97), respiratory rate (HR 1.05, 95%CI
1.00-1.10) and lower PaFiO2 (HR 0.99, 95%CI 0.98-1.00) were factors associated with admission to ICU (Figure 2C).
The CT performed at admission reported severe involvement in 78 patients (65.5%), moderate in 35 (28.6%), and mild involvement in 6 (5%) patients. Treatment in hospitalized patients included hydroxychloroquine in 24 (20.2%), low molecular weight heparin in 94 (79%), and total anticoagulation in 18 (15.1%). Antihypertensive drugs were indicated in 12 (10.1%) patients. Thirty-six (30.3%) patients received morphine infusion for dyspnea. The most prescribed antibiotics were azithromycin in 101 (84.9%), amoxicillin/clavulanate in 51 (42.9%), cephalosporins in 39 (32.8%), piperacillin/tazobactam in 30 (25.2%), and vancomycin in 24 (20.2%) patients.
Outcomes
In this population, 44.6% (n=53) of hospitalized patients died. Clinical and biochemical characteristics of survivors and deceased patients and survivors are shown in Tables 3, 4 & 5 and Supplementary Table III. There were no differences at admission in hemoglobin, platelet count, ALT, alkaline phosphatase, prothrombin time, and 25-OH vitamin D. In addition, no differences in treatment were observed (Supplementary Table IV). Length of hospitalization was 8.5 (6-14) and 6 (2-10) days (p=0.003), for discharged and deceased patients, respectively.
| Outpatient n=21 | Hospitalized n=132 | P | |
|---|---|---|---|
| Glucose (mg/dl) | 216 (129-277) | 221 (157-313.7) | 0.394 |
| BUN (mg/dl) | 13.5 (11.3-19.6) | 21.5 (14-31) | 0.004 |
| Creatinine (mg/dl) | 0.77 (0.68-0.95) | 0.97 (0.77-0.97) | 0.012 |
| Hemoglobin (g/dl) * | 14.4 ± 2 | 15.0 ± 2 | 0.193 |
| Leukocytes (x109/L) | 8.1 (6.0-9.8) | 7.9 (6.2-11.3) | 0.448 |
| Lymphocytes (%) | 15.5 (10.7-18.3) | 8.9 (5.3-14.8) | 0.002 |
| Platelets (x 109/L) | 258 (211.5-329) | 225 (183-305) | 0.274 |
| AST (IU/L) | 31.5 (20.4-51.6) | 43 (33-.62.7) | 0.029 |
| ALT (IU/L) | 30.8 (21.4-51.6) | 32 (22-49.3) | 0.994 |
| Albumin (g/dl) * | 3.8 ± 0.5 | 3.4 ± 0.4 | <0.001 |
| Alkaline phosphatase (IU/L) | 86 (76-125) | 95 (78-122) | 0.534 |
| C-reactive protein (mg/L) | 10.4 (5.2--13.1) | 18.6 (12.5-26.1) | 0.001 |
| Lactic dehydrogenase (IU/L) | 266 (241-325.5) | 434 (326-546) | <0.001 |
| Ferritin (ng/ml) | 363.5 (211.5-638.3) | 767.5 (392-1300) | <0.001 |
| Creatinine phosphokinase (IU/L) | 62.5 (51.2-85.5) | 118 (56-232.5) | 0.007 |
| D-dimer (ng/ml) | 595 (323.7-1060.7) | 850 (577-1829) | 0.023 |
| Prothrombin time (seconds)* | 11.4 ± 2.5 | 11.5 ± 1.2 | 0.91 |
| Troponin I (ng/ml) | 3.8 (2.1-5) | 7.8 (4.7-26.6) | <0.001 |
| 25-hydroxyvitamin D (ng/ml) | 21.6 (16.1-26.8) | 19.05 (14.7-25.2) | 0.262 |
Table 3: Comparison of biochemical parameters of outpatients and hospitalized patients. All values median, interquartile range, e
| Discharged n=66 | Deceased n=53 | p | |
|---|---|---|---|
| Men n (%) | 43 (65.2) | 42 (79.2) | 0.105 |
| Age (years) | 56.2 ± 11.2 | 59.6 ± 11.7 | 0.113 |
| Scholarship n (%) | |||
| -High School or lower | 36 (54.6) | 36 (43.4) | 0.085 |
| -More than highschool | 30 (45.4) | 16 (32.1) | |
| Time since diabetes diagnosis (years) | 8 (4.7-15) | 10 (5-20) | 0.473 |
| Duration of symptoms (days) | 6 (3-9) | 8 (5-10) | 0.441 |
| PCR COVID-19 test n (%) | |||
| Not done | 1 (0.8) | 3 (5.6) | 0.45 |
| Negative | 7 (10.6) | 6 (11.3) | |
| Positive | 58 (87.7) | 44 (83) | |
| Comorbidities | |||
| - Obesity | 33 (50) | 19 (35.8) | 0.191 |
| - Overweight | 23 (34.8) | 23 (43.9) | 1 |
| - Dyslipidemia | 9 (13.6) | 6 (11.3) | 0.786 |
| - Hypertension | 33 (50) | 23 (43.4) | 0.58 |
| - Hepatic steatosis | 1 (1.5) | 1 (1.9) | 1 |
| - Nephropathy | 7 (10.6) | 6 (11.5) | 0.584 |
| - Neuropathy | 5 (7.6) | 8 (15.4) | 0.239 |
| - Retinopathy | 11 (9.3) | 5 (9.6) | 0.98 |
| - Stroke | 1 (1.5) | 1 (1.9) | 1 |
| - Cardiovascular disease | 4 (6.1) | 3 (5.7) | 0.968 |
| - Peripheral artery disease | 2 (3.0) | 1 (1.9) | 0.661 |
| Weight (kg) | 80.4 ± 13.5 | 78.0 ± 15.8 | 0.372 |
| Body mass index (kg/m2) | 30.6 ± 5.5 | 29.1 ± 5.2 | 0.131 |
| Systolic blood pressure (SBP) (mmHg) | 126.1 ± 14.6 | 124.3 ± 19.7 | 0.592 |
| Diastolic blood pressure (DBP) (mmHg) | 74.9 ± 11.7 | 74.08 ±13.3 | 0.719 |
| Heart rate (beats/minute) | 101.9 ± 14.4 | 110.9 ± 16.6 | 0.002 |
| Respiratory rate. (breaths/minute) | 28.1 ± 7.4 | 34.2 ± 7.2 | <0.001 |
| Temperature (°C) | 36.9 ± 0.7 | 37.1 ± 0.8 | <0.001 |
| Oxygen saturation on admission (%) | 80.7 ± 9.1 | 63.3 ± 17.3 | 0.559 |
| Kirby index (PaO2/FiO2) | 196.4 ± 84.4 | 140.6 ± 86.9 | 0.001 |
Table 4: Clinical and biochemical characteristics of hospitalized patients according to mortality.
| Discharged n=66 | Deceased n=53 | P | |
|---|---|---|---|
| Glucose (mg/dl) | 200 (143.5-272) | 271 (181-334) | 0.001 |
| BUN | 18 (12.1-25) | 24 (16-5.38) | 0.008 |
| Creatinine (mg/dl) | 0.9 (0.7-1.12) | 1.02 (0.84-1.65) | 0.033 |
| Hemoglobin (g/dl) * | 15.1 (13.3-15.8) | 14.9 (13.6-15.9) | 0.088 |
| Leukocytes (x109/L) | 7.1 (5.3-8.5) | 9.6 (7.2-13.9) | <0.001 |
| Lymphocytes (%) | 13.1 (8.5-17.4) | 7.2 (3.9-9.9) | <0.001 |
| Platelets (x 109/L) | 237 (169-308) | 230.5 (185-316) | 0.595 |
| AST (IU/L) | 37 (26-47.4) | 54.5 (37.7-74.9) | <0.001 |
| ALT (IU/L) | 31 (19-44.6) | 34 (23.1-50.6) | 0.115 |
| Albumin (g/dl) * | 3.67 (3.3-3.94) | 3.2 (2.9-3.4) | <0.001 |
| Alkaline phosphatase (IU/L) | 91 (76-114) | 100 (80.5-135) | 0.149 |
| C-reactive protein (mg/L) | 13.9 (8.9-20.9) | 21.7 (13.7-27.9) | 0.028 |
| Lactic dehydrogenase (IU/L) | 329 (264-403) | 543 (422.5-714.2) | <0.001 |
| Ferritin (ng/ml) | 564 (290.4-877) | 939 (389.3-1439) | 0.048 |
| Creatinine phosphokinase (CPK) (IU/L) | 74 (48.5-148) | 137 (75-380) | 0.005 |
| D-dimer (ng/ml) | 708.5 (402.2-1091.7) | 1130.5 (858-3117.5) | <0.001 |
| Prothrombin time (seconds)* | 10.9 (10.4-11.95) | 11.4 (10.7-12.3) | 0.308 |
| Troponin I (ng/ml) | 5 (3.2-6.7) | 15.9 (7.4-91) | <0.001 |
| 25-hydroxyvitamin D (ng/ml) | 19.1 (14.8-19) | 19.7 (14.8-24.6) | 0.825 |
Table 5: Biochemical parameters at admission among hospitalized patients who recovered compared with those who died.
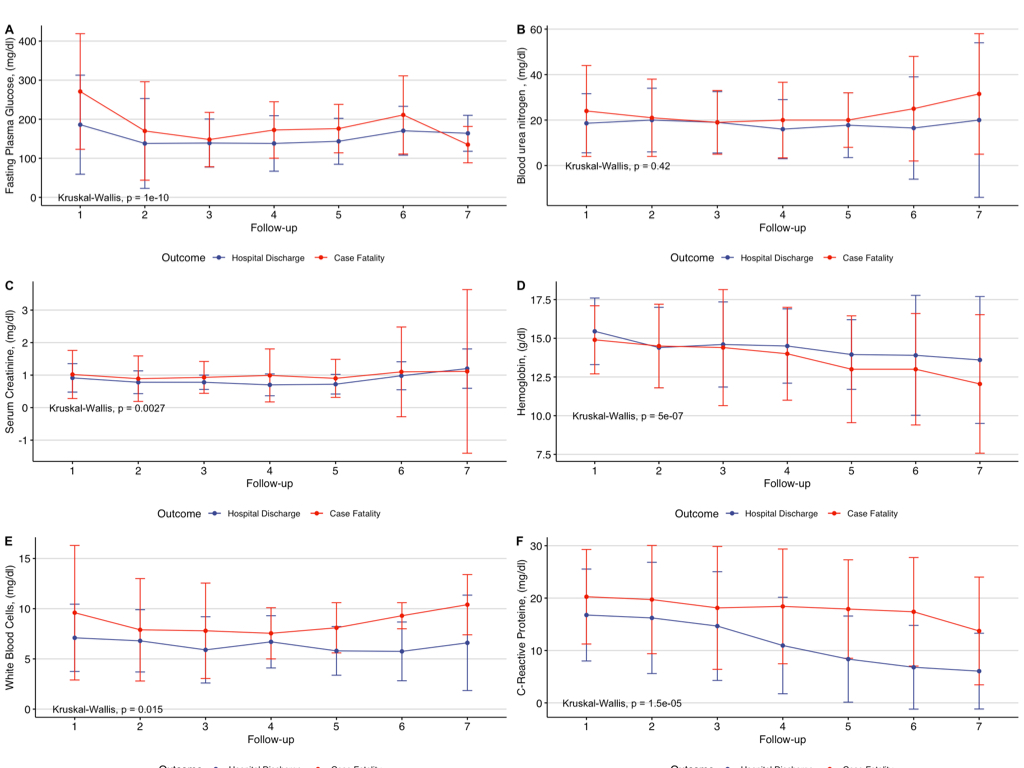
HbA1c was measured in 44 patients (33.3%); in 24 patients who recovered the HbA1c was 8.8% ±2.2 and in 20 patients who died 9.0% ±1.5 (p=0.729). Capillary glucose was different in deceased vs recovered patients. Glucose concentrations were higher during the first and second weeks in deceased patients (Figure 3 and Supplementary Table V). During hospitalization 29 episodes of hypoglycemia were reported and 11 were severe hypoglycemia episodes.
Factors associated with mortality were age ≥65 years (HR 2.88, 95%CI 1.61-5.17), respiratory rate ≥25 rpm (HR 3.86, 95%CI 1.33-11.12), heart rate ≥100 bpm (HR 1.82, 95%CI 0.96-3.42), PaFiO2 <100 (HR 3.70, 95% CI 1.06-6.65) and fasting glucose ≥150 mg/dl (HR: 2.57, 95%CI 1.05-6.25) (Figure 2D).
Reported complications during hospitalization were refractory hypoxemia in 26 cases (19.7%), acute renal failure in 19 (14.4%), dialysis requirement in 5 (3.8%), myocardial injury in 11 (8.3%), aggregate non-viral infection in 8 (6.1%), delirium in 6 (4.5%), pulmonary thromboembolism in 5 (3.8%), diabetic ketoacidosis in 2 (1.5%), multiorgan failure in 2 (1.5%), and pneumothorax in 1 (0.8%) case.
Follow-up of Survivors
Forty-nine patients (74.2%) were contacted upon discharge. From these, 73.4% continued using supplemental oxygen at home to achieve oximetry >93%. None of the discharged patients died at follow-up, 66.7% continued with asthenia/adynamia, 45.8% persisted with myalgias/ arthralgias, and 41.7% with headache and cough. Patients reported a median loss of 5 kg during their hospital stay. The patients resumed their diabetes treatment, except 8.5% of the patients who maintained adequate glycemic control without therapy. These results are shown in Supplementary Table VI.
Discussion
In this study we analyze the clinical characteristics of patients with diabetes and COVID-19 to find factors associated with the need for hospitalization, admission to an ICU, and death. Factors associated with the need for hospitalization were low oximetry and mean arterial pressure. We found that older age, tachypnea, tachycardia, lower PaFiO2 and higher glucose were associated with death. Treatment did not differ between groups, which might imply that the most important factors associated with hospitalization need and death were metabolic control and vital signs.
We observed a difference in glycemic control at admission and during the first week in hospital in survivor’s vs deceased patients. Different authors have reported an 89% survival rate in patients with glucose levels <180 mg/dl; above this threshold the survival rate falls to 11% [19]. The activation of the renin angiotensin system (RAS) in the pathogenesis of SARS-CoV-2 might predispose individuals with diabetes to have glucose elevation due to beta cell destruction.
Although patients requiring hospitalization had a higher BMI this difference was not significant. Obesity has been reported as a contributing factor to adverse outcomes related to COVID19, possibly due to a state of low-grade, chronic inflammation which worsens with SARS-CoV-2 infection [19].
We found hypertension (43.2%), dyslipidemia (27.6%) and nephropathy (14.8%) as the main comorbidities in our study population. These comorbidities were different between groups who were outpatients and those who required hospitalization.
Male sex is known to be a risk factor for a severe disease presentation and death. Approximately 60% of deaths from COVID-19 are in men (hazard ratio 1.59, 95%CI 1.53-1.65) [20]. In this study most deceased patients and those who required hospitalization were men. However, the mechanism by which SARS-CoV-2 causes more severe disease in males remains unclear. In our analysis men had lower lymphocytes, higher ferritin, CPK and D dimer and prothrombin.
Our patients lost around 5 kg during hospitalization. Studies have reported that most survivors return to their prehospitalization weight within the first year after discharge, mainly due to adipose tissue accumulation [1]. Ayres, et al. [1] reported that in the first week after admission to an ICU, patients lose around 20% of their body mass. A future analysis is needed to evaluate weight trajectory and body composition in survivors as part of their follow-up.
Reports show that 25-50% of patients with COVID-19 are asymptomatic but test positive for SARS-CoV-2 and might transmit the disease [1]. In our evaluation 4.5% of the patients who were sent home were asymptomatic. In their follow-up, they maintained good health.
Post-viral syndromes manifest as low energy feeling and dizziness which are associated with post-viral hypocortisolism [2]. When contacting discharged patients, 66.7% of our population continued with asthenia/ adynamia for one week, and myalgias/arthralgias were reported in 45.8% of patients (duration of 3.5 days). Reports from previous pandemics showed that survivors develop myopathies. Muscle weakness is attributed to fiber dysfunction due to impaired mitochondrial function and metabolic alterations necessary for muscle regeneration [1].
Vitamin D may play a role in SARS-CoV-2 virulence [2]. In this study, vitamin D levels were low both in outpatients (21.6 ng/ml) and hospitalized patients (19.05 ng/ml), which could be part of the physiopathology of COVID-19, sequestration by adipose tissue (in those with high BMI) or due to a high prevalence of vitamin D deficiency in our country. Vitamin D and 1, 25 (OH)2D stimulate the production of anti- inflammatory Th2 cytokines [2]. Therefore, vitamin D may play a role in reducing inflammation [2].
In conclusion, people with diabetes have a more severe presentation of COVID-19. The analysis of the determinants that condition the behavior of COVID-19 should continue. This will help us to improve counseling and care of patients with diabetes with COVID-19. Educational campaigns should be created to reinforce actions to maintain glycemic control goals, weight, and other comorbidities. It is important to not let symptoms progress for more than 3 days, especially in socioeconomic and culturally vulnerable areas. We continue learning about COVID-19 and its consequences, and sharing information is crucial.
Acknowledgement
To all health care providers (medical residents, assigned physicians, nursing staff, nutritionist, diabetes educators), laundry, security, administrative staff, and all those who demonstrated their value and dedication by being in front of each patient with COVID-19 to help in their treatment. To the physicians who contributed to the elaboration of the institutional database, specially to Said Urbina Teran and Iliana Mejía Herrera. To all health professionals who dedicated time and effort to mitigate the impact of the pandemic in our country.
Funding: None
Conflict of Interest: No potential conflicts of interest relevant to this article were reported.
Author Contributions
Research idea and study design SHJ, ACGU, PAV, CAAS, CLS, FRD; data acquisition: MDP, CLS, FRD; data analysis/ interpretation SHJ, ACGU, PAV; statistical analysis SHJ, ACGU, PAV; manuscript drafting SHJ, ACGU, MAGS; supervision or mentorship AGF, THG, AGH, CAAS, FJGP, DKS. Each author contributed important intellectual content during manuscript drafting or revision and accepted accountability for the overall work by ensuring that questions pertaining to the accuracy or integrity of any portion of the work are appropriately investigated and resolved.
References
-
Ruan Q, Yang K, Wang W, Jiang L, Song J (2020) Clinical predictors of mortality due to COVID-19 based on and analysis of data of 150 patients from Wuhan, China. Intensive Care Med 46(5): 846-848.
-
Wu Z, McGoogan JM (2020) Characteristics of and Important Lessons From the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72 314 Cases From the Chinese Center for Disease Control and Prevention. JAMA 323(13): 1239-1242.
-
Zhou F, Yu T, Du R, Fan G, Liu Y, et al. (2020) Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet 395(10229): 1054-1062.
-
Guan W, Ni Z, Hu Y, Liang W, Ou Ch, et al. (2020) Clinical Characteristics of Coronavirus Disease 2019 in China. N Engl J Med 382: 1708-1720.
-
Richardson S, Hirsch JS, Narasimhan M, Crawford JM, McGinn T, et al. (2020) Presenting Characteristics, Comorbidities, and Outcomes Among 5700 Patients Hospitalized With COVID-19 in the New York City Area. JAMA 323(20): 2052-2059.
-
Ortiz Brizuela E, Villanueva Reza M, Gonzalez Lara MF, Tamez Torres KM, Roman Montes CM, et al. (2020) Clinical and epidemiological characteristics of patients diagnosed with covid-19 in a tertiary care center in Mexico City: a prospective cohort study. Rev Invest Clin 72(3): 165-177.
-
Apicella M, Campopiano MC, Mantuano M, Mazoni L, Coppelli A, et al. (2020) COVID-19 in people with diabetes: understanding the reasons for worse outcomes. Lancet Diabetes Endocrinol 8(9): 782-792.
-
Ayres JS (2020) A metabolic handbook for the COVID-19 pandemic. Nature metabolism 2(7): 572-585.
-
Somasundaram NP, Ranathunga I, Ratnasamy V, Wijewickrama P, Dissanayake HA, et al. (2020) The Impact of SARS-Cov-2 Virus Infection on the Endocrine System. Journal of the Endocrine Society 4(8): bvaa082.
-
Zhu L, She ZG, Cheng X, Qin J, Zhang X, et al. (2020) Association of Blood Glucose Control and Outcomes in Patients with COVID-19 and Pre-existing Type 2 Diabetes. Cell Metab 31(6): 1068-1077.e3.
-
Wang Z, Du Z, Zhu F (2020) Glycosylated hemoglobin is associated with systemic inflammation, hypercoagulability, and prognosis of COVID-19 patients. Diabetes Res Clin Pract 164: 108214.
-
Sardu C, D’Onofrio N, Balestrieri ML, Barbieri M, Rizzo MA, et al. (2020) Outcomes in Patients With Hyperglycemia Affected by COVID-19: Can We Do More on Glycemic Control? Diabetes Care 43(7): 1408-1415.
-
Bello Chavolla OY, Bahena López JP, Antonio Villa NE, Vargas Vazquez A, Gonzalez Díaz A, et al. (2020) Predicting Mortality Due to SARS-CoV-2: A Mechanistic Score Relating Obesity and Diabetes to COVID-19 Outcomes in Mexico. The Journal of Clinical Endocrinology & Metabolism 105(8): dgaa346.
-
Zhang JJ, Dong X, Cao YY, Yuan Y, Yang Y, et al. (2020) Clinical characteristics of 140 patients infected with SARS-CoV-2 in Wuhan, China. Allergy 75(7): 1730-1741.
-
Simonnet A, Chetboun M, Poissy J, Raverdy V, Noulette J, et al. (2020) High Prevalence of Obesity in Severe Acute Respiratory Syndrome Coronavirus-2 (SARS-CoV-2) Requiring Invasive Mechanical Ventilation. Obesity (Silver Spring) 28(7): 1195-1199.
-
Cariou B, Hadjadj S, Wargny M, Pichelin M, Al-Salameh A, et al. (2020) Phenotypic characteristics and prognosis of inpatients with COVID-19 and diabetes: the CORONADO study. Diabetologia 63(8): 1500-1515.
-
Agarwal S, Schechter C, Southern W, Crandall JP, Tomer Y (2020) Preadmission Diabetes-Specific Risk Factors for Mortality in Hospitalized Patients With Diabetes and Coronavirus Disease 2019. Diabetes Care 43(10): 2339- 2344.
-
Riddle MC, Buse JB, Franks PW, Knowler WC, Ratner RE, et al. (2020) COVID-19 in People with Diabetes: Urgently Needed Lessons from Early Reports. Diabetes Care 43(7): 1378-1381.
-
Caballero AE, Ceriello A, Misra A, Aschner P, McDonnell ME, et al. (2020) COVID-19 in people living with diabetes: An international consensus. Journal of Diabetes and Its Complications 34(9): 107671.
-
Takahashi T, Ellingson MK, Wong P, Israelow B, Lucas C, et al. (2020) Sex differences in immune responses that underlie COVID-19 disease outcomes. Nature 588: 315- 320.
- Investigation of Polymorphisms in PPAR-Ɣ and TRHR Genes and their Impact on Turkish Diabetic and Obese Individuals
- The Impact of Aircraft Noise Exposure on the Efficacy of Empagliflozin Therapy in an Animal Model of Obesity
- Rooibos Mitigates Metabolic and Inflammatory Dysfunctions in Mice Fed a High-Carbohydrate Diet
- Synergistic Effect of Combined Leaf Extract of Vernonia amygdalina, Ocimum gratissimum, and Zingiber officinale Tuber on Phytochemical Profile, Antioxidant Activity, Serum Insulin, and Biochemical Parameters in Streptozotocin-Induced Diabetic Rats
- Investigation of Cardiovascular Responses to Aerobic Exercise in Obese University Students
- A Look at the Phase Angle Obtained by Electrical Bioimpedance