Ergonomic Force Analysis, based on the UNE-EN-1005-3 Method, for Crude Oil Production Plant Operators
The processes carried out by the operators in the crude oil production centers (CPF) of the oil sector require greater interaction when making a musculoskeletal movement in each operation, this implies manipulation and force or the combination of the two, during the time of exposure to this factor for several hours a day, generating different pathologies that represent damage to health, producing consequences of physical overload in each work cycle during the biomechanical action of the body by manipulation, force, push or pull. Based on the Nordic (CN) questionnaire, the operators present indicators of high and medium morbidity due to Musculoskeletal Injury (SCI), more than 62.4% of the operators in the CPF, show chronic pain causing absenteeism from work and loss in production, causing deterioration in health in the short, medium or long term. By applying the UNE-EN-1005-3 method, it allows evaluating each cycle of physiological movement by force. These disergonomic aspects need to be corrected in due time, preventing pathologies due to SCI both clinical and permanent or temporary disability, preventing damage to the back-lumbar or cervical area. An occupational medical control program can decrease morbidity and increase the organization productivity.
Guillermo Neusa Arenas1*, Jeanette del Pilar Ureña Aguirre2, Ramiro Vicente Saraguro3 and Soraya Nathali Puco Fonseca4
Introduction
Ergonomics is the science that relates the work environment and those who perform work by time cycles, i.e. workers. One of the fundamental objectives is to adapt a work space to the capabilities and environment in which the worker works during the working day, avoiding the presence of dysergonomic factors due to exposure. However, other dysergonomic factors can be generated by aspects that are interrelated with the worker; work environment, cognitive, organizational, and physiological type. All osteomuscular movements, can cause symptoms are a set of SCI as inflammatory or degenerative in the muscle, tendons, ligaments, joint and nerves, these diseases usually occur in the neck, upper back, lower back, shoulders, elbows and complemented by wrists and hands.
In the process of modernization, organizations have been developing in the international field of ergonomics. On the one hand, they have adopted the criteria and concepts issued by the International Ergonomics Association (IEA), in the simplest, most coherent and, above all, most applicable way. On the other hand, by ensuring a correlation between design, architecture, and visual elements, they are part of the control systems and in the macro processes of perception, which are included in the development of Ergonomics, for the prevention of dysergonomic factors both physiological and cognitive type [1].
In this way, the principles of ergonomics aim to adapt and adapt the spaces or areas that allow the worker to maintain an appropriate working environment during the working day [2].
On the other hand, the capacities of each operator in a crude oil production plant can prevent the appearance of health alterations that may arise as a consequence of an excessive physical load, whether high or low, “so the aim is to promote the health and safety of the worker, benefiting the functionality of the work cycle or system [3]. Working activities constitute a series of biomechanical movements performed by the operator, repetitive movements, and movement of loads, inadequate postures, push and pull and above all force; they are mechanisms of the body, which perform an osteomuscular effort and tension during biomechanical postural exposure [4].
Musculoskeletal pain is common and can affect more than one muscle. However, muscle pain symptoms can occur in other systems such as ligaments, tendons, and fascia. Fascias are part of the soft tissues, which connect to muscles, bones and organs [5].
Therefore, any muscle pain is often related to stress, muscle injury from overloading or exercise from physical exertion. Muscle pain symptomatology tends to involve some specific muscles, starting during the activity or after the activity. Often these symptoms cause pain in the short, medium and long term, where health prevention is required.
In the methodological principles of physical ergonomic assessment, several types of methods are present; to determine the exposure by Force; in the operators of the production centers (CPF), they are analyzed with the method UNE-EN: 1005-3, that we allows to establish the exposures needed for both specific conditions by task to be performed and exposure cycles (Force measured in Newtons) [6]. Muscle pain can generate a sign of pathology, affecting an organ throughout the body. For example, some disorders that affect tissues in the body (such as tendonitis) can cause pain or discomfort.
Materials and Methods
Determination of the Study Population
In the investigation by force analysis in the operators in the CPFs located in the Ecuadorian east, the following are determined: the population to be evaluated, work spaces, application of the Nordic questionnaire (NC) and evaluation methodology UNE-EN: 1005-3 [7].
To determine the finite sample in the population of CPFs, the Picker method is used [8].
N Z p q n d N Z p q
$$ n = \frac {N \times Z _ {\alpha^ {2}} \times p \times q}{d 2 \times (N - 1) + Z _ {\alpha 2} \times p \times q} $$
2 α ( )
2 2 1 α Where: N = population size Z = confidence level. P = probability of success, or expected ratio Q = probability of failure D = accuracy (Maximum permissible error in terms of proportion) When determining the calculation of the sample of 400 operators from the different areas, an average of 291 operators are considered, with a margin of error of 3% and reliability of 95%. In Table 1, he institutes the sample calculation.
| 3,0% | |
| ERROR MARGIN (common in auditing) | |
| PRELIMINARY POPULATION SIZE: | 400 |
| TRUST LEVEL (common in auditing): | 95% |
| Z-values (common in auditing): 90% | 95% |
| Variance (value to replace in the formula): 1.645 | 1,960 |
| Preliminary Sample Size= | 400 |
| Sample size Finita= | 291 |
Table 1: Calculation of the evaluated population.
Identification of Work Spaces
Choosing the results of the by the size of the finite sample of 291 operators from different companies in the oil production sector, table 2, represents the areas of study, by the number of operators:
| Operators | |
|---|---|
| Warehouse | 14 |
| Energy | 24 |
| Maintenance | 69 |
| Operations | 63 |
| Production | 36 |
| P Y O | 24 |
| Community Relations | 35 |
| SMA | 14 |
| TI | 12 |
Table 2: Identification of areas or spaces.
Nordic Questionnaire (NC) Iinstruments
During the analysis by musculoskeletal disorder (MSD) based on the NC in each of the operators (291) surveyed, and with the objective of validating the reliability by biomechanical exposure of body movement by Force, in the occupational clinical evaluation (OCE). “existing pathologies per operator, both of symptomatic origin and clinical picture, must be taken into account. (CN) de Kuorinka”- [9].
When determining a pathological or epidemiological clinical picture by force, “whether it is a stress load, it is not fully described if we do not know only its magnitude” [10, 11]. With the context of study of the CN, we can check the symptoms by clinical occupational picture (CCO), which originates the MSD or SCI. However, other aspects of initiation are analyzed as factors of analysis; age, gender and experience, elements that are part of the biomechanics and postural biometry, which allows to determine and check the duration of the working day cycles by exposure to Force, in table 3, aspects of identity of the operators are shown.
| Age | No Operators | Gender | No People | Experience | No People |
|---|---|---|---|---|---|
| 25-35 | 148 | Male | 198 | Yes | 238 |
| 36-45 | 69 | Female | 93 | No | 53 |
| 46 from now on | 74 | Total | 291 | Total | 291 |
| TOTAL | 291 |
Table 3: Identification of the population.
In graphs 1, 2 and 3, the study averages of the operators are analysed:
![Figure 1: Enhanced CN model. Source: Pizarro-2019 [12].](/fulltextimages/5582/fig_1.jpeg)
Graph 1: Average age.
Graph 2: Gender.
Graph 3: Experience in the oil sector.
The Kuorinka’s CN, standardized, allows to identify the detection and analysis of the symptoms by MSD or SCI, it is applicable in the analytical context in the ergonomics, with the purpose of checking the presence of CCO, of diagnosis, this allows us to determine if the operator presents or is presenting, some osteomuscular symptom, that can produce an occupational pathology. However, the evaluation allows us to establish information to estimate the level of risk factor in an appropriate, proactive way and to translate it into immediate actions by the occupational medicine [12].
Each NC question is a multiple choice question that can be used in one or two ways. A relation the autonomous form, allowing answering in a clear and concise way, without the absence of the pollster. On the other hand, in the second form, they are more explained by the interviewer as the development of the interview.
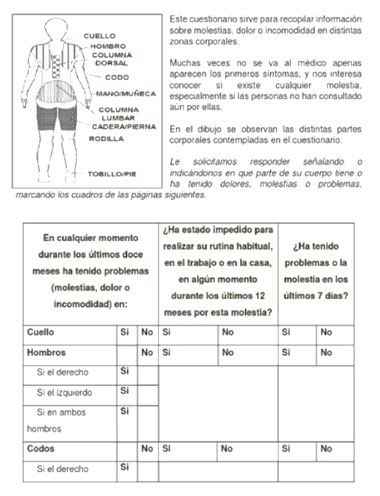
The consultations for each question are generally gathered by the symptomatology and pathology present in the operator, which on many occasions are detected in different activities by work cycles. In figure 2, the reliability of the NC, and its characteristics defined in the efforts made in the working day cycles, presents in real form the frequency of responses in time. Therefore, the CN is used in the occupational health units in the organizations, to select MSD information from the work areas that affect the operator with symptoms such as; about muscular pain, fatigue or the discomfort in anatomical zones to the osteomuscular movement.
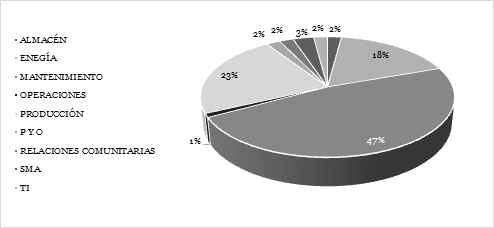
In graph 4, the % of interviews per NC is established, giving as results the personnel per area:
Graph 4: Staff interviewed by area.
Evaluation Methodology UNE-EN: 1005-3: 2020
When applying the procedure detailed in this European regulation, based on the revised NIOSH equation, it includes some technical criteria from other methodologies, defined in three steps [13]: Evaluation of activities by manual load handling work cycle:
- Checklist
- Estimation by means of tables
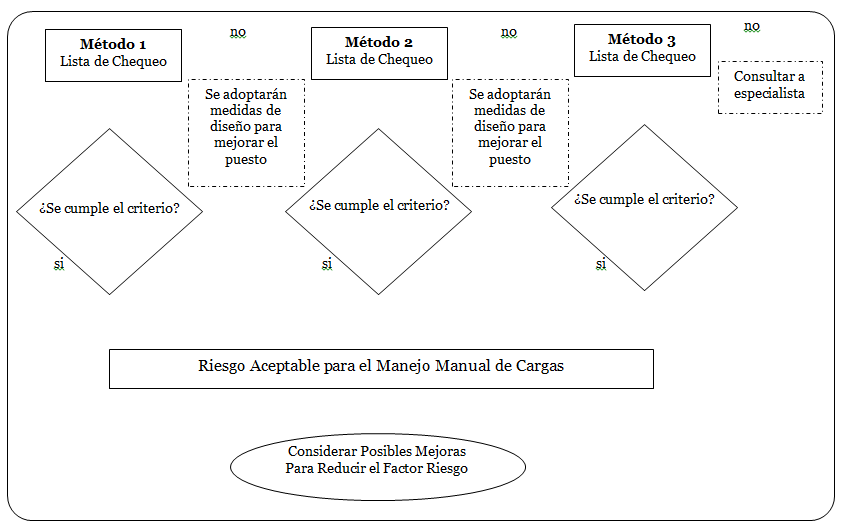
- Analytical calculation. When determining each of the procedures, graph 5, the decision tree is set as three methods of application;
Graph 5: Decision application method diagram.
In step 1; they consider the working mass constant as: a. Identify the user group. b. Select the mass constant (MC) according to the user group.
In Step 2; they define the risk assessment to be performed: a. Moderate thermal environment. b. Unrestricted standing position. c. Gentle lifting d. Good foot-to-floor coupling.
e. The object to be handled is not cold, hot or contaminated Continued: a. If one or more of these assumptions are not met, consult an expert. b. If all of the assumptions are met, assess the risk: 1. calculating the recommended mass limit (RML) 2. calculating the risk index (RI) RMLI=MC x HM x VM x DM x AM x CM x FM x 1HM x 2PM x NM $$ R I = \frac {M A S A R E A L}{R M L I} $$ Calculation from the RMLI (method 2): RML = RMLI × 1HM × 2PM × NM Where: 1HM is the multiplier for one hand 1HM = 0.60 2PM is the multiplier for two people 2PM = 0.85 NM is the multiplier for secondary tasks NM = 0.80 Calculation of the RML:
$$ R M L = M C \times \left(\frac {2 5}{H}\right) \times \left(\frac {1 - 0 . 0 0 3}{V - 7 5}\right) \times \left(0. 8 2 + \frac {4 . 5}{D}\right) \times \left(1 - 0. 0 0 3 2 \times A\right) \times C M \times F M \times 1 H M \times 2 P M \times N M $$ Where; MC is the mass constant. H is the horizontal distance in cm. V is the vertical location in cm. D is the vertical displacement in cm. A is the angle of asymmetry in degrees CM is the coupling multiplier. FM is the frequency multiplier. 1HM is the multiplier for one hand 1HM = 0.60. 2PM is the multiplier for two hands 2PM = 0.85 NM is the multiplier for secondary tasks NM = 0.80 In Step 3; Determine the action required: RI ≤ 0.85 The risk can be considered acceptable 0.85 < RI < 1.0 Significant risk exists.
It is recommended: - use method 3 to reduce the risk - redesigning the machine or procedure - consult with a specialist RI ≥ 1.0 Requires a redesign
| MC [kg] | % H y M | % M | % H | User | ||
|---|---|---|---|---|---|---|
| Professional Use | 10 25 30 40 50 | 95 80 | 90 70 | 99 90 | General Working Population (including young and old) Adult Labor Population Specialized Labour Force | General Working Population Only in Special Cases |
| Datos No Disponibles |
Table 4: Mass constant according to usury group.
| Duration of the Activity | ||||||
|---|---|---|---|---|---|---|
| Frequency [lev/min] | ≤ 8 h | ≤ 2 h | ≤ 1 h | |||
| V<75 | V≥75 | V<75 | V≥75 | V<75 | V≥75 | |
| 0.2 | 0.85 | 0.85 | 0.95 | 0.95 | 1 | 1 |
| 0.5 | 0.81 | 0.81 | 0.92 | 0.92 | 0.97 | 0.97 |
| 1 | 0.75 | 0.75 | 0.88 | 0.88 | 0.94 | 0.94 |
| 2 | 0.65 | 0.65 | 0.84 | 0.84 | 0.91 | 0.91 |
| 3 | 0.55 | 0.55 | 0.79 | 0.79 | 0.88 | 0.88 |
| 4 | 0.45 | 0.45 | 0.72 | 0.72 | 0.84 | 0.84 |
| 5 | 0.35 | 0.35 | 0.6 | 0.6 | 0.8 | 0.8 |
| 6 | 0.27 | 0.27 | 0.5 | 0.5 | 0.75 | 0.75 |
| 7 | 0.22 | 0.22 | 0.42 | 0.42 | 0.7 | 0.7 |
| 8 | 0.18 | 0.18 | 0.35 | 0.35 | 0.6 | 0.6 |
| 9 | 0 | 0.15 | 0.3 | 0.3 | 0.52 | 0.52 |
| 10 | 0 | 0.13 | 0.26 | 0.26 | 0.45 | 0.45 |
| 11 | 0 | 0 | 0 | 0.23 | 0.41 | 0.41 |
| 12 | 0 | 0 | 0 | 0.21 | 0.37 | 0.37 |
| 13 | 0 | 0 | 0 | 0 | 0 | 0.34 |
| 14 | 0 | 0 | 0 | 0 | 0 | 0.31 |
| 15 | 0 | 0 | 0 | 0 | 0 | 0.28 |
| >15 | 0 | 0 | 0 | 0 | 0 | 0 |
Table 5: Multiplier by coupling, according to working cycles per frequency of exposure per min. Source: NIOSH -Psicopreven-2002 [
Results
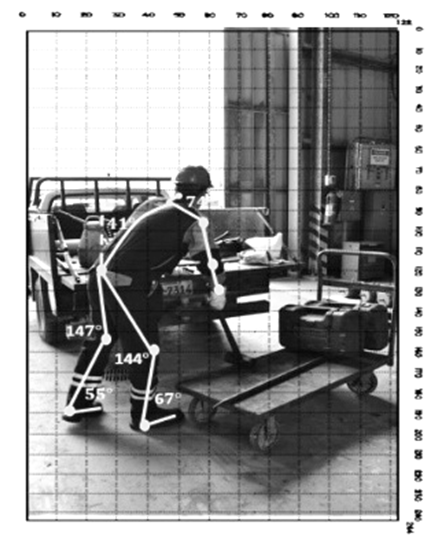
Direct observation (In Situ) by the researchers, based on the results of the study by CN and the UNE-EN 1005-3:2002 method, allowed a real-time analysis by work cycles.
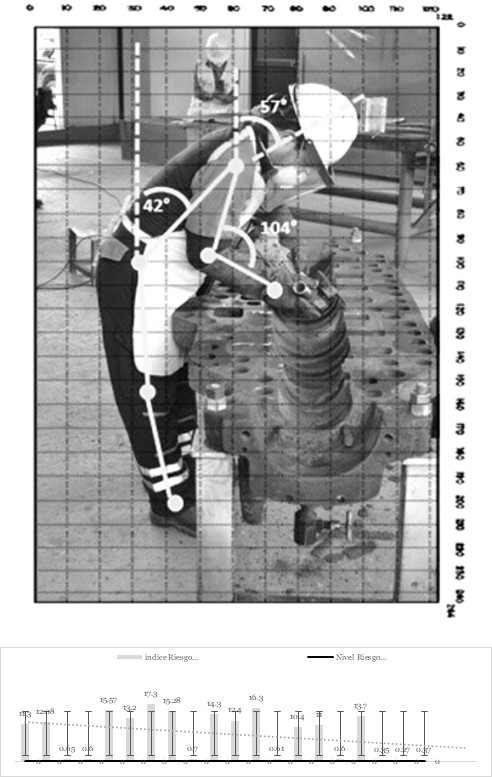
The tasks by activity and absorption by exposure to the risk factor to evaluate, allow to establish results after applying the CN, the information in the labor area, variables like: environmental conditions, design of the work area, tools used, protective equipment, activities carried out by task, time per cycle of activity and risks associated during work (image 3), provide the results of the CN as “The operators have tolerated pain due to MSDs and have received occupational medical care. When the pain has been extreme, it is indicated that 29% of the population has been treated by a general practitioner; 27% have been treated by other specialists, including physiotherapists, neurologists, traumatologists and orthopedists; while 44% have not received medical care. “Operators have received occupational medical care from the organization”, 32% have had X-rays; 10% have had electromyography; and 58% have had other types of examinations such as audiometry, tomography, magnetic resonance imaging, ultrasound, etc. However, in the diagnoses carried out, pathologies such as; tendinitis, rotator cuff inflammation, muscle inflammation, disc herniation, disc bulging, scoliosis, tennis elbow syndrome, rotator cuff ligaments, lumbago, spinal prothrosis and spinal deviation were found in the CCO. Another of the results by the CN is; “The operators received occupational medical care”, 66% stated that they did not follow a treatment and 34% if they received occupational medical treatment with physical therapy, swimming and medication. While in the evaluation by operator and by exposure for the application of the UNE- EN 1005-3:2002 Method, the results provided variables such as:
Risk Level Analysis (RL) by Force
In table 6 and Graph 6, the risk index (ÍR) is evaluated by areas or jobs, based on the results of the method obtained, by force at risk level (NR) and its exposure by cycle (Frequency per min),:
Graph 6: Index of the variable by the IR x NR x Exp.
| Index Risk IR | Risk Level RL | |
|---|---|---|
| Warehouse Technician | 11,3 | High |
| Right-of-way Assistant | 12,08 | High |
| Assistant Welder Api | 0,65 | Not Recommended |
| Inspection and Coating Engineer | 0,6 | Not Recommended |
| Crane Operator | 15,57 | High |
| Welder | 13,2 | Not Recommended |
| Api Welder | 17,3 | High |
| Auxiliary Services Technician | 15,28 | High |
| Electrical Technician | 0,7 | Not Recommended |
| Instrumentation and Control Technician | 14,3 | High |
| Maintenance Technician | 12,4 | High |
| Overhaul Technician | 16,3 | High |
| Cathodic Protection Technician | 0,61 | Not Recommended |
| Piping Technician | 10,4 | High |
| Operator Production | 11 | High |
| Camp Technician | 0,6 | Not Recommended |
| Vacuum Technician | 13,7 | High |
| Community Relations Technician | 0,35 | Acceptable |
| Environment Coordinator | 0,27 | Acceptable |
Table 6: Evaluation of risk level by force.
The force level is based on the application of the variable frequency (min [lev/min]) per work cycle. The compression of the blood vessels which increases the force when the required work is done also increases the muscle mass (Figure 3). On the other hand, the biomechanical and biometric postural maintenance time of the operator defines the static muscular contraction at the moment of keeping an inverse relation with the effort to be demanded.
It has been analyzed that the maximum isometric contraction (static work with force) is maintained during the cycles of 10 sec. per min. [lev/min]; a contraction made at 50% of maximum possible, maintained for one minute. However, when exercising with less than 20% maximum force, it could be obtained for hours. Likewise, the contraction time can be reduced as the force increases due to exposure to it; based on this principle, when evaluating the pathologies associated with the risk found, the MSD is determined. In Table 7 and Graph 7, the NR is analyzed:
| Risk Level (RL) | |
| High Risk | 55% |
| Risk Not Recommended / Level of Attention | 30% |
| Acceptable Risk | 15% |
Table 7: Rating of the NR by exposure.
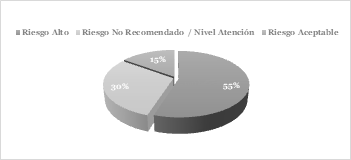
Graph 7: Trend of the NR. by Exp.
In summary, the current scenario of CPF operators, in relation to the risk factor produced by the Force determines that: 55% are exposed to a high risk, while 30% correspond to a not recommended NR and 15% have an acceptable risk. However, it is important to indicate that all positions and work areas are related to field activities and office work. The estimated work stations carry out field work 2/3 of the time per day, although the remaining 1/3 of the time is spent coordinating the preparation of reports on the activities carried out during the day.
Conclusion
In CPFs there are different areas and positions, of which 19 carry out activities that interact integrally, such as handling loads with force, handling heavy tools, forced postures with force and even lifting loads of different weights (kg). Therefore, the existence of force is of greater risk for the appearance of symptoms. By analyzing the level of high risk by force, a health prevention plan is instituted with emphasis on ergonomic occupational medicine, focusing on postural biometrics in each of the operators. However, these collective prevention measures are related to organization, order and cleanliness, corrective and preventive maintenance, programmed in equipment, machines and electric and manual tools. By establishing norms and protocols for the use of force through muscular-osseous movement, it leads to a reduction in personnel morbidity and the cost-benefit ratio in the organization. Training, awareness of pushing and pulling, manual lifting of loads and safe procedures create an ergonomic prevention culture among personnel.
Finally, procedures are issued to carry out relaxation exercises in accordance with the work cycles, as well as specific complementary occupational medical examinations, be they half-yearly or annual, by spinal radiography and carpal tunnel syndrome, for the osteomuscular symptomatological follow-up in the operators of the production plants.
References
-
Muñoz JE (2015) Basic Ergonomics, U. Editorials, Bogotá.
-
Pellecer, M. L. (2015). Ergonomics Manual. Madrid: Pirámide.
-
Llorca PL (2016) Ergonomics Manual. Madrid, Pirámide.
-
Sandoval ST (2009) Risk Assessment Manual for the Prevention of Musculoskeletal Disorders, Barcelona, Spain.
-
Soto AH (2009) Risk Assessment Manual for the Prevention of Musculoskeletal Disorders, Barcelona, Spain.
-
Betancur SM (2014) Newton’s methodology and the demonstration of the reality of the force. Universidad de Antioquia, pp: 131-154.
-
INSHT (2017) Document prepared by the Working Group on MSDs of the CNSST, Madrid, Spain, pp: 22-23.
-
Pickers (2019). www.psyma.com. Retrieved from www. psyma.com
-
Martinez MM (2017) Validation of the Standardized Nordic Musculoskeletal Symptom Questionnaire. Revista de Salud Pública 21: 41-51.
-
Barney VL (2008) Biomechanics of Human Movement, Mexico City, Mexico, pp: 15-16.
-
Veau BL (2008) Biomechanics of the Human Body, Mexico City, Mexico.
-
Pizarro LI (2019) ¿Cómo determinar el tamaño de una muestra? Psyma.
-
Psycho-prevention (2002) UNE-EN 1005-2 STANDARD: 2003. Psicopreven, pp: 1-5.
- The Expanding Landscape of Road Rage: A Systematic Review of Conflicts Involving Drivers, Pedestrians, and Micromobility
- Validating Cognitive Models of Royal Navy Performance on Control Systems
- Comparing Standard and State-of-the-art Firefighter Coats on Postural Balance and Gait in a Live Burn Environment
- Investigating the Integration of Telemedicine into Clinicians Workflow: A Review of Methods
- Risk Assessment of Ergonomic Factors in a Textile Firm by RULA, REBA and Fine Kinney Methods
- Impact of Self-Esteem Training on Individuals with Disabilities Aged 17-30