Prevalence of Depression in Diabetes Mellitus Patients with Associated Co-Morbidities in Addis Ababa, Ethiopia, 2022
Background: Diabetes and depression are extremely common, devastating, and incapacitating diseases. Co-existing Depression in people with diabetes results in decreased adherence, poor health outcomes, higher diabetes complications, decreased quality of life, increased disability, and lost productivity with an increased risk of death. The aim of the study was to assess the prevalence of depression in Diabetes Mellitus patients with associated co-morbidities in Addis Ababa, Ethiopia, 2022. Methods: An institutional-based cross-sectional study design was conducted among 403 diabetes patients in the armed force general hospital, Addis Ababa, Ethiopia, from April to Jun 11, 2022. The participants were selected using systematic random sampling. Data was collected by face-to-face interview using a standardized and pretested questionnaire. Depression was assessed using the patient health questionnaire. Data was entered into EPI INFO and analyzed by SPSS version 25 software. Logistic regression analyses were performed to identify factors associated with depression, and a significant association was declared at a p-value less than 0.05 and a 95% confidence interval. Result: The study showed that the overall prevalence of depression was found to be 37.2% and respondents who had moderate social support (AOR = 2.429, 95% CI: 1.208–4.881), age 35 (AOR = 0.358, 95% CI: 0.181–0.706), age 45–54 (AOR = 0.431, 95% CI: 0.232–0.801), insulin users (AOR = 0.471, 95% CI: 0.227-0.976), metformin users (AOR = 0.104, 95% CI: 0.105-0.397), liver disease (AOR = 3.077, 95%CI: 2.437–7.265), and could read and write (AOR = 8.253, 95% CI: 3.278–24.527) were significantly associated with depression. Conclusion: This study demonstrated that the prevalence of depression among diabetes patients at Armed Forces General Hospital was found to be high. Furthermore, depression was associated with social support, age, anti-diabetic drug users, liver disease, and educational level. Different stakeholders, including hospital managers, health professionals, and different nongovernmental organizations, should give emphasis to linking depressive patients with hospitalization.
Introduction
Health is a state of complete physical, mental, and social well-being and not merely the absence of disease or infirmity. Mental health includes subjective well-being, perceived self-efficacy, autonomy, competence, intergenerational dependence, and recognition of the ability to realize one’s intellectual and emotional potential. Mental disorders such as depression, anxiety and substance abuse are common in chronic disorders, which can lead to poor health outcomes and failure to adhere to treatment plans [1].
Diabetes mellitus is a group of metabolic diseases characterized by increased levels of glucose in the blood (hyperglycemia) resulting from defects in insulin secretion, insulin action, or both (American Diabetes Association [ADA]). Normally, a certain amount of glucose circulates in the blood [2].
Depression is used to describe a range of moods – from low spirits to a severe problem that interferes with everyday life. The experience of depression is an overwhelming feeling which can make you feel quite unable to cope and hopeless about the future [3]. Depression can be very different in different people, or in the same person over time. It is a common but serious illnesses and treatment can help those with even the most severe depression get better [4].
Depression might have a severe impact on the course and prognosis of diabetes and should therefore be carefully diagnosed and treated early in the course of illness [5]. Diabetes and depression have a bidirectional relationship, i.e., diabetic patients are more likely to develop depressive disorders, while the normo-glycemic population has increased risk of acquiring a diabetic condition during their life time [6, 7, 8, 9].
Depression is a significant contributor to the global burden of disease and affects people in all communities across the world. Today, depression is estimated to affect 350 million people. The World Mental Health Survey, which was conducted in 17 countries, discovered that, on average about 1 in 20 people report having an episode of depression each year. While depression is the leading cause of disability for both males and females, the burden of depression is 50% higher for females than males. In fact, depression is the leading cause of disease burden for women in both high- income and low- and middle-income countries [10].
The coexistence of diabetes and mental disorders has a strong impact on the patient, with an increased risk of cardiovascular disease (CVD), all causes of mortality, especially as a result of cardiovascular complications of DM [11]. Diabetes mellitus is the third leading cause of death by disease, primarily because of the high prevalence of cardiovascular disease (myocardial infarction, stroke, and peripheral vascular disease). It affects about 17 million people, 5.9 million of whom are undiagnosed [12]. The overall prevalence of depression among diabetes patients at the diabetes clinic was reported to be 87% and most 56.7% had mild depression 22.1% had moderate depression, and 8.2% had severe depression [13].
Studies suggested that the prevalence of depression in Low and Middle-Income Countries and Sub-Saharan African countries was comparable with High-Income countries at around 10–20% of the population. However, the majority of people suffering from depression go untreated [14]. Despite research carried out in primary healthcare settings indicating a high prevalence of depression among facility attendees, particularly in the context of co-morbid chronic diseases, evidences were not sufficient at developing countries including Ethiopia specifically at armed force hospitals hence most of clients are militaries, those military personals have a stressful and risky life situation; including potential injury or death, witnessing the loss of human life, temporary campaign away from home, mission, frequent changes of home from place to place and exposure to dangerous equipment and materials which can potentially increase the risk of depression [14]. Therefore, the aim of this study was to assess the prevalence of depression and associated factors among diabetes mellitus patients at the armed force hospital in Addis Ababa, Ethiopia, 2021.
Methods
Study Area
The study was conducted at the armed forces hospital in Addis Ababa, Ethiopia. It was formerly known as Princess Tsehai Memorial Hospital, the hospital has 10 departments and 1100 clinical and supportive staff. Of those, 306 were military and the remaining were civil servants. The hospital has 460 beds and provides service to an annual average of 140,000 patients. There were around 520 diabetes mellitus patients with follow up at the chronic illness follow up clinic. It had psychiatry, surgical, medical, orthopedics, MDR, obstetrics, gynecology, and pediatric wards. There was also antenatal care, anti-retroviral therapy (ART) service, Operation Room (OR), Ear, Nose, and Throat (ENT), Dermatology, ophthalmology, dental, and emergency services. The study was conducted using an ethical clearance letter obtained from Yanet College. Full permission and acceptance letters were obtained from the armed forces hospital administration.
Design and Duration of the Study
An institution-based cross-sectional study was conducted from April to June 2022.
Study Population
Sampled patients with diabetes mellitus, who had follow-up at Armed Force Hospital chronic illness follow-up clinic during the study period.
Eligibility Criteria
- Inclusion Criteria Patients who were diagnosed with diabetes and had a follow-up age of more than 18 years.
- Exclusion Criteria Patients who were diagnosed with diabetes and had a serious illness and unable to communicate were excluded from the study.
Sample Size Determination
The sample size was estimated using a single population proportion formula. Considering 95% CI, 5% margin of error, and proportion of depression among diabetic patients 50% hence there were no previous studies in a similar setting.
Then we added a non-response rate of 5%, and it was finally 403.
The Technique and Procedure of Sampling
The lists of potential respondents were obtained from the updated registry book at the follow-up clinics of the armed force general hospital. Then, the study participants were selected by using a systematic random sampling technique in order of their appointments. The total number of diabetes mellitus patients who were on follow-up was 520 patients. So, the first patient was selected between the first and Kth interval, then we determined K value.
K=N/n, where N is the total number of diabetes mellitus patients. Then K was 520/403 = 1.29, then the study participants were selected from the 1st interval up to the maximum sample size that had been achieved from each diabetes mellitus patient who presented for follow up at the armed force general hospital’s chronic illness follow-up clinics.
Study Variables
- Dependent Variable Depression (presence or absence)
- Independent Variables Socio-demographic variables like age, sex, education status, monthly income, religion, occupation status, residence and marital status.
- Behavioral And Lifestyle Characteristics: alcohol consumption, cigarette smoking and chewing chats.
- Medical Related Characteristics: heart disease. blood pressure, lung disease, liver disease, Blood sugar level, and DM complications.
- Medication-Related Characteristics: insulin users and users of oral anti-diabetic medications.
- Social Characteristics: social support, stigma, duration of DM, and hospital admission.
- Physical Characteristics include limb loss, immobility, and mobility.
Data Collection Tools and Procedures
The data was gathered using a standardized questionnaire designed to assess depression in diabetic patients. This tool was not developed for clinical diagnosis. It is repeatable, sensitive and useful as a screening and surveillance tool for depression disorders, including diabetes patients (15). The questionnaire was used to assess prevalence and associated factors like socio-demographic characteristics, lifestyle and psychological factors to determine the depression of individuals with diabetes. The data was collected by a face- to-face interview using an Amharic language translated questionnaire.
Operational Definitions
Depression is a common mental disorder characterized by depressed mood, loss of interest or pleasure, decreased energy, feelings of guilt or low self-worth, disturbed sleep or appetite, and poor concentration. Moreover, depression often comes with symptoms of anxiety [10]. The PHQ-9 scoring system was used to assess depression in patients with established. The PHQ-9 subscale is classified as:
- There is no depression: less than 0 [15].
- Minimal depression: Study participants who had a score of 1-4 from PHQ 9 total score [15].
- Mild depression: diabetes patients with a PHQ 9 total score of 5-9 [15].
- Moderate depression: diabetes patients with a PHQ-9 total score of 10-14 [15].
- Moderately severe depression: a diabetic patient with a total score of 15-19 on the PHQ-9 [15].
• Severe depression: a DM patients who had score 20-27 from PHQ 9 total score [15].
Diabetes mellitus is a metabolic disorder of multiple etiologies characterized by chronic hyperglycemia with disturbances of carbohydrate, fat, and protein metabolism resulting from defects in insulin secretion, insulin action, or both [16]. Major Depressive Disorder (MDD) is characterized by discrete episodes of at least 2 weeks’ duration (although most episodes last considerably longer) involving clear-cut changes in affect, cognition, and neurovegetative functions and inter-episode remissions [17]. The (Oslo scale social support 3 item) OSSS-3 sum score can be operationalized into three broad categories of social support [18] Poor social support: 3-8 Moderate social support: 9-11 Strong social support: 12-14 Stigma is defined as “a mark of shame, disgrace, or disapproval which results in an individual being rejected, discriminated against, and excluded from participating in a number of different areas of society [19].
Quality Assurance of Data
The quality of data was assured before, during, and after the data collection. Before data collection, the questioners were pretested on 5% of the target population to evaluate the reliability and validity of the study prior to the final distribution and then after the data collection. The questionnaire was prepared first in English and then translated into Amharic, finally retranslated back to English to check for consistency. Two days of training were given for data collectors based on prepared training manuals, and how to use field guiding, procedure of data collection, and review of key terminologies, and ethical issues of the study were discussed in detail by the principal investigator prior to the actual data collection period.
During the data collection period, the collected data was checked for completeness and for its consistencies by the principal investigators and supervisors every night of data collection. For the duration of their appointment, patients were seen once a month. After the data collection, the collected datasets were rechecked for their completeness and consistency by the supervisors and principal investigators.
Data Processing and Analysis
After checking the collected data visually for completeness, the response was coded and entered into the computer using EPI Info version 7.1 Statistical Packages.
Then printed frequencies were used for outlier checking and for cleaning data. The data was cleaned accordingly and then exported to SPSS version 25 for further analysis. The frequency distributions of dependent and independent variables were workout and presented in tables and figures. The associated factors were identified using bivariate and multivariate logistic regression analysis.
Results
Socio-Demographic Characteristics of the Study Participants
| Variable | Category | Frequency (n=403) | Percent (%) |
|---|---|---|---|
| Sex | Male | 291 | 72.2 |
| Sex | Female | 112 | 27.8 |
| Age in year | 18-34 | 43 | 10.7 |
| Age in year | 35-44 | 96 | 23.8 |
| Age in year | 45-54 | 102 | 25.3 |
| Age in year | >=55 | 162 | 40.2 |
| Religion | Muslim | 65 | 16.1 |
| Religion | Orthodox | 218 | 54.1 |
| Religion | Protestant | 113 | 28 |
| Religion | Catholic | 6 | 1.5 |
| Religion | Jubbah | 1 | 0.2 |
| Marital status | Married | 269 | 66.7 |
| Marital status | Single | 80 | 19.9 |
| Marital status | Divorced | 30 | 7.4 |
| Marital status | Widowed | 16 | 4 |
| Marital status | Separated | 8 | 2 |
| Educational status | Can read and write (Informal education) | 12 | 3 |
| Educational status | 1-8 grade | 44 | 10.9 |
| Educational status | 9-12 grade | 161 | 40 |
| Educational status | Diploma and above | 186 | 46.2 |
| Occupation | Active military | 231 | 57.3 |
| Occupation | Medical bored | 52 | 12.9 |
| Occupation | Pension | 120 | 29.8 |
| Residence | Urban | 290 | 72 |
| Residence | Rural | 113 | 28 |
| Monthly Income (ETB) | <1500 | 1 | 0.2 |
| Monthly Income (ETB) | 1500-3000 | 113 | 28 |
| Monthly Income (ETB) | 3001-4500 | 129 | 32 |
| Monthly Income (ETB) | 4501-6000 | 96 | 23.8 |
| Monthly Income (ETB) | >6001 | 64 | 15.9 |
Table 1: Socio-demographic characteristics of Armed Forces General Hospital Addis Ababa, Ethiopia 2022 study participants (n=403)
A total of 403 participants took part with a response rate of 100%. About 291 (72.2%) of the participants were males, and a higher percentage 218 (54.1%) of the participants were orthodox in religion. 269 (66.7%) of the respondents were married, and 186 (46.2%) of the participants had completed their diploma and above. Concerning their occupation, 231 (57.3%) of the participants were active military. Of the total respondents, 162 (40.2%) were over the age of 55. The largest proportion129 (32.0%) of the respondents had an income of 3001-4500 Ethiopian Birr (ETB) per month and 290 (72.0%) of respondents lived in urban areas (Table 1).
Social, Behavioral, and Lifestyle Characteristics of Respondents
Of the total respondents, 224 (55.6%) had moderate social support and nearly two-thirds (61.3%) of the interviewers had less than eight years of diabetes mellitus duration. Of the total respondents (178, 44.2%) had a history of hospital admitting and 48 (11.9%) were drank alcoholic beverages. Around 30 (7.4%) respondents were smoking cigarettes and 35 (8.7%) were chewing chat (Table 2).
| Category | Frequency (n=403) | Percent (%) | |
|---|---|---|---|
| Social support | Poor | 96 | 23.8 |
| Social support | Moderate | 224 | 55.6 |
| Social support | Strong | 83 | 20.6 |
| Duration of diabetic mellitus(in year) | <8 | 247 | 61.3 |
| Duration of diabetic mellitus(in year) | Sep-16 | 114 | 28.3 |
| Duration of diabetic mellitus(in year) | >17 | 42 | 10.4 |
| Hospital admission | Yes | 178 | 44.2 |
| Hospital admission | No | 225 | 55.8 |
| Do you drink alcoholic beverage? | Yes | 48 | 11.9 |
| Do you drink alcoholic beverage? | No | 355 | 88.1 |
| Dou you smoke cigar ate? | Yes | 30 | 7.4 |
| Dou you smoke cigar ate? | No | 373 | 92.6 |
| Do you chew chat? | Yes | 35 | 8.7 |
| Do you chew chat? | No | 368 | 91.3 |
Table 2: Social, behavioral, and lifestyle characteristics of study participants at the Armed Forces General Hospital in Addis Ab
Medical and Medication Characteristics of Respondents
The majority of study participants 264 (65.5%) fasting blood glucose levels was normoglycemic (euglycemic) and 73 (18.1%) developed diabetes mellitus complications.
Over half of the study participants (227, 56.3%) were taking metformin oral anti-diabetic medication and 15 (3.7%), 91 (22.6%), 39 (9.7%) 16 (4.0%), and 12 (3.0%) of participants had heart disease, HTN, lung disease, kidney disease, and liver disease (Table 3).
| Category | Frequency (n=403) | Percentage (%) | |
|---|---|---|---|
| Heart disease or problems? | Yes | 15 | 3.7 |
| Heart disease or problems? | No | 388 | 96.3 |
| High blood pressure or Hypertension? | Yes | 91 | 22.6 |
| High blood pressure or Hypertension? | No | 312 | 77.4 |
| Lung disease or problems (such as Asthma, TB, Pneumonia or others | Yes | 39 | 9.7 |
| Lung disease or problems (such as Asthma, TB, Pneumonia or others | No | 364 | 90.3 |
| Kidney disease? | Yes | 16 | 4 |
| Kidney disease? | No | 387 | 96 |
| Liver disease? | Yes | 12 | 3 |
| Liver disease? | No | 391 | 97 |
| Fasting blood sugar level? | Normoglycemic | 264 | 65.5 |
| Fasting blood sugar level? | Hyperglycemic | 117 | 29 |
| Fasting blood sugar level? | Hypoglycemic | 22 | 5.5 |
| Diabetics’ mellitus complication? | Yes | 73 | 18.1 |
| Diabetics’ mellitus complication? | No | 330 | 81.9 |
| Types of drug taking currently? | Insulin | 92 | 22.8 |
| Types of drug taking currently? | Metformin | 227 | 56.3 |
| Types of drug taking currently? | Metformin and glimepiride | 84 | 20.8 |
Table 3: Medical and medication-related characteristics of the study participants at Armed Forces General Hospital, Addis Ababa,
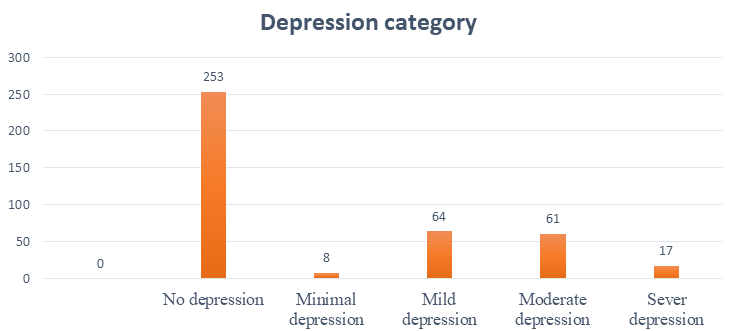
Depression-Related Characteristics
Of the total respondents, 64 (15.9%) were mild depressed, 61 (15.1%) moderate depressed, 17 (4.2%) of the respondents were severely depressed, 8 (2.0%) minimal depression, and there was no severe depression. In this study, the PHQ-9 measurement tool yielded a total score of 253, indicating that there was no depression (62.8%) (Figure 1).
Bivariate Analysis of Factors Associated with Depression among Patients with Diabetes Mellitus
Those variables performed in the bivariate analysis with p-values less than 0.25 were candidate for multivariate analysis. To identify independent predictors for depression among the participants of 403, from the variables social support, Age, diabetes medication users, liver disease, physical mobility and educational status were associated with depression (Table 5).
| Depression | No depression | COR (95%CI) | P-value | |
|---|---|---|---|---|
| Social support category | ||||
| Poor social support | 39(40.6) | 57(59.4) | 1.897(1.005-3.581) | 0.048 |
| Moderate social support | 89(39.7) | 135(60.3) | 1.828(1.048-3.188) | 0.033 |
| Strong social support | 22(26.5) | 61(73.5) | 1 | |
| Current age category | ||||
| Age 18-34 | 3(7.0) | 40(93.0) | 0.049(0.015-0.165) | 0 |
| Age 35-44 | 20(20.8) | 76(79.2) | 0.172(0.096-0.308) | 0 |
| Age 45-54 | 29(28.4) | 73(71.6) | 0.259(0.152-0.442) | 0 |
| Age>55 | 98(60.5) | 64(39.5) | 1 | |
| Diabetic treatment regime | ||||
| Insulin user | 39(42.4) | 53(57.6) | 0.294,(0.157-0.552) | 0 |
| Metformin user | 51(22.5) | 176(77.5) | 0.116,(0.066-0.204) | 0 |
| Metformin & glimepiride user | 60(71.4) | 24(28.6) | 1 | |
| Physical mobility | ||||
| Yes | 116(32.0) | 246(68.0) | 0.097 (0.042-0.226) | 0 |
| No | 34(82.9) | 7(17.1) | 1 | |
| Liver disease | ||||
| Yes | 10(83.3) | 2(16.7) | 8.964 (1.937-4.490) | 0.005 |
| No | 140(35.8) | 251(64.2) | 1 | |
| Current educational status category | ||||
| Can read and write (informal education) | 11(91.7) | 1(8.3) | 21.476 (2.711-17.112) | 0.004 |
| 1-8 grad | 17(38.6) | 27(61.4) | 1.229 (0.624-2.423) | |
| 9-12 grad | 59(36.6) | 102(63.4) | 1.129(0.726-1.756) | 0.551 |
| Diploma and above | 63(33.9) | 123(66.1) | 1 | 0.589 |
Table 5: Bivariate analysis of study participants at Armed Forces General Hospital, Addis Ababa, Ethiopia, 2021 (n = 403).
Multivariate Analysis Results for Factors Associated with Depression among Patients with Diabetes Mellitus
Multivariate analysis was performed to identify independent predictors for depression among the participants. In multivariate analysis, variables with p 0.05 were declared significantly associated with depression. Consequently, respondents who had social support, age, diabetes medication users, liver disease, and educational status were determined.
Those patients with moderate social support were 2.43 times more likely to have depression than those who had strong social support (AOR = 2.429, 95% CI: (1.208-4.881). Those patients who were insulin users were 53% less likely to have depression compared to those patients on metformin and glimepiride (AOR = 0.471, 95% CI: 0.227-0.976).
Those patients who were liver diseased were 3 times more likely to be depressed than those patients who had no liver disease (AOR = 3.077, 95% CI: 2.437–7.165). Those patients who could read and write were 8.25 times more
- likely to be depressed compared to those patients who had a diploma and above (AOR = 8.253, 95% CI: 3.278–24.527)
- (Table 6).
- Variable
- Depression
- No depression
- AOR (95%CI) p-value
- Social support category
- Poor social support
- 39(40.6)
- 57(59.4)
- 1.975(0.876-4.454)
- 0.101
- Moderate social support
- 89(39.7)
- 135(60.3)
- 2.429(1.208-4.881)
- 0.013
- Strong social support
- 22(26.5)
- 61(73.5)
- 1
- Current age category
- Age 18-34
- 3(7.0)
- 40(93.0)
- 0.106(0.029-0.383)
- 0.001
- Age 35-44
- 20(20.8)
- 76(79.2)
- 0.358(0.181-0.706)
- 0.003
- Age 45-54
- 29(28.4)
- 73(71.6)
- 0.431(0.232-0.801)
- 0.008
- Age>=55
- 98(60.5)
- 64(39.5)
- 1
- Diabetic treatment regime
- Insulin user
- 39(42.4)
- 53(57.6)
- 0.471(0.227-0.976)
- 0.043
- Metformin user
- 51(22.5)
- 176(77.5)
- 0.204(0.105-0.397)
- 0
- Metformin and glimepiride user
- 60(71.4)
- 24(28.6)
- 1
- Physical mobility
- Yes
- 116(32.0)
- 246(68.0) no
- 34(82.9)
- 7(17.1)
- 0.223(0.088-0.563)
- 0.001
- 1
- Liver disease
- Yes
- 10(83.3)
- 2(16.7) no
- 140(35.8)
- 251(64.2)
- 3.077(2.437-7.165
- 0.003
- Current educational status category
- Can read and write
- 11(91.7)
- 1(8.3)
- 8.253(3.278-24.527)
- 0.002
- 1-8 grad
- 17(38.6)
- 27(61.4)
- 1.679(0.686-4.113)
- 0.257
- 9-12 grade
- 59(36.6)
- 102(63.4)
- 1.082(0.633-1.850)
- 0.774
- Diploma and above
- 63(33.9)
- 123(66.1)
- 1
Table 6: Multivariate analysis of the study participants at Armed Force General Hospital, Addis Ababa, Ethiopia, 2022 (n = 403)
Discussion
This study showed that the overall prevalence of depression was found to be (37.2%), moreover social support, age, educational level, liver disease and anti-diabetes drug users were significantly associated with depression The finding of the current study was in line with a cross-sectional study done in Mizan Tepi University Hospital(37%) [20].
However the present study was lower than a cross- sectional study conducted in Palestine primary health care center(40%) [8] in Egypt suz canal hospital (69.0%) [21], in Ethiopia metanalysis research overall prevalence(39.73%) (22), in Bahirdar Felege Hiwot specialized hospital 40.40% [23] and Jimma University specialized hospital 43.6% [5].
The discrepancy might be due to different assessment tools, health service delivery systems, educational status, lifestyle, and social interaction. For example in Egypt, the MADRS screening tool was used for assessing depression. In the study of Ethiopia (Felege-Hiwot Referral hospital and Jimma University Specialized Hospital), Beck depression inventory (BDI II) was used to assess depression. The other reason for the difference might be due to difference with study settings and participants. For example, the study in Egypt was done among individuals with Type 2 DM [24].
On the other hand, the result of this study was relatively higher than studies conducted in Spain Madrid 20.03% [11]. Victoria hospital 19.9% [7], Nepal (27%) [25], University of Gondar diabetic clinic 15.4 %[26], Black-Lion Specialized Hospital 13% [12], Meekly hider hospital(17%) [27], and Tirunesh Beijing general hospital Addis Ababa, Ethiopia (21.3%) [24].
One of the reasons for the difference might be the difference with health care settings and likely due to the cut-off score for PHQ-9 being 5. Besides, it could be due to variation in attributes of study participants, use of different psycho metric scale, study design, time frame and sample size. The second objective of this study was to identify the associated factors of depression among patients with diabetes mellitus. Accordingly, the odds of developing depression among diabetic patients who have moderate social support were two times more likely when compared to clients who have strong social support. This finding was similar to the study conducted in Bahirdar Ethiopia at Felege- Hiwot referral hospital [28] and Tirunesh Beijing general hospital [24].
This might be due to the fact that social isolation reduces social support, which can have undesirable influence on physical and mental wellbeing. Having moderate social support may leads to delayed diabetic treatment. If the treatment is delayed, the patient will have an early sign of diabetic-related complication which predispose the patient to different psychiatric disorders including depression. The odds of educational status with respondents who can read and write were 8.25 times more likely to have depression compared to those who were diploma and above, similar study conducted in Palestine [8], Saudi Arabia [29] and Seri lanka [30] , this might be due to the difference in sample size, economic status and study setting.
The odds of anti-diabetes drug users’ respondents who were insulin users were 53% less likely to have depression compared to that of metformin users and glimipride, similar results were found with study conducted in Nepal [25], Bangladesh [31] and East Shewa Adama, Ethiopia [31], this might be due to the fact that respondents who were insulin users might have better social support and income.
In contrast to some other studies, this study showed no significant association between depression score with gender and marital status [30] this study showed no significant association between depression and participants monthly income which is contrary to other published studies [29], this study found that the duration of DM and residence was not significantly associated with depression which is consistent with the findings reported by other studies [20].
Finally, this study was not free of limitations due to lack of sophisticated screening tests, time and budget constraints, diabetes complications were not addressed in this and were not confirmed by respective specialists instead only by patient’s subjective response of complication was detected. As the study was a simple cross sectional study design, it was impossible to know the direction of cause-and-effect relationship of diabetic and depression. Data were collected by self-report rather than observation which could lead to recall and social desirability bias.
Conclusion
This study revealed a high prevalence of depression among diabetes patients in Addis Ababa, Ethiopia. Furthermore, depression had associated with social support, anti-diabetes drug users, liver disease, and educational level.
Recommendation
The finding of this study revealed that a significant number of diabetes patients had a high level of depression. These findings request for the need of integrated interventional management on diabetes mellitus and depression, which will increase health and wellbeing of the patients. Therefore, in order to reduce risk of depression among diabetes patients different stakeholders including Hospital managers, diabetic association, health professionals, health programmers, and different non-governmental organizations should give emphasis on linking depressive patients, to different supporting social groups, improving knowledge through health education on diabetes and depression.
Declaration
• Ethical consideration Ethical approval was obtained from Yanet College of research and ethical board. Permission letter was obtained from armed force hospitals. An informed written consent was obtained from each study participants. All respondents were informed that the participation was voluntarily. The potential benefits, harms, confidentiality, and the possibility of withdrawing from the interview at any time of interview and after were also informed.
- Consent for Publication Not applicable
- Data Availability The data used to support the findings of this study are available from the corresponding author upon request.
• Conflicts of Interest
The author declares they have no competing conflicts of interest.
• Funding The study has no funding source.
• Acknowledgement: We would like to thank armed force general hospital administrators, data collectors and study participants.
References
-
World Health Organization (2003) Investing in mental health.
-
Smeltzer SC, Hinkle JL, Bare BG, Cheever KH (2010) Textbook of Medical-surgical nursing. In: 12th
-
(Edn.), Lippincott Williams & Wilkins, New york, USA.
-
Borrill J (2020) Clinical Research Manager, Mental Health Foundation UK Office 83 Victoria Street London SW1H 0HW.
-
National Institute of Mental Health US (2020) Department of health & human services. 07-5084.
-
Dejene S, Negash A, Tesfay K, Jobst A, Abera M (2014) Depression and diabetes in jimma university specialized hospital, Southwest Ethiopia. African J Psychiatry 17(3).
-
Udedi M, Pence BW, Stewart RC, Muula AS (2020) Detection and prevalence of depression among adult type 2 diabetes mellitus patients attending non- communicable diseases clinics in Lilongwe, Malawi. Int J Ment Health Syst 14(1): 1-8.
-
Victoria GMB, Dampil AO (2019) Prevalence of Depression among Patients with Type 2 Diabetes Mellitus and its associated Clinical Factors 34(2): 197- 203.
-
Sweileh WM, Hadeed HM, Jabi SW, Zyoud SH (2014) Prevalence of depression among people with type 2 diabetes mellitus: A cross sectional study in Palestine. BMC Public Health 14(1).
-
Marcus M, Yasamy MT, Ommeren VM, Chisholm D (2012) Depression, a global public health concern. WHO Dep Ment Heal Subst Abus pp: 1-8.
-
Salinero FMA, Andrés FJS, Cárdenas VJ, Abánades HJC, Carrillo E, et al. (2018) Prevalence of depression in patients with type 2 diabetes mellitus in Spain (the DIADEMA Study): results from the MADIABETES cohort. BMJ Open 8(9): e020768.
-
Dejenie HT, Radie YT, Sharew NT (2015) Prevalence of depression among type 2 diabetic outpatients in black lion general specialized hospital, addis ababa, Ethiopia. Depress Res Treat 2015:184902.
-
Lutale J, Moledina SM (2019) Prevalence of Depression and Associated Factors among Diabetic Patients in an Outpatient Diabetes Clinic. Psychiatry J 2019:2083196.
-
Mayston R, Frissa S, Tekola B, Hanlon C, Prince M, et al. (2020) Explanatory models of depression in sub- Saharan Africa : Synthesis of qualitative evidence. Soc Sci Med pp: 112760.
-
(2020) Depression primary care.
-
Khatib, Oussama MN (2020) Guidelines for the prevention, management and care of diabetes mellitus. In: Oussama MN, Khatib P, et al (Eds.).
-
American Psychiatric Association (2013) Diagnostic and Statistical Manual of Mental Disorders. In: 5th (Edn.), Arlington VA, American Psychiatric Association.
-
Kocalevent R, Berg L, Beutel ME, Hinz A, Zenger M, et al. (2018) Social support in the general population: standardization of the Oslo social support scale (OSSS- 3). BMC Psychol 6(1): 31.
-
Paper TI, Paper TI, Statement P (2020) beyond blue Information Paper : Stigma and discrimination associated with depression and Executive summary. (P2): 1-35.
-
Asefa A, Zewudie A, Henok A, Mamo Y (2020) Depression and Its Associated Factors among Diabetes Mellitus Patients Attending Selected Hospitals in Southwest Ethiopia : A Cross-Sectional Study 2020: 6486030.
-
Ismail MFS, Fares MM, Alrhman AG (2019) Prevalence of Depression and Predictors of Glycemic Control among Type 2 Diabetes Mellitus Patients at Family Medicine Clinic, Suez Canal University Hospital Egypt. World Fam Med Journal/Middle East J Fam Med 17(2): 4-13.
-
Teshome HM, Ayalew GD, Shiferaw FW, Leshargie CT, Boneya DJ (2018) The Prevalence of Depression among Diabetic Patients in Ethiopia: A Systematic Review and Meta-Analysis, 2018. Depress Res Treat 2018: 6135460.
-
Engidaw NA, Wubetu AD, Basha EA (2020) Prevalence of depression and its associated factors among patients with diabetes mellitus at Tirunesh-Beijing general hospital, Addis Ababa, Ethiopia. BMC Public Health 20: 266.
-
Subedi S, Adhikari A, Paudel K, Shrestha L, Shrestha S, et al. (2020) Depression in Patients with Diabetes Mellitus : Prevalence & Factors Associated 9(1): 16-22.
-
Birhanu AM, Alemu FM, Ashenafie TD, Balcha SA, Dachew BA (2016) Depression in diabetic patients attending university of gondar hospital diabetic clinic, Northwest Ethiopia. Diabetes, Metab Syndr Obes Targets Ther 9: 155-62.
-
Mossie TB, Berhe GH, Kahsay GH, Tareke M (2017) Prevalence of depression and associated factors among diabetic patients at Mekelle City, North Ethiopia. Indian J Psychol Med 39(1): 52-58.
-
Dar B, Dar B (2019) Patients Attending Outpatient Department , at Felege Hiwot Referral Hospital , International Journal of Health Sciences and Research Prevalence of Depression and Associated Factors among Adult Diabetic Patients Attending Outpatient Department , at Felege .
-
Madkhali JM, Hakami AA, Dallak AH, Hakami RM, Yatimi AA, et al. (2020) Prevalence and Associated Factors of Depression among Patients with Diabetes at Jazan Province, Saudi Arabia : A Cross-Sectional Study. Psychiatry J 2019: 6160927.
-
Arambewela MH, Somasundaram NP, Buddhi H, Ranjan P, Kumbukage MP (2019) Prevalence of Depression and Associated Factors among Patients with Type 2 Diabetes Attending the Diabetic Clinic at a Tertiary Care Hospital in Sri Lanka : A Descriptive Study. Psychiatry J 2019: 7468363.
-
Rahman M, Rahman A, Flora MS (2011) Urban hospital of Bangladesh Depression and associated factors in diabetic patients attending an urban hospital of Bangladesh. pp: 65-76.
-
Tusa BS, Alemayehu M, Weldesenbet AB, Kebede SA, Dagne GA (2020) Prevalence of Depression and Associated Factors among Diabetes Patients in East Shewa , Ethiopia : Bayesian Approach. Depress Res Treat 2020: 4071575.
- Investigation of Polymorphisms in PPAR-Ɣ and TRHR Genes and their Impact on Turkish Diabetic and Obese Individuals
- The Impact of Aircraft Noise Exposure on the Efficacy of Empagliflozin Therapy in an Animal Model of Obesity
- Rooibos Mitigates Metabolic and Inflammatory Dysfunctions in Mice Fed a High-Carbohydrate Diet
- Synergistic Effect of Combined Leaf Extract of Vernonia amygdalina, Ocimum gratissimum, and Zingiber officinale Tuber on Phytochemical Profile, Antioxidant Activity, Serum Insulin, and Biochemical Parameters in Streptozotocin-Induced Diabetic Rats
- Investigation of Cardiovascular Responses to Aerobic Exercise in Obese University Students
- A Look at the Phase Angle Obtained by Electrical Bioimpedance