Growth Hormone and Growth Retardation in Autoimmune Type-1 Diabetes. Insulin an Important Endocrine Growth Factor
Growth hormone (GH) secretory alterations and dysregulations with insulin-like growth factor-I (IGF-1) axis among type-1 diabetic children and adolescents is well established. In this poorly controlled abnormal metabolic state, GH hypersecretion is observed with decreased levels of Insulin-like Growth Factors (IGFs), IGF binding proteins-3 (IGFBP-3), and growth hormone binding protein (GHBP). These all factors results in decreased growth velocity and growth retardation in type-1 diabetic children and adolescents. Insulin is the most important metabolic regulator of this system. Absolute insulin deficiency, as observed in type-1 diabetics, is the primary cause of this dysregulation and alterations. Several published studies have shown that elevated HbA1c and poor glycaemic control are the main factors of this abnormal metabolic state. Conversely, studies have also demonstrated that good glycaemic control with basal bolus insulin regimens or insulin pump can improve diabetic state with restoration of normal growth. Hence this perspective review focuses on these important aspects of growth abnormalities in type-1 diabetic patients and concludes that health care policy makers should develop a close monitoring program and system with multi-disciplinary team approach to prevent further diabetes related growth complications.
Introduction
Pathophysiological and Hormonal Aspects of Linear Growth in Type-1 Diabetics
Epidemiological studies have shown that nearly 60 % of patients with type-1 diabetes are diagnosed before the age of 15 years. In Western countries type-1 diabetes accounts approximately 90% of cases of childhood and adolescent diabetes [1]. There are multiple causes of growth failure in Type-1 Diabetes Mellitus (DM). One of the examples of severe form of growth failure is Mauriac syndrome; however, now this is rare [2].
Mammosomatotroph cells expressing both PRL and GH arise from the acidophilic stem cells which are located mainly in the lateral wings of the anterior pituitary gland; here they comprise 35% to 45% of all pituitary cells. The pituitary gland contains a total of 5 to 15 mg of GH. The genes of GH are located on the long arm of human chromosome 17q22-24. The GH is a single-chain polypeptide hormone consisting of 191 amino acids and synthesized by somatotroph cells. Neuropeptides, neurotransmitters, and opiates effect on the hypothalamus and modulate release of GHRH and somatostatin (somatotropin release–inhibiting factor [SRIF]). Complex and integrated effects of these neuropeptides determines the final secretory pattern of GH. These physiology of the growth hormone and insulin-like growth factor (GH-IGF) axis is demonstrated in Figure 1 and explained in further details in the text below.
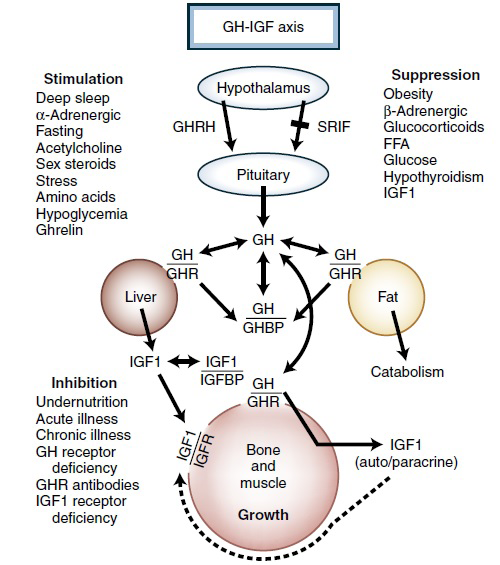
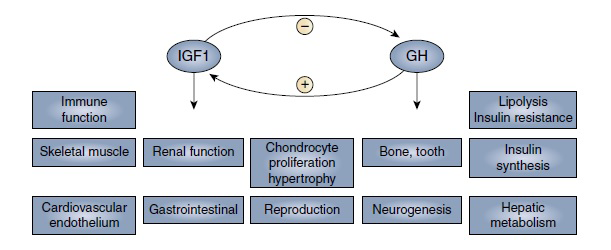
Figure-1: The growth hormone/insulin-like growth factor (GH-IGF) axis and hormones controlling GH release. IGFR, IGF1 receptor; FFA, free fatty acids; SRIF, somatotropin release–inhibiting factor (somatostatin). (From Rosenbloom A. Growth hormone insensitivity: physiologic and genetic basis, phenotype and treatment. JPediatr. 1999;135:280–289.) Insulin-like Growth Factors (IGFs) are a family of hormones produced mainly by the liver in response to growth hormone (GH). While IGF-2 enhances foetal development, IGF-1 (previously named somatomedin C) is important for postnatal growth, reaching its peak during puberty. IGFs are transported in the blood via IGF binding proteins (IGFBP). GH inhibit production of IGFBP-1 and -2 whereas stimulate IGFBP-3, -4 and -5. IGFBP-3 regulates bioavailability and half-life of the IGF-1 and its effects on tissues metabolism. GH is an important stimulant of IGF-1 and IGFBP-3 secretion via the liver. Hence levels of IGF-1 and IGFBP-3 may be low or decreased in hepatic failure. Similarly, Malnutrition, anorexia (and associated nutritional diseases such as coeliac disease) has a strong inhibitory effect on IGF-1, IGFBP-3 and ALS (acid labile subunit; see below text). In summary, IGF-1, IGFBP-3 and ALS are growth hormone responsive markers. Furthermore, GH is not the only stimulant for IGF-1 concentrations; other hormones such as insulin, thyroid hormone, androgens, and oestrogens at low concentrations stimulate IGF-1 release from hepatocytes [3, 4, 5, 6]. Major physiologic actions of GH and IGF-1 are regulated by a very sensitive negative feedback loop between hepatic IGF-1 production and pituitary growth hormone secretion; these are explained in Figure 2.
Insulin a Main Endocrine Regulator for GH/IGF Axis Programming
Most emphasizing, Insulin plays an important role in the regulation of GH/IGF axis by GH receptors expression, availability, downregulation and responsiveness in the liver and also modulates GH post-receptor cascades, leading to IGFs and IGFBPs synthesis [7]. Of note, IGF-1 activity is negatively regulated by IGFBP-1 concentrations. Hence Insulin potentially increases IGF-1 bioactivity via negative modulation of gene expression of IGFBP-1. IGFBP-3 was first discovered in 1986, the main IGF transport protein in the serum. A large and significant data demonstrates that type-1 diabetic state (absolute insulin deficiency) results in GH hypersecretion with low circulating levels of IGF-1 and IGFBP-3, with lack of upregulation of GH receptors (called Hepatic GH resistance) . Diminished GH receptors is reflected by diminished circulating GHBP levels with additional post- receptor defects in GH action [8, 9, 10, 11].
Furthermore, newly diagnosed type-1 diabetics have low concentrations of GH binding protein. Interestingly, treatment with insulin (with advanced analogue insulin regimes/basal bolus) or hyperinsulinemia restore GH binding protein levels in circulation, weight gain and accelerated linear growth. However, GH binding protein levels remain lower than the age matched normal subjects. These pathophysiological changes increase the risk of growth failure, as has been demonstrated in Mauriac syndrome (hepatomegaly, delay in growth and puberty, dyslipidaemia) [12, 13, 14, 15, 16, 17].
GH/IGF Alterations and Dysregulation in Type- 1 Diabetic State
The most important role of GH and IGFs is to increase bone length by augmentation of chondrocyte proliferation, maturation, hypertrophy and thus regulation of growth plate and matrix synthesis. Furthermore, GH also directly stimulates proliferation chondrocytes. Insulin deficiency with alterations in the GH-IGF axis, results in bone fragility in type-1 diabetic metabolic state. Furthermore, it has also been demonstrated that IGF-1 levels have a positive correlation with C-peptide (an endocrine metabolic marker of ß-cell function). Insulin deficiency or type-1 diabetic state is thus associated with decreased levels of IGF-1 [18, 19]. In this scenario, insulin is one of the most important endocrine hormone which regulates this entire osteology system [20, 21].
It has been demonstrated by Amiel SA, et al. [22] that elevated blood GH concentrations in poorly controlled type- 1 metabolic state are not helpful in IGF generation; and this endocrine defect is partially corrected by glycaemic control. They have demonstrated that “IGF I was low during conventional insulin therapy and rose within the week of intensified treatment (P < 0.001), despite a significant fall in mean 24-h growth hormone levels (P < 0.02)”. Moreover, it has been also demonstrated that over time IGF-1 levels fall among autoimmune type-1 diabetic patients who have multiple antibodies in the serum [18, 22].
Research conducted among pubertal subjects done by Rogers et al. has demonstrated significant negative association between IGF-1 and HbA1c levels (r = −0.45, P < 0.001), with no such associations in pre-pubertal subjects, and concluded that “glycemic control appears to strongly influence IGF-1 levels only after the onset of puberty”. Similarly, studies have also demonstrated a blunted somatomedin (SM) production and GH action in type-1 diabetics [23, 24, 25].
Alterations in Metabolic Homeostasis in Type-1 Diabetes
GH, IGF axis and serum insulin are important physiological metabolic and anabolic factors which promote weight gain with linear growth. Disorders in this interlinked anabolic system results in alterations in metabolic homeostasis. Insulin deficiency (as observed in type-1 DM) results in hepatic GH resistance (as observed by decreased IGF-1 production by liver) which causes increased production of IGF-binding proteins-1 (IGFBP-1) and IGFBP-2. Moreover, IGFs (especially IGF-1, IGF-2) enhances glucose metabolism. In addition to these important aspects, it should also be noted that GH mediates its affects via actions of peptides. As mentioned above, these peptides are IGF-1 and IGF-2 secreted by liver and bound to proteins (IGFBPs), importantly IGFBP-3, levels of which are GH-dependent. The GH/IGFs axis is such regulated that these binding proteins prolong the half-life of IGFs and transporting them to the target organs and making a ternary complex with the acid labile subunit (ALS), collectively called “Insulin-like growth factor binding protein, acid labile subunit” (IGFALS); this is encoded by the IGFALS gene and is stimulated by growth hormone [26, 27]. This ternary complex (ALS) inactivates both IGF-1 and IGFBP-3 and prolongs their half-life in the circulation.
Studies have demonstrated that optimal insulin concentrations are required to maintain normal serum concentrations of IGFs and IGFBPs and to promote normal growth. With absolute insulin deficiency in type-1 diabetics, alterations in GH-dependent proteins are observed in diabetics’ children and adolescents. Additionally, increased proteolysis of IGFBP-3 has been also observed in such patients with resultant decreased serum concentrations of intact IGFBP-3; serum ALS levels are also demonstrated to be diminished in insulinopenic untreated diabetic subjects. Hence, lack of IGF-1 feedback on GH secretion results in GH hypersecretion, which in turn decreases insulin sensitivity and cause hyperglycemia. After the discovery of insulin in 1920s, and thereafter in 1974, clinical researchers have found that at the diagnosis of type-1 diabetes, most children were taller than age matched non-diabetic children. This rapid growth was found to be associated with islet β-cell autoimmunity. However, pre-pubertal growth velocity was demonstrated to be lower in type-1 diabetics [28, 29, 30, 31].
GH hypersecretion also play a significant role in the development of vascular complications. However, these pathologic alterations are reversed by proper insulinization. In experimental studies, it has been demonstrated also that addition of IGF-1 treatment to such type-1 diabetic adolescents corrects GH hypersecretion, improves insulin sensitivity, decreases insulin requirements with improvement in glycemic control [32]. Research has also demonstrated that uncontrolled diabetes and long term higher HbA1c will result in reduced axial length and strict glycemic control is required in such patients [33]. In summary, Children and adolescents with poorly controlled type-1 diabetes significantly demonstrate lower growth velocity, especially in girls. Furthermore, these type-1 diabetics also exhibit low IGFBP-3 concentrations in the blood [34, 35, 36].
A recent study conducted in Germany and Austria between 1980 and 2000 in a cohort of 22,651 type-1 diabetic children has demonstrated a loss of 0.42 SDS (standard deviation score) during the entire period of the study. Hence health care policy makers should focus on this important aspect and cause of growth retardation in type-1 diabetic children and early intervention to optimize glycemic control, and to prevent further complication. These growth alterations can be restored by the newer insulin analogue basal bolus regimens with at least four injections per day. The physiologic insulin regimen is provided by longer acting basal insulins and rapid acting insulin analogues (RAIs) before each meal, with a multidisciplinary team approach, including diabetologist, endocrinologist, diabetic educator and dietitian. Insulin pump can also be used in resistant or erratic diabetic metabolic states [37].
Regarding type-1 diabetes among children and adolescents and its seriousness, investigators have linked decelerated growth velocity and short stature with microvascular complications as well, specifically diabetic nephropathy and retinopathy [38, 39]. Moreover, type-1 diabetes is associated with skeletal complications including decreased trabecular bone density. These bone complications are usually associated with other diabetic microvascular complications simultaneously [40].
Conclusion and Recommendations
It is recommended that in paediatric or adolescent diabetic patients, blood glucose should be controlled to achieve optimal goal for HbA1c. Insulin intensification is recommended to promote optimal growth. Recombinant human analog growth hormone is available since 1985 for the treatment of short stature [41, 42]. If specific diagnosis is not confirmed and child/adolescent is not achieving optima height, then GH–IGF axis should be clinically assessed with serum measurements of IGF-1 and IGFBP-3 concentrations. Furthermore, GH stimulation tests are recommended in diabetic patients with clinical evidence and family history of GH deficiency; and appropriate treatment should be initiated when specific aetiology is discovered [43]. However, if specific cause not found and patient is diabetic (especially type-1 autoimmune diabetes) efforts should be made to optimize HbA1c goal to near targets and achieving fasting and random blood glucose levels via intensive insulin therapy or basal bolus strategy to prevent growth and height delay or retardation and to prevent further diabetes associated complications [44]. Moreover, health care policy makers should develop a close monitoring program and system with multi-disciplinary team approach to avoid growth related disorders in type-1 diabetic children and adolescents.
Conflict of Interest
All authors declare no conflict of interest.
Acknowledgement
Authors are thankful for Eissa Ali Karn for his support for official documentation work.
Funding
This project was not funded by any organization and authors themselves reviewed the medical literature, collected data, written and edited the manuscript.
References
-
Atlas IDFID (2007) http://www.eatlas.idf.org/.
-
Kim MS, Quintos JB (2008) Mauriac syndrome: growth failure and type 1 diabetes mellitus. Pediatric endocrinology Reviews 5(S4): 989-993.
-
Hwa V, Oh Y, Rosenfeld RG (1999) The insulin-like growth factor-binding protein (IGFBP) superfamily. Endocrine Reviews 20(6): 761-787.
-
Weber MM, Auernhammer CJ, Lee PD, Engelhardt D, Zachoval R (2002) Insulin-like growth factors and insulin-like growth factor binding proteins in adult patients with severe liver disease before and after orthotopic liver transplantation. Hormone Research 57(3-4): 105-112.
-
Leung KC, Doyle N, Ballesteros M, Waters MJ, Ho KK (2000) Insulin regulation of human hepatic growth hormone receptors: divergent effects on biosynthesis and surface translocation. Journal of Clinical Endocrinology and Metabolism 85(12): 4712-4720.
-
Purandare A, Co Ng L, Godil M, Ahnn SH, Wilson TA (2003) Effect of hypothyroidism and its treatment on the IGF system in infants and children. Journal of Pediatric Endocrinology and Metabolism 16(1): 35-42.
-
Baxter RC, Martin JL (2018) Radioimmunoassay of growth hormone-dependent insulin like growth factor binding protein in human plasma. The Journal of clinical investigation 78(6): 1504-1512.
-
Nambam B, Schatz D (2018) Growth hormone and insulin-like growth factor-I axis in type 1 diabetes. Growth Hormone & IGF Research 38: 49-52.
-
Hill DJ, Milner RD (1978) Insulin as a growth factor. Pediatric research 19(9): 879-886.
-
Baxter RC, Turtle JR (178) Regulation of hepatic growth hormone receptors by insulin. Biochemical and Biophysical Research Communications 84(2): 350-357.
-
Daughaday WH, Phillips LS, Mueller MC (1976) The effects of insulin and growth hormone on the release of somatomedin by the isolated rat liver. Endocrinology 98(5): 1214-1219.
-
Maes LM, Underwood E, Ketelslegers JM (1986) Low serum somatomedin-C in insulin-dependent diabetes: evidence for a postreceptor mechanism. Endocrinology 118(1): 377-382.
-
Holly JMP, Biddlecombe RA, Dunger DB, et al. (1988) Circadian variation of GH-independent IGF-binding protein in diabetes mellitus and its relationship to insulin. A new role for insulin?. Clinical Endocrinology 29(6): 667-675.
-
Holl RW, Siegler B, Scherbaum WA, Heinze E (1993) The serum growth hormone-binding protein is reduced in young patients with insulin-dependent diabetes mellitus. Journal of Clinical Endocrinology and Metabolism 76(1): 165-167.
-
Arslanian SA, Menon RK, Gierl AP, Heil BV, Foley TP (1993) Insulin therapy increases low plasma growth hormone binding protein in children with new-onset Type 1 diabetes. Diabetic Medicine 10(9): 833-838.
-
Dunger DB, Cheetham TD (1996) Growth hormone insulin-like growth factor I axis in insulin-dependent diabetes mellitus. Hormone Research 46(1): 2-6.
-
Najjar S, Ayash MA (2020) The Mauriac syndrome. Clinical Pediatrics 13(9): 723-725.
-
Shapiro MR, Wasserfall CH, McGrail SM, Posgai AL, Bacher R, et al. (2020) Insulin-like growth factor dysregulation both preceding and following type 1 diabetes diagnosis. Diabetes 69(3): 413-423.
-
Hedman CA, Frystyk J, Lindstrom T, Chen JW, Flyvbjerg A, et al. (2004) Residual beta-cell function more than glycemic control determines abnormalities of the insulin-like growth factor system in type 1 diabetes. J Clin Endocrinol Metab 89(12): 6305-6309.
-
MacRae E, Wong SC, Farquharson C, Ahmed SF (2006) Cytokine actions in growth disorders associated with pediatric chronic inflammatory diseases. International Journal of Molecular Medicine 18(6): 1011-1018.
-
McCabe L, Zhang J, Raehtz S (2011) Understanding the skeletal pathology of type 1 and 2 diabetes mellitus. Critical Reviews in Eukaryotic Gene Expression 21(2): 187-206.
-
Amiel SA, Sherwin RS, Hintz RL, Gertner JM, Press CM, et al. (1984) Effect of diabetes and its control on insulin- like growth factors in the young subject with type I diabetes. Diabetes 33(12): 1175-1179.
-
Giustina A, Wehrenberg WB (1994) Growth hormone neuroregulation in diabetes mellitus. Trends in Endocrinology & Metabolism 5(2): 73-78.
-
Lanes R, Recker B, Fort P, Lifshitz F (1985) Impaired somatomedin generation test in children with insulin- dependent diabetes mellitus. Diabetes 34(2): 156-160.
-
Sönksen P, Jones RDH, Jones RH (1993) Growth Hormone and Diabetes mellitus. Horm Res 40: 68-79.
-
Butler J, Fitzgerald K, Hinkle G, Bettencourt B, Xu H (2019) Insulin-like growth factor binding protein, acid labile subunit (IGFALS) compositions and methods of use thereof. Alnylam Pharmaceuticals Inc 10,494,632.
-
Giannini C, Mohn A, Chiarelli F (2014) Growth abnormalities in children with type 1 diabetes, juvenile chronic arthritis, and asthma. International Journal of Endocrinology 265954.
-
Drayer NM (1974) Height of diabetic children at onset of symptoms. Archives of disease in childhood 49(8): 616- 620.
-
Songer TJ, LaPorte RE, Tajima N, Orchard TJ, Rabin BS, et al. (1986) Height at diagnosis of insulin dependent diabetes in patients and their non-diabetic family members. Br Med J 292(6533): 1419-1422.
-
Group ESS (2002) Rapid early growth is associated with increased risk of childhood type 1 diabetes in various European populations. Diabetes Care 25(10): 1755- 1760.
-
Bizzarri C, Benevento D, Patera IP, Bongiovanni M, Boiani A (2013) Residual β-cell mass influences growth of prepubertal children with type 1 diabetes. Hormone Research in Paediatrics 80(4): 287-292.
-
Bereket AB, Lang CH, Wilson TA (1999) Alterations in the growth hormone-insulin-like growth factor axis in insulin dependent diabetes mellitus. Hormone and Metabolic Research 31(2-3): 172-181.
-
Liu CF, Chen SC, Chen KJ, Liu L, Chen YP (2021) Higher HbA1c may reduce axial length elongation in myopic children: a comparison cohort study. Acta Diabetologica 58(6): 779-786.
-
Brown M, Ahmed ML, Clayton KL, Dunger DB (1994) Growth during childhood and final height in Type 1 diabetes. Diabetic Medicine 11(2): 182-187.
-
Gunczler P, Lanes R, Esaa S, Paoli M (1996) Effect of glycemic control on the growth velocity and several metabolic parameters of conventionally treated children with insulin dependent diabetes mellitus. Journal of Pediatric Endocrinology and Metabolism 9(6): 569-575.
-
Batch JA, Baxter RC, Werther G (1991) Abnormal regulation of insulin-like growth factor binding proteins in adolescents with insulin-dependent diabetes. Journal of Clinical Endocrinology and Metabolism 73(5): 964- 968.
-
Bonfig W, Kapellen T, Dost A, Fritsch M, Rohrer T, et al. (2012) Growth in children and adolescents with type 1 diabetes. Journal of Pediatrics 160(6): 900-903.
-
Penfold J, Chase HP, Marshall G, Walravens CF, Walravens PA (1995) Final adult height and its relationship to blood glucose control and microvascular complications in IDDM. Diabet Med 12(2): 129-133.
-
Fava S, Azzopardi J, Watkins PJ, Hattersley AT (2001) Adult height and proteinuria in type 2 diabetes. Nephrology Dialysis Transplantation 16(3): 525-528.
-
Abdalrahaman N, McComb C, Foster JE, Mclean J, Lindsay RS, et al. (2015) Deficits in Trabecular Bone Microarchitecture in Young Women with Type 1 Diabetes Mellitus. J Bone Miner Res 30(8): 1386-1393.
-
Bang P, Bjerknes R, Dahlgren J, Dunkel L, Gustafsson J (2011) A Comparison of different definitions of growth response in short prepubertal children treated with growth hormone. Hormone Research in Paediatrics 75(5): 335-345.
-
Sprogøe K, Mortensen E, Karpf DB, Leff JA (2017) The rationale and design of TransCon Growth Hormone for the treatment of growth hormone deficiency. Endocrine connections 6(8): R171-181.
-
Cohen P, Rogol AD, Deal CL, Saenger P, Reiter EO (2007) Consensus statement on the diagnosis and treatment of children with idiopathic short stature: a summary of the Growth Hormone Research Society, the Lawson Wilkins Pediatric Endocrine Society, and the European Society for Paediatric Endocrinology Workshop. The Journal of Clinical Endocrinology & Metabolism 93(11): 4210- 4217.
-
Aziz KMA (2012) Management of type-1 and type-2 diabetes by insulin injections in diabetology clinics-a scientific research review. Recent Patents on Endocrine, Metabolic & Immune Drug Discovery 6(2): 148-170.
- Investigation of Polymorphisms in PPAR-Ɣ and TRHR Genes and their Impact on Turkish Diabetic and Obese Individuals
- The Impact of Aircraft Noise Exposure on the Efficacy of Empagliflozin Therapy in an Animal Model of Obesity
- Rooibos Mitigates Metabolic and Inflammatory Dysfunctions in Mice Fed a High-Carbohydrate Diet
- Synergistic Effect of Combined Leaf Extract of Vernonia amygdalina, Ocimum gratissimum, and Zingiber officinale Tuber on Phytochemical Profile, Antioxidant Activity, Serum Insulin, and Biochemical Parameters in Streptozotocin-Induced Diabetic Rats
- Investigation of Cardiovascular Responses to Aerobic Exercise in Obese University Students
- A Look at the Phase Angle Obtained by Electrical Bioimpedance