Awareness of Diabetes Complication in Subjects with Type 2 Diabetes
Patients with diabetes are well-educated about the self-management of glycemic control; conversely, the education on the screening of complications are less structured and personalized. We designed our study to assess the awareness of complications in a sample of people with type 2 diabetes (T2D). This is an observational cross-sectional study. A questionnaire aimed to evaluate the knowledge of micro- and macro-vascular diabetic complications and of the tests used to detect them was provided to consecutive people with T2D. Three-hundred eleven participants with T2D were enrolled and competed the questionnaire. The majority of them were aware of retinopathy (98%), kidney disease (90%), cardiovascular diseases (57%), and leg sensitive abnormalities (83%), while few were aware of sexual (38%), bladder (45%), gastrointestinal (27%) and cardiovascular autonomic disorders (0.6%). Among those who were aware of sexual disorders, 33% defined the complication specific of male sex and 5% of both sexes. About one-third were aware of albuminuria, and 37% indicated electromyography as the standard test for peripheral neuropathy. An adequate level of awareness for most complications was observed. However, some complications linked to autonomic neuropathy and standard tests to detect diabetic nephropathy and peripheral neuropathy were poorly known. Furthermore, bladder, gastrointestinal disorders, and cardiac autonomic neuropathy were also less aware or unaware. A comprehensive education might be helpful to prevent the lesser-known complications and avoid inappropriate and expensive diagnostic tests.
Introduction
Diabetes is the most widespread public health challenge draining many humans and economic resources in several countries. Leading specialists involved in the delivery of diabetes care and education are the doctor and the nurse. Patient-tailored educational activities, managed by specialized nurses, aim to keep therapeutic adherence, stimulate glucose monitoring, propose nutritional programs and physical activity, and prevent acute hypo- and hyper- glycemia are essential to maintain and achieve adequate glycemic control. International guidelines recommend self- management education and support (DSMES) as the key element enabling people with diabetes to decide on daily diabetes management [1]. Conversely, the education on the screening of complications seems to be less structured and personalized. Some complications, as diabetic retinopathy and diabetic foot, are well known in the patient community and more discussed during the visit than other complications.
The prevention of chronic micro-and macro-vascular complications is fundamental to reduce the high rate of diabetes mortality and morbidity [2]. The main causes of death in people with diabetes are cardiovascular diseases and end-stage renal disease, fostered by poor glycemic control, disease duration, comorbidities, delay in the intensification of treatment, low patients’ education, and lack of regular screening [3, 4].
Unfortunately, most of the complications become clinically manifest in the late stage; therefore, a regular and possibly annual screening is essential for early detection. Guidelines suggest the screening to promptly intensify treatment and avoid worsening of the clinical conditions [5].
Reasons for the lack of adequate screening are manifold. Among these, to mention only the most frequent ones, patients’ knowledge, accessibility to facilities in the center for the cure of diabetes, availability of a medical team. According to the recent annual report from the Italian Association of Diabetes from a cohort of 473.740 people with type 2 diabetes, 67% measured microalbuminuria, 21% underwent foot inspection, and 37% performed the fundoscopy. There are no data about the screening for neuropathy or cardiovascular diseases, while blood pressure and lipids seem to be regularly measured [6]. We have designed the present study to assess, by a questionnaire, the knowledge on complications in a sample of people with type 2 diabetes attending the center for the care of diabetes and the test used to detect some complications.
Methodology
The survey research includes people with type 2 diabetes attending our diabetes health care center for three months. An expert specialist in diabetes prepared the questionnaire in line with those available in the literature for diabetic retinopathy [7]. Specialized nurses administered the questionnaire to consecutive patients who gave their informed consent. The questions included information about the knowledge of each complication and the suggested tests used to detect its presence (supplementary data). If requested, the nurse better described specific disorders and tests. Age, sex, disease duration, and the ongoing insulin or non-insulin treatment were collected.
Data Collection
All results have been reported as a percentage. Patients were divided into three groups according to the age: ≤ 50, 50 ≤ 70, and > 70. A score of 1 was attributed to each correct response, and the mean value was calculated. According to the score mean value, patients were divided into tertiles and classified as Aware, Less Unaware, and Unaware.
Statistical Analyses
The Analysis of Variance was used to evaluate the differences of continuous variables among groups, while the chi-square test was applied to compare percentages. The sample size was determined according to the following survey sample size formula [8]:
n = (p (100 – p) z2)/ E2
Where p is the percentage of a sample having the characteristic of interest (awareness of diabetes complications), z is the value corresponding to the level of confidence required, and E is the margin of error. By setting a p of 75%, with a z of 1.96 (level of confidence of 0.05) and an E of 5%, a sample size of 288 was determined.
The local Ethical Committee was informed about the investigation. According to national guidelines, GU n. 76 del 31-3-2008, approval for this research is not requested. Non- sensitive data were collected.
Results
Three-hundred eleven subjects with type 2 diabetes completed the questionnaire (all the subjects to whom the questionnaire was administered). Mean±standard deviation of age, disease duration, and age at the onset of diabetes were respectively 61±11 years, 12±8 years, and 49±11 years. The prevalence of males was 66%. Among participants, 190 (61%) were taking non-insulin hypoglycemic drugs, and 121 (39%) were injecting at least one insulin daily.
| Yes (%) | No (%) | Don’t know (%) | |
|---|---|---|---|
| 1. Does diabetes affect organs? | 98 | 0.6 | 1.3 |
| 2. Does diabetes affect the heart and vessels? | 57 | 29 | 14 |
| 3. Does diabetes affect the eye? | 98 | 0 | 1.6 |
| 4. Does diabetes affect the kidney? | 90 | 0.3 | 9.3 |
| 5. Does diabetes affect lower leg sensitivity? | 83 | 2.3 | 14.8 |
| 6. Does diabetes cause sexual disorders? | 38 | 24 | 38 |
| 7. Does diabetes cause foot ulcers? | 85 | 0.6 | 14 |
| 8. Does diabetes cause bladder disorders? | 45 | 3.5 | 52 |
| 9. Does diabetes cause gastrointestinal disorders? | 27 | 18 | 55 |
| 10. Does diabetes affect blood pressure and heart rate? | 0.6 | 40 | 59 |
Table 1: Questionnaire and percentage of response Yes, No, Don’t know.
Table 1 shows the percentage of Yes, No, and Don’t know for each question submitted to the patients. Most patients agreed diabetes can affect the function of organs. Diabetic retinopathy, nephropathy, and diabetic foot were the known complications among interviewed patients.
Conversely, diabetic autonomic neuropathy (sexual, bladder, gastrointestinal disorders, blood pressure abnormalities, and heart rate) was less known. Question no. 6 (sexual disorders) provided different answers for Yes: Yes, Only in males, and Yes, in Both Sexes. In the table, we have displayed the percentage of Yes, however the respective answers for Yes in male and Yes in both sexes were 33% and
5%. All interviewed participants requested more details on question 10 (Does diabetes affect blood pressure and heart rate?). The nurses reformulated the question asking if they knew that diabetes might affect blood pressure regulation while changing the position or increase heart rate at rest.
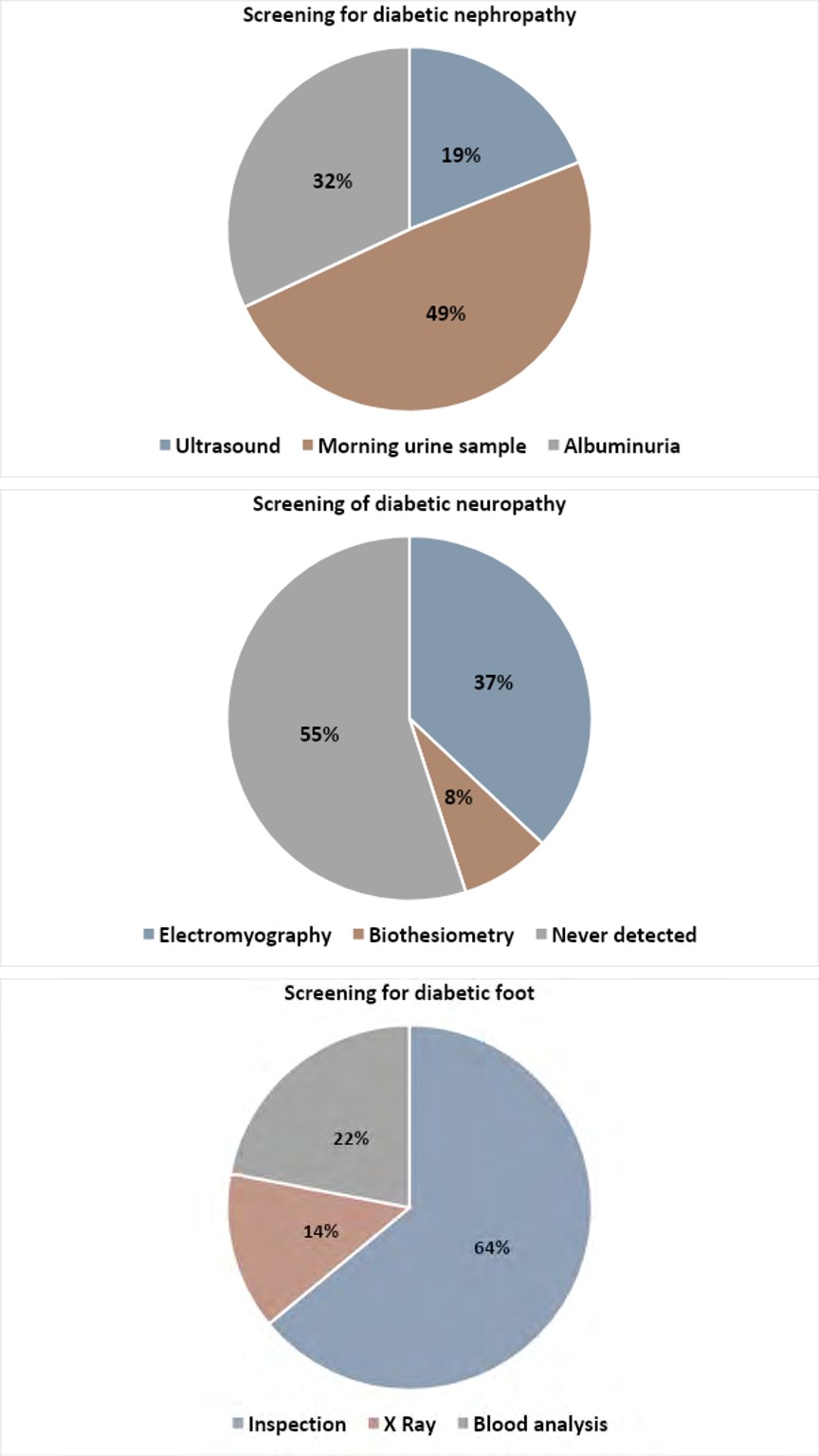
We have also investigated the timing for the screening of diabetic retinopathy, and the answers were the following: once a year 83%, 13% if symptoms occur, 4% every 5 years. In Figure 1 we have illustrated the answers of participants on the suggested tests for the diagnosis of nephropathy, neuropathy, and diabetic foot.
| Aware | Less aware | Unaware | p | |
|---|---|---|---|---|
| N (%) | 100 (32) | 124 (40) | 87 (28) | --- |
| Age (years) | 64±8 | 61±10 | 57±13 | 0.0001a |
| ≤ 50 years (%) | 8 | 40 | 52 | 0.0001b |
| ≤ 70 years (%) | 35 | 41 | 24 | |
| > 70 years (%) | 42 | 36 | 22 | |
| Disease duration (years) | 15±10 | 11±8 | 9±6 | 0.0001a |
| Male (%) | 46 | 40 | 14 | 0.048 |
| Female (%) | 37 | 34 | 28 | |
| Non-insulin drugs (%) | 57 | 56 | 74 | 0.02 |
| Insulin drugs (%) | 43 | 44 | 26 |
Table 2: Patients divided into three tertiles according to their awareness levels. aOne way ANOVA; bchi square test The mean scor
Table 2: Patients divided into three tertiles according to their awareness levels. aOne way ANOVA; bchi square test The mean score for each group was: Aware 7.7±0.7, Less Aware 5.6±0.5, and Unaware 3.2±0.8. Aware participants were significantly older, with longer disease duration, higher prevalence of males, and injecting at least one insulin per day.
Discussion
The present study has demonstrated a good level of knowledge of diabetes complications among patients with type 2 diabetes and a low level of knowledge on the specific tests detecting complications. More than half of interviewed patients had an overall acceptable level of knowledge, and one-third seemed very well aware. Specifically, we found a high prevalence of awareness for diabetic retinopathy, nephropathy, diabetic foot, and loss of peripheral sensitivity. Conversely, less than half of the interviewed patients associated diabetes with sexual or bladder disorders, and less than one-third with gastrointestinal disorders. Sexual disorders have been considered by most of the interviewed a male-specific complication. Almost no one believed that diabetes might affect blood pressure and heart rate, although the question was further detailed during the interview.
Older patients and those with a longer disease duration were those more aware, and this finding was expected since the longer the illness, the greater the level of knowledge. The gender difference we found in our study has been described in other studies [9]. Males have a higher level of knowledge than females. We hypothesize that among women, there is a higher adhesion to the screening for breast and uterus cancer than the screening for diabetes complications.
A further significant difference among aware, less aware, and unaware patients, was detected between those injecting or not injecting insulin. The higher level of knowledge in insulin-treated patients could be attributable to the more frequent access to the ambulatory and, therefore, to the increased likelihood of discussing complications or the higher prevalence of complications in these patients [10].
We have then compared our results with those available in the literature. A recent report has described a very low prevalence (20%) of adequate knowledge on complications in a sample of Ethiopian patients with an average age of about 45 yrs. The factors related to a better, despite insufficient, level of understanding were younger age, male sex, higher income, residence in an urban area, and disease duration [11]. The most investigated and known complication in different countries is diabetic retinopathy, with a prevalence of its knowledge of about 60-70% [12, 13, 14]. It is of particular interest that the interviewed patients know that diabetes might cause the reduction or loss of sight, but a very low number of patients know the term retina and use the correct terminology [14]. A recent paper from the central area of Saudi Arabia has investigated the knowledge, attitude, and practice of about 300 patients with type 1 and type 2 diabetes. They have demonstrated that participants with a good level of attitude and knowledge on basic aspects of diabetes (self- monitoring of blood glucose, diet, physical activity) also have a good knowledge of retinopathy, nephropathy, foot ulcer, and cardiovascular diseases [15]. This study suggests that the multidisciplinary approach should be pursued to obtain good metabolic control and a low rate of complications.
The study shows some limits: patients have been enrolled only in one center where a specialized team is involved in the care of the disease. The questionnaire did not include questions about metabolic control, concomitant disease, and complications. Some questions were detailed by the specialized nurses if necessary, and this might have influenced the response. In Italy, diabetes care is provided by specialists in the diabetic clinic, and doctors, specialized nurses, and dietitians cooperate in providing the best care according to the national guidelines. This kind of assistance might have influenced the results of the survey.
Conclusion
In conclusion, we can state that there is a good level of information and education for most complications in our sample of patients with type 2 diabetes. There is a grey zone for some complications as bladder and gastrointestinal disorders and a black box for cardiovascular autonomic neuropathy. The cooperation between patients, doctors, and specialized nurses is fundamental to managing diabetes and preventing long-term complications. Likely, better education and modern technologies can reduce the gap between knowledge and the number of performed screening.
References
-
Davies MJ, D’Alessio DA, Fradkin J, Kernan WA, Mathieu C, et al. (2018) Management of Hyperglycemia in Type 2 Diabetes. A Consensus Report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care 41(12): 2669- 2701.
-
Cusick M, Meleth AD, Agrón A, Fisher MR, Reed GF, et al. (2005) Associations of mortality and diabetes complications in patients with type 1 and type 2 diabetes: early treatment diabetic retinopathy study report no. 27. Diabetes Care 28(3): 617-625.
-
Li S, Wang J, Zhang B, Li X, Li Y (2019) Diabetes Mellitus and Cause-Specific Mortality: A Population-Based Study. Diabetes Metab J 43(3): 319-341.
-
Tracey ML, McHugh SM, Fitzgerald AP, Buckley CM, Canavan RJ, et al. (2016) Risk Factors for Macro- and Microvascular Complications among Older Adults with Diagnosed Type 2 Diabetes: Findings from The Irish Longitudinal Study on Ageing. J Diabetes Res 2016: 5975903.
-
American Diabetes Association (2021) Microvascular Complications and Foot Care: Standards of Medical Care in Diabetes. Diabetes Care 44: S151-S167.
-
AMD. 2020. Annals 2020.
-
Almalki NR, Almalki TM, Alswat K (2018) Diabetics Retinopathy Knowledge and Awareness Assessment among the Type 2 Diabetics. Open Access Maced J Med Sci 6(3): 574-577.
-
Taherdoost H (2017) Determining Sample Size; How to Calculate Survey Sample Size. International Journal of Economics and Management System.
-
Peters SAE, Woodwar M (2018) Sex Differences in the Burden and Complications of Diabetes. Curr Diab Rep 18(6): 33.
-
Willis WD, Diago-Cabezudo JI, Madec-Hily A, Asalm A (2013) Medical resource use, disturbance of daily life and burden of hypoglycemia in insulin-treated patients with diabetes: results from a European online survey. Pharmacoecon Outcomes Res 13(1): 123-130.
-
Gizaw AB, Belachew YB, Kebede DB (2019) Knowledge about Diabetic Complications among Patients on Diabetic Follow up Clinic at Jimma University Medical Centre. J Diabetes Metab Disord 6: 029.
-
Trento M, Bajardi M, Borgo E, passera P, Maurino M, et al. (2002) Perceptions of diabetic retinopathy and screening procedures among diabetic people. Diabet Med 19(10): 810-813.
-
Krayem B, Zarea Al (2016) Knowledge, Attitude and Practice of Diabetic Retinopathy amongst the Diabetic Patients of Al Jouf and Hail Province of Saudi Arabia. J Clin Diagn Res 10(5): NC05-NC08.
-
Khandekar R, Al Harby S, Al Harthy H, Al Lawatti J (2010) Knowledge, attitude and practice regarding eye complications and care among Omani persons with diabetes - A cross sectional study. Oman J Ophthalmol 3(2): 60-65.
-
Abougalambou SSI, AbaAlkhail H, Abougalambou AS (2019) The knowledge, attitude and practice among diabetic patient in central region of Saudi Arabia. Diabetes Metab Syndr 13(5): 2975-2981.
- Investigation of Polymorphisms in PPAR-Ɣ and TRHR Genes and their Impact on Turkish Diabetic and Obese Individuals
- The Impact of Aircraft Noise Exposure on the Efficacy of Empagliflozin Therapy in an Animal Model of Obesity
- Rooibos Mitigates Metabolic and Inflammatory Dysfunctions in Mice Fed a High-Carbohydrate Diet
- Synergistic Effect of Combined Leaf Extract of Vernonia amygdalina, Ocimum gratissimum, and Zingiber officinale Tuber on Phytochemical Profile, Antioxidant Activity, Serum Insulin, and Biochemical Parameters in Streptozotocin-Induced Diabetic Rats
- Investigation of Cardiovascular Responses to Aerobic Exercise in Obese University Students
- A Look at the Phase Angle Obtained by Electrical Bioimpedance