How safe is Contraception use among Obese Diabetic Women?
Incidence of diabetes mellitus is increasing is worldwide. The incidence of obesity is also increasing among the diabetic people. Sexually active obese women are commonly encountered nowadays due to increase in the global burden of obesity and diabetes mellitus Obesity and diabetes mellitus is associated with many health risks and a pregnant obese diabetic woman has health risks not only for herself but also to the foetus she carries. Thus, an effective birth control method is important to reduce pregnancy related complications. Though most of us are aware of management of diabetes and obesity, we may not be aware of the contraceptive usage among premenopausal women and HRT [hormone replacement therapy] use among perimenopausal women. A study was conducted to find the incidence of obese diabetics among the women attending a religious function. Later the study was extended to find the contraceptive use among the obese diabetic women and HRT usage among obese perimenopausal diabetic women. It has been found that 16/84 are prediabetic 25/84 are diabetic and 35/84 are overweight and 22/84 are obese. Follow up study was done to find out what contraceptive method was used by them and their knowledge about the contraceptive use. 77% (n=364) of the sexually active obese women are using contraception, with most of them using hormonal contraception. We are aware that some of the oral contraceptives will aggravate diabetes and obesity. Introduction: There is global increase in diabetes mellitus together with increasing incidence of obesity among women. This increase in obese diabetic women includes increasing numbers of women of a reproductive age whose reproductive health and contraception need careful consideration. We have conducted a study among obese diabetic women and their contraceptive usage. This study explored the level of knowledge, attitude, and practice of contraception usage of the sexually active obese women. Among the respondents (25.6%) were not aware of the best contraceptive for sexually active obese women. It is noted that 32.1% of obese women with underlying medical illness were still on hormonal contraception. The awareness of health risk associated with hormonal contraceptive usage of the amongst the obese diabetic women is less. This study has revealed that there is a lack of education and counselling with regards to safe and appropriate use of contraceptive to the women who need it for family planning. Objective: This study aims to look at the knowledge, attitude and practice (KAP) in the choice of contraceptives among obese and sexually active women. Methods: This study was conducted at Ministry of Health, health facilities and Private General Practitioners’ Clinics in Peninsular Malaysia. A self-designed questionnaire was used to assess KAP of the participants. A total of 473 respondents participated in the survey. Results: 77% (n=364) of the sexually active obese women are using contraceptives. Majority used hormonal contraceptives (n=204, 56%) and barrier method was the preferred method (39%, n=142) among the others. Women with Hypertension and Type II Diabetes Mellitus have the highest rate of using hormonal contraception (51.6%, n=32, 52.6%, n=30) respectively. Both groups have low awareness on the health risk associated with hormonal contraception which was 69% and 83% respectively. Most of the respondents were satisfied with the method of contraception they use, and majority mentioned ‘Easy to take’ as the reason for using it. 32%(n=152) of the respondents have underlying medical illnesses. 24.5% thought that hormonal contraception is the best. 23.5% choose IUCD as the method of choice. Conclusion: In the first part of the study the incidence of diabetes mellitus and obesity among the women was done. In the second part the study explored the level of knowledge, attitude, and practice, of the sexually active obese women based on their sociodemographic data in the choice of the appropriate contraceptive considering their existing medical conditions and sources of procurement. Majority of obese women used non hormonal contraception and almost half of the rest chose hormonal contraception. A quarter of the respondents claimed that hormonal contraception was the best choice. Many obese women with underlying medical illnesses were on hormonal contraception. It is noted that 32.1% of obese women with underlying medical illness were still on hormonal contraception. The awareness amongst the diabetic and hypertensive respondents on health risk associated with hormonal contraceptive used was noted to be poor, being 38.7% and 42.9% respectively. The use of IUCD as the preferred and appropriate choice for those with medical conditions is very discouraging (less than 3%).
Introduction
Age and BMI
Among them 26% [22/84] were normal BMI, 41% [35/84] were overweight and 32% [27/84] were obese.
Among them 41.5 % overweight pre and perimenopausal women and 32 % were obese pre and perimenopausal women. About 36 % of obese women were in the age group [less than 60 years age] who may require contraceptives or HRT (Table 1).
| Age | <40 | 41-60 | >60 | Total |
|---|---|---|---|---|
| <25 | 14 | 1 | 7 | 22 |
| 26-29 | 3 | 13 | 19 | 35 |
| >30 | 3 | 11 | 13 | 27 |
| Total | 20 | 25 | 39 | 84 |
Table 1: Age and BMI.
Age and Blood sugar
53.4% were non-diabetic 16.6% were pre diabetic and
30 % were diabetic. About 46.5% of diabetic women require contraceptives or HRT (Table 2).
| Age <40 | 41-60 | >60 | TOTAL | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Blood sugar | 5.5-8 | 8-10 | >10 | 5.5-8 | 8-10 | >10 | 5.5-8 | 8-10 | >10 | |
| Total | 16 | 2 | 2 | 16 | 6 | 6 | 13 | 6 | 17 | 84 |
Table 2: Age and Blood sugar.
Age, BMI, Blood Sugar
23[27.4%] were pre diabetic overweight women and 19[22.6%] were prediabetic obese women. 12 [14.2%] were diabetic overweight women and 8[10%] were diabetic obese women. 36[43%] were below 60 years and pre or diabetic women who may require contraceptive or HRT management (Table 3).
| <40 | 41-60 | >60 | Total | |
|---|---|---|---|---|
| Blood sugar < 5.5 | ||||
| <25 | 4 | 0 | 4 | |
| 26-29 | 0 | 2 | 3 | 5 |
| >30 | 0 | 1 | 2 | 3 |
| 4 | 3 | 5 | 12 | |
| Blood sugar 5.5 - 8 | ||||
| <25 | 11 | 1 | 2 | 14 |
| 26-29 | 2 | 10 | 4 | 16 |
| >30 | 1 | 5 | 7 | 13 |
| 16 | 16 | 13 | 45 | |
| Blood sugar 8.1-10 | ||||
| <25 | 1 | 0 | 0 | 1 |
| 26-29 | 0 | 3 | 4 | 7 |
| >30 | 1 | 3 | 2 | 6 |
| 2 | 6 | 6 | 14 | |
| Blood sugar >10 | ||||
| <25 | 0 | 0 | 5 | 5 |
| 26-29 | 1 | 3 | 8 | 12 |
| >30 | 1 | 3 | 4 | 8 |
| 2 | 6 | 17 | 25 | |
| Total | 24 | 31 | 31 | 84 |
Table 3: Age, BMI, Blood sugar.
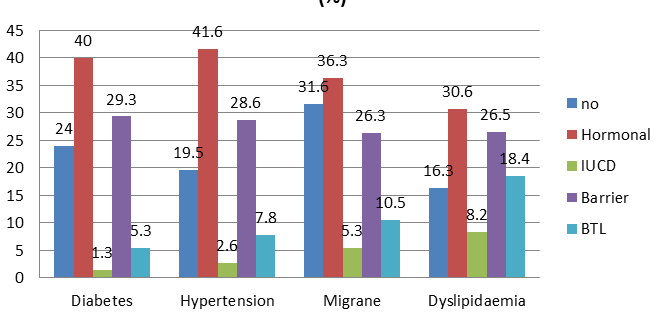
Out of total 152 obese women using contraceptives 49 had diabetes and 72 had hypertension (Figure 1).
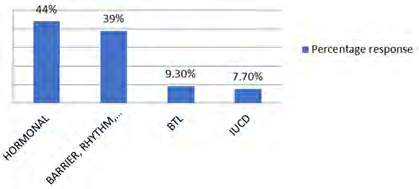
44 % of the responders used hormonal contraception and 39 % used non hormonal method like barrier or rhythm method (Figure 2).
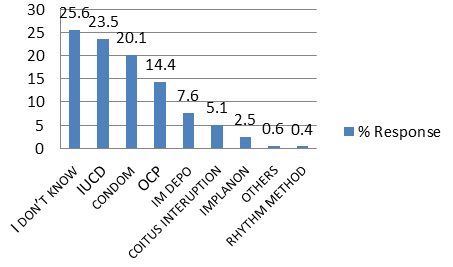
41% has no knowledge about the risks of using contraceptives. 32.8 % felt it can produce obesity. 7% thought it can produce cancer (Figures 3 & 4).
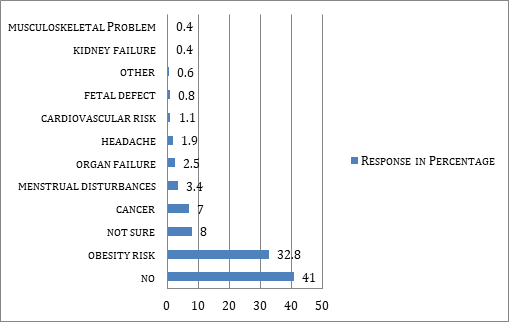
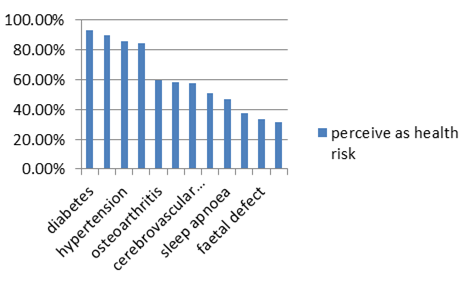
92% felt obesity can produce diabetes, 90% coronary heart disease, 85% hypertension, 60% arthritis (Figure 5).
Discussion
This study revealed lack of awareness was noted, of the association between obesity and health risks as related to hormonal contraception. There was also a lack of knowledge amongst the obese, in selecting suitable contraception. Most of the respondents obtained their contraceptives from government or private clinics while a small number obtained it from the pharmacies, shops, This shows lack of proper education on the contraceptive usage.There is increasing incidence of obesity among women [1]. In imperative that an effective birth control method must be followed to reduce pregnancy related complications [2]. Diabetes mellitus (DM) is the most common of metabolic disorders and it has become important global public health concern. Three hundred and eighty-three million adults are currently diagnosed with DM and another 175 million are estimated to be living with the condition but are yet undiagnosed [3]. It is expected to increase in 2035 by 55% with 592 million people will be affected worldwide [3].
Obesity and Contraception
Obesity among diabetes has reached epidemic proportions in all most all countries Effectiveness of hormonal contraceptives may affected by their metabolic changes in obese women or to increased BMI [Body mass index] or body fat. Most of the hormonal contraceptives include oral contraceptives (OCs), injectables hormones, hormone implants, hormonal intrauterine contraception (IUC), the transdermal patch, and the vaginal ring. Due to increased prevalence of overweight and obesity women, the public health awareness program must have effect on contraceptive efficacy use among obese diabetic women must be substantial. Complications can arise due to usage of full range of contraceptive methods including hormonal contraception, but advantages of their use must outweigh any risk. Women with diabetic complications may need specialist advice as it is important to assess the risk–benefit advantage, especially in respect of hormonal contraception. Hormonal contraception among obese diabetic is the most important condition complicating pregnancy and affects up to 10% of women of a reproductive age in developed countries [4]. Usage of contraceptive is almost same among women of all BMI, but traditionally contraceptive development studies excluded women over 130% of ideal body weight. This has caused very little information for obese diabetics and health care providers in understanding of contraceptive efficacy for obese and overweight women. Due to a range of drug metabolism alterations in obese women there is a possibility for changes in hormonal contraception metabolism and its effectiveness in obese women. But available research studies did not reveal any difference in oral contraceptive pill effectiveness in obese women compared with non-obese women. There is very little data for obese women using progestin type of contraceptive usage. While using non- oral contraceptives the effectiveness was not compromised in obesity women. There are some exceptions to it like the combined hormonal patch and oral levonorgestrel emergency contraception may be less effective in obese women. But Intrauterine contraception (IUC) which works by a local mechanism of action, there is no evidence of reduced effectiveness of levonorgestrel intrauterine systems (LNG- IUS) or copper intrauterine devices (Cu-IUD) in women with raised BMI [5]. There is a technical difficulty in the insertion and removal of intra uterine devices in obese women but raised BMI did not show any significant factor in insertion failures [6].
Progestogen-only Implant
The etonogestrel (ENG) implant is effective method of contraception, but limited studies have been done with the specific aim of assessing the impact of weight or BMI on etonogestrel effectiveness as a contraceptive drug. The manufacturer suggested early replacement of the etonogestrel implant can be considered in obese women as blood levels of etonogestrel are inversely related to body weight and decrease with time after insertion [7].
Progestogen-only Injectables
Progestogen-only injectables (i.e., depot medroxyprogesterone acetate [DMPA]) are an effective method of contraception for all types of women irrespective of their body weight [7]. Raised BMI does not restrict the use of DMPA (UK medical eligibility criteria for contraceptive use. UKMEC 1). But raised BMI is one of multiple risk factors causing cardiovascular disease. UKMEC 3 [8]. More research is required as only a small body of research has linked DMPA to an increased risk of venous thromboembolism (VTE) as it may be a causal relationship which cannot be established or refuted. All physicians must consider this added risk in obese women who are already at increased risk of VTE due to high BMI. Obesity alone does not restrict the use of DMPA; but obesity is one of multiple risk factors for cardiovascular disease, DMPA becomes UKMEC 3. We must be careful of the needle used to administer DMPA and it must be long enough, so that the injection will not miss the muscle. Sufficiently longer -length needle must be used for deltoid administration, or subcutaneous DMPA injection for obese women.
Progestogen-only Pill
At present there is very limited evidence to the effectiveness of the progestogen-only pill (POP) in obese women with raised BMI. The data are available suggests that the POP is effective in obese women with raised BMI, hence double dose of POP is not recommended for contraception.
Combined Hormonal Contraception [CHC]
Combined hormonal contraception (CHC) is usually contraindicated (UKMEC 3) for use by obese women with BMI ≥35 kg/m2 as it increases thrombotic risk. Available evidence suggests that the combined patch is less effective in obese women weighing more than 90 kg. It is recommended that women who weigh more than 90 kg to consider additional precautions or use alternative method of contraception.
- The risk of thrombosis increases in obese women with increased BMI.
- Current CHC use is associated with increased risk of venous thrombo embolism which may produce myocardial infarction or ischaemic stroke
- The risks of CHC is more than the benefits in obese women with BMI ≥35 kg/m2.
Barrier and Fertility Awareness Methods
No studies have looked specifically at barrier methods or fertility awareness methods (FAM) in women with raised weight or BMI, but there are no theoretical reasons why these methods would be less effective or less safe. However, if women are experiencing irregular menstrual cycles, they should not rely on FAM; healthcare professionals should discuss how irregular bleeding patterns affect fertility awareness. For women who experience a large change in weight, it is advisable to check that their diaphragm still fits.
Emergency Contraception
The Cu-IUD is the most effective form of emergency contraception (EC) for all women and its effectiveness is not affected by weight or BMI. Some reports suggest that oral levonorgestrel EC (LNG-EC) is less effective in overweight women weighing more than 70 kg or with BMI >26 kg/m2 and oral ulipristal acetate EC (UPA-EC) is also less effective in obese women weighing >85 kg or with BMI >30 kg/m2 [9]. The guideline advised by Faculty of Sexual & Reproductive Healthcare. Emergency contraception. FSRH, 2017 is that when a Cu-IUD is not suitable or acceptable, alternatively UPA-EC must be considered, and if UPA-EC is also not suitable then, obese women can be offered a double dose of LNG-EC when their BMI is more 26 kg/m2 or their weight is more 70 kg [10]. At present we do not know how effective the double dose of LNG-EC is or its effectiveness when compared to that of UPA-EC. A double dose of UPA-EC is not recommended for any women irrespective of their body weight or BMI [10]. For those women with prior gestational diabetes mellitus (GDM) effective contraception is essential in at the same time contraception should not increase their risk of developing type 2 diabetes [11]. We are aware that Progestin-only OCs were associated with an increased risk of diabetes in breast-feeding women with recent onset GDM and should be prescribed with extra caution when prescribed for these women. Long-term use of low-dose combination OCs usually will not increase the risk of type 2 diabetes when compared with use of nonhormonal contraception. Combination OCs will not increase the risk of diabetes in non–breast-feeding women with recent GDM. Breast-feeding mothers who elected to use OCs were uniformly prescribed the progestin-only OC (0.35 mg of norethindrone) till they stop breast-feeding, after which they were switched to one of the low-dose combination OCs. When progestin-only OCs was prescribed during breast-feeding, they should be carefully monitored of blood glucose concentrations in these high-risk women. Combination OCs containing similar amounts of norethindrone or another progestational agent, levonorgestrel does not increase the risk of diabetes but when used alone the norethindrone is associated with increased. When low-dose progestin and estrogen combination OCs is used does not increase the risk of developing diabetes in the high-risk women. Important observation is that the use of a progestin-only OC while breast-feeding was associated with a nearly 3-fold increase in the incidence of diabetes when compared with the other groups. The longer uninterrupted OC use increase the risk more. In breast feeding women with high risk of developing diabetes the low-dose progestin and estrogen combination OCs appears to be safe, while the progestin-only OC appears to increase the risk of developing diabetes. It has been found that the effects of progestins and oestrogens on carbohydrate metabolism indicate that the progestin component induce insulin resistance and it is in a dose and potency dependent [12, 13, 14].
Oestrogens has very little effect or no effect on insulin sensitivity or glucose tolerance [15]. Oestrogens may actually enhance insulin action in vitro [16, 17]. Some reports suggest that Oestrogens have beneficial effects on pancreatic β-cell function in animal models of diabetes [18]. These reports suggest that while breast feeding the oestrogen levels are low and the pregestational agents may exert a more pronounced effect on induction of insulin resistance and deterioration in glucose tolerance.
Conclusion
The study has revealed that there is a lack of education and counselling with regards to safe and appropriate use of contraceptive to the women who need it for family planning. Every mother who turns up to get contraceptives should be assessed for morbid states like diabetes, obesity and should be counselled on the early recognition of side effects and complications arising from use of hormonal contraceptives. Where appropriate the non-hormonal methods like IUCD or bilateral tubal ligation should be advised. Creating awareness through distribution of pamphlets, posters, health campaigns would help. Talks in secondary and tertiary level institutions can raise the awareness among the adolescent and pre-marital group of women. Most of the respondents obtained their contraceptives from government and private clinics while a few obtained them from pharmacies and other sources. Contraceptives should only be made available at facilities managed by qualified health personnel.
Acknowledgement
Authors thank the following for the collection and compilation of the data. Dr. Sawrirajan Rajagopal, Dr. Chan Mei Wei, Dr. Norahayati Sharman, Dr. Joginder Singh Rakra , Prof Nik Sherina. Part of this work was done by Dr. Sawrirajan Rajagopal for the fulfilment of the criteria to complete the advanced training program in family medicine conducted by the academy of family physicians Malaysia.by qualified health personnel.
References
-
James WPT, Chuming C, Inoue S (2002) Appropriate Asian body mass indices? Obesity review 3(3): 139.
-
Society of Family Planning, Susan Higginbotham (2009) Contraceptive considerations in obese women: release date 1 September 2009, SFP Guideline 20091. Contraception 80(6): 583-590.
-
IDF (2013) IDF Diabetes Atlas, 6th (Edn.), International Diabetes Federation.
-
Dunlop AL, Jack BW, Bottalico JN, Lu MC, James A, et al. (2008) The clinical content of preconception care: women with chronic medical conditions. Am J Obstet Gynaecol 199(6 S2): S310-S327.
-
Katharine B Simmons, Alison B Edelman (2016) Hormonal contraception and obesity. Fertil Steril 106(6): 1282-1288.
-
FSRH (2019) Overweight, obesity and contraception. Faculty of Sexual & Reproductive Healthcare, Royal College of Obstetricians & Gynaecologists.
-
Merck Sharp, Dohme Limited (2019) Nexplanon® 68 mg implant for subdermal use-summary of product characteristics. Organon Pharma (UK) Limited.
-
(2016) UK medical eligibility criteria for contraceptive use. Faculty of Sexual & Reproductive Healthcare.
-
(2017) The Scottish Health Survey 2017-volume one: main report. The Scottish Government, Edinburgh.
-
FSRH (2017) Emergency contraception. Faculty of Sexual & Reproductive Healthcare, Royal College of Obstetricians & Gynaecologists.
-
Kjos SL, Peters RK, Xiang A, Thomas D, Schaeer U, et al. (1998) Contraception and the Risk of Type 2 Diabetes Mellitus in Latina Women With Prior Gestational Diabetes Mellitus. JAMA 280(6): 533-538.
-
Kalkhoff RK (1982) Metabolic effects of progesterone. Am J Obstet Gynecol 142(6 Pt 2): 735-738.
-
Godsland IF, Crook D, Simpson R (1990) The effects of different formulations of oral contraceptive agents on lipid and carbohydrate metabolism. N Engl J Med 323(20): 1375-1381.
-
Perlman JA, Russell-Briefel R, Ezzati T, Lieberknecht G (1985) Oral glucose tolerance and the potency of contraceptive progestins. J Chronic Dis 38(10): 857-864.
-
Spellacy WN, Buhi WC, Birk SA (1972) The effect of estrogens on carbohydrate metabolism: glucose insulin and growth hormone studies one hundred seventy- one women ingesting Premarin, mestranol and ethinyl estradiol for six months. Am J Obstet Gynecol 114: 378-
-
Ryan EA, Enns L (1988) Role of gestational hormones in the induction of insulin resistance. J Clin Endocrinol Metab 67(2): 341-347.
-
Wilcox JG, Hwang J, Hodis HN, Sevanian A, Stanczyk FZ (1997) Cardioprotective effects of individual conjugated equine estrogens through their possible modulation of insulin resistance and oxidation of low-density lipoprotein. Fertil Steril 67(1): 57-62.
-
Houssay BA, Foglia VG, Rodriguez RR (1954) Production and prevention of some types of experimental diabetes by oestrogens and corticosteroids. Acta Endocrinol 17(1-4): 146-164.
- Investigation of Polymorphisms in PPAR-Ɣ and TRHR Genes and their Impact on Turkish Diabetic and Obese Individuals
- The Impact of Aircraft Noise Exposure on the Efficacy of Empagliflozin Therapy in an Animal Model of Obesity
- Rooibos Mitigates Metabolic and Inflammatory Dysfunctions in Mice Fed a High-Carbohydrate Diet
- Synergistic Effect of Combined Leaf Extract of Vernonia amygdalina, Ocimum gratissimum, and Zingiber officinale Tuber on Phytochemical Profile, Antioxidant Activity, Serum Insulin, and Biochemical Parameters in Streptozotocin-Induced Diabetic Rats
- Investigation of Cardiovascular Responses to Aerobic Exercise in Obese University Students
- A Look at the Phase Angle Obtained by Electrical Bioimpedance