Case of Splenic Infarction; A Rare Presentation of Complicated Enteric Fever in a Pediatric Patient
Background: The causative organism for enteric fever is Salmonella typhi, which has developed resistance to first-line antibiotics such as ampicillin, chloramphenicol, and TMP-SMX. Case Presentation: A 14-year-old boy presented to the emergency department with complaints of fever, chills, and rigors, as well as excessive sweating and LUQ abdominal pain, for a period of seven days. The boy also experienced vomiting and loose feces for three days. The abdominal examination revealed splenomegaly and LUQ tenderness. Salmonella typhi organism was isolated in blood cultures. Conclusions: Splenic vein thrombosis and infarction, a rare complication of S. Paratyphi infection, frequently cause discomfort in the left upper quadrant. In conjunction with supportive care, third-generation cephalosporins or quinolones are essential for effective treatment.
Background
The causative organism for enteric fever is Salmonella typhi, which has developed resistance to first-line antibiotics such as ampicillin, chloramphenicol, and TMP-SMX. From 2016 to 2018, approximately 5,274 cases of Salmonella Typhi were detected in Sindh, Pakistan. These cases were resistant to first- and second-line antibiotics, including fluoroquinolones and third-generation cephalosporins [1]. The emergence of antibiotic resistance has transformed the enormous threat into a public health emergency, particularly in Pakistan, where enteric fever has become endemic. It was estimated to be responsible for approximately 76.3% of enteric fever cases worldwide, with a higher fatality rate in children and adults from low-income countries [2]. Approximately 10 to 15% of patients with enteric fever experience severe complications, such as gastrointestinal bleeding, pancreatitis, hepatitis, intestinal perforation, DIC, enteric encephalopathy, endocarditis, pneumonia, hemolytic uremic syndrome, and, in rare cases, rhabdomyolysis and reactive hemophagocytic lymphohistocytosis (HLH) [3]. Splenic infarction is a rare complication that is frequently linked to rheumatological and hematological diseases [4, 5]. We present a case of acute peritonitis occurring as a result of splenic infarction, which was a complication of enteric fever.
A 14-year-old boy who was previously healthy and had no significant family history presented to the emergency department with complaints of fever, chills, and rigors, as well as excessive sweating and abdominal pain, for a period of seven days. The boy also experienced vomiting and loose feces for three days. The pain was described as localized to the LUQ, radiating to the back upon coughing, and being acute and stabbing in nature. It occasionally involved the parasternal region. The oral temperature at home was 104◦F. The patient’s immunization record was completed in accordance with the EPI schedule. Upon examination, the child was overweight, with a body mass index (BMI) of 25.4, which was within the 94th percentile for his age and gender. His blood pressure was 110/70, his pulse was 102 bpm, his respiratory rate was 29 breaths per minute, and his oral temperature was recorded as 102F. The abdominal examination was noteworthy for the presence of splenomegaly and LUQ tenderness. The liver span was 10 cm, and the spleen was palpable below the subcostal margin at a depth of 2 cm.
The neutrophil count was predominant in the complete blood count (WBC, 7.4 x 10^9 L; 60% neutrophils). The platelet count was below the normal range at 146 x 10^9/L, and the ESR was elevated at 44 mm/1 hr. PT/INR and APTT were within the normal range, as were renal function tests, Amylase and lipase enzymes, and electrolytes. Salmonella paratyphoid A was resistant to ofloxacin and ciprofloxacin, as evidenced by blood culture. The autoimmune workup was unremarkable. Tables 1a and 1b provide a comprehensive overview of electrolytes, renal function tests, and CBC.
| Hemoglobin | 12.9 gm/dl |
|---|---|
| Red Cell Count | 5.03 x10^12 L |
| H.C.T (PCV) | 38% |
| M.C.V | 76% |
| M.C.H | 27 Pg |
| M.C.H.C | 34 gm/dl |
| R.D.W | 14.40% |
| Total WBC count | 7.4 x 10^9 L |
| Neutrophils | 60% |
| Lymphocytes | 29% |
| Monocytes | 11% |
| Platelet Count | 146 x10^9 L |
| ESR | 44 mm/1 hour |
| Salmonella Paratyphi A Sensitive to Ampicillin, Ceftriaxone, Chloramphenicol, CO- Trimoxazole Resistant to Oflox Cipro | |
| COVID -19 rapid antigen test (ICT) | negative |
RBC morphology: Microcytosis, Normochromic Table 1a: Comprehensive overview of electrolytes, renal function tests, and CBC.
| Renal Function Tests | |
|---|---|
| Urea | 21 mg/dl |
| Creatinine | 0.56 mg/dl |
| Electrolytes | |
| Sodium | 134 meq/L |
| Potassium | 3.9 meq/L |
| Chloride | 96 meq/L |
| Bicarbonate | 26 meq/L |
| Pancreatic Function Tests | |
| Amylase | 49 IU/L range (28-100) |
| Lipase | 44 U/L range 13-60) |
| HBA1c | 6.10% |
Table 1b: Comprehensive overview of electrolytes, renal function tests, and CBC.
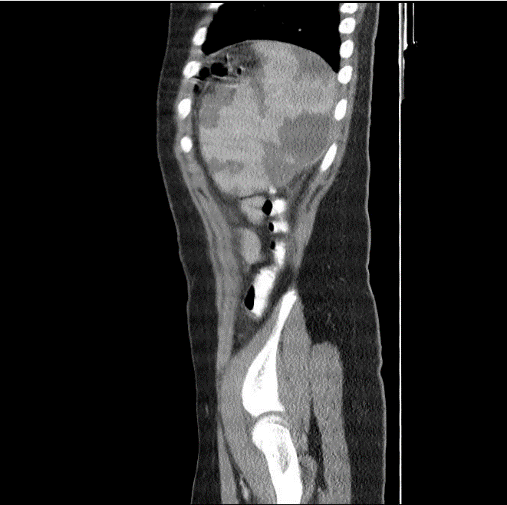
Imaging experiments were conducted. A 13.2 cm spleen was observed to be marginally enlarged during an upper abdominal ultrasound. The largest infarct, which measured 6.2 x 4.0cm and exhibited some liquefaction, was one of numerous splenic infarcts. Afterward, a CT scan of the abdomen was conducted, revealing a marginally enlarged bulky spleen with a craniocaudal extension of 14.0 cm and a width of 8 cm, as well as mild hepatomegaly. The spleen
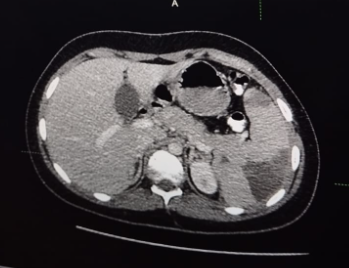
exhibited numerous subcapsular wedge-shaped non- enhancing hypodense areas indicative of splenic infarcts. The largest of these areas was located near the lower pole and measured 5.0 x 3.5 cm. There was no indication of splenic vein thrombosis or splenic artery pseudoaneurysms. A benign reactive mesenteric lymphadenopathy was also observed (Figure 1).
The patient was treated conservatively with antibiotics, supportive care, and nutritional support. In conjunction with Inj. Amikacin and Inj. For metronidazole, we administered 2 g of ceftriaxone intravenously. Intravenous analgesics and antipyretics were administered to alleviate symptoms. Antibiotics were reduced to 400 mg of Inj. Ceftriaxone, Tab. azithromycin, and Tab. metronidazole following the culture report. The patient was discharged after six days of treatment with the same antibiotics and a once-daily PPI. He was advised to undergo an ultrasound of the spleen at the end of the week. The subsequent ultrasound of the spleen revealed a reduction in size from 13.3 × 6.2 cm to 12.5 to 5.7 cm, as well as a re-demonstration of a splenic infarct with an interval reduction in size. The largest infarct, measuring 5.2 x 2.9 cm, exhibited a small liquefied component measuring 2.4 x 1.6 cm. On color Doppler examination, the splenic vein demonstrated normal flow.
The patient demonstrated substantial improvement in signs and symptoms during the follow-up period, despite the fact that he was maintained on a two-week antibiotic course. He remained afebrile and experienced an increase in appetite. Serial ultrasounds were conducted. The final ultrasound conducted after four weeks of illness revealed that the splenic infarcts had resolved, with hyperechoic lesions, the largest of which measured 1.6 × 0.8 cm.
Figure 2 illustrates the subsequent U/S.

Discussion
Myelofibrosis, mural thrombosis following acute myocardial infarction, postpartum toxic syndrome, HIV-
associated mycobacterium, splenic venous thrombosis, trauma, hemoglobinopathy, hemoglobinopathy, systemic embolization, and chronic myelogenous leukemia are among the conditions that can result in splenic infarction [6]. An auto- immune pathology was ruled out in our case due to a routine peripheral smear, negative rheumatoid factor, and negative antinuclear acid antibody. A normal echocardiography ruled out the infarct’s cardiac origin.
Imaging techniques may prove advantageous in the event of splenic involvement in enteric fever. In a previous investigation conducted in Turkey, a patient who was otherwise healthy was documented to have experienced spleen infarction caused by group B Salmonella. His stool samples were positive for group B Salmonellae, and he was seropositive for the O antigen [6]. A patient who was otherwise healthy was the subject of another investigation conducted in France, which described a splenic abscess caused by gram-negative salmonella typhoid. The patient returned to a state of normalcy four months after receiving susceptible antibiotic therapy [7]. Intensive treatment and recovery can result from an earlier ultrasound identification of splenic infarction, as demonstrated by our current case.
The duration of the regimen is contingent upon the presence of complications and extraintestinal symptoms, as antibiotics are the primary treatment for enteric fever. The use of antibiotics such as fluoroquinolones, ampicillin, co-trimoxazole, or third-generation cephalosporins may be adequate for 5-7 days. However, if the infection is severe or drug-resistant, a prolonged course of therapy may be necessary [8]. In cases of ciprofloxacin-resistant enteric fever, many authors also incorporate aminoglycoside antibiotics, such as gentamicin and amikacin, into susceptibility testing to evaluate the in vitro efficacy of these antibiotics and develop a treatment regimen for MDR typhoid fever that is urgently needed [9, 10]. Additionally, there are reports of treatment failures in typhoid fever with ciprofloxacin and 3rd- generation cephalosporins [10]. Amikacin and gentamicin are, therefore, necessary to provide an efficacious treatment regimen. Early detection and, more importantly, the capacity to differentiate between an infarct and an abscess may serve to prevent fatal complications, including splenic hemorrhage and perforation, despite the rarity of the consequences. Furthermore, antibiotic medication may be justified and temporarily reduced.
Nevertheless, the potential mechanisms of solid organ infarction associated with typhoid fever are still not fully understood. Salmonella infections have been associated with thrombosis through the C-type lectin-like receptor-2 on platelets. The bacteria have the potential to colonize solid organs, resulting in inflammatory and thrombotic reactions [11]. Antiplatelet medications are inappropriate in situations that necessitate additional care, such as splenic vein thrombosis and infarction. Nevertheless, there are still no precise indications, which may be due to the rarity of this issue. In the event of large, intricate thrombi and non-resolving conditions, anticoagulation treatment may be implemented. Anticoagulant therapy is typically administered for a period of 3 to 6 months in cases of provoked thrombosis; however, the most critical aspect of treatment is the elimination of the underlying cause. Splenectomy and other surgical procedures are typically reserved for severe cases, such as splenic rupture [12]. Our patient was successfully treated with antibiotics, which prevented the need for a splenectomy.
Conclusion
Splenic vein thrombosis and infarction, a rare complication of S. Paratyphi infection, frequently cause discomfort in the left upper quadrant, which is easily disregarded. Due to the nonspecific nature of laboratory results, prompt diagnosis is essential, particularly through imaging, particularly CT scans. In conjunction with supportive care, third-generation cephalosporins or quinolones are essential for effective treatment. This underscores the significance of early identification and management in guaranteeing the reversibility of the condition.
References
-
Dyson ZA, Klemm EJ, Palmer S, Dougan G (2019) Antibiotic Resistance and Typhoid. Clin Infect Dis 68(2): S165–S170.
-
Shaikh OA, Asghar Z, Aftab RM, Amin S, Shaikh G, et al. (2023) Antimicrobial resistant strains of Salmonella typhi: The role of illicit antibiotics sales, misuse, and self- medication practices in Pakistan. J Infect Public Health 16(10): 1591-1597.
-
Klemm EJ, Shakoor S, Page AJ, Qamar FN, Judge K, et al. (2018) Emergence of an Extensively Drug- Resistant Salmonella enterica Serovar Typhi Clone Harboring a Promiscuous Plasmid Encoding Resistance to Fluoroquinolones and Third-Generation Cephalosporins. mBio 9(1): e00105-e00118.
-
Mehta LK, Arya SC, Mathai G (2007) Infarction of spleen in typhoid fever. Saudi Med J 28(2): 271-272.
-
Rafaey W, Shanawar, Latif A (2020) Splenic Infarction Rare Complication of XDR Enteric Fever; Case Report. Annals of Microbiology and Infectious Diseases 3(2):17- 20.
-
Küpeli S, Alehan D, Akpinar E (2002) Isolated splenic infarction owing to group B Salmonella: case report. Ann Trop Paediatr 22(4): 380-382.
-
Görg C, Bert T (2005) Contrast Enhanced Sonography of Focal Splenic Lesions with a Second-Generation Contrast Agent. Ultraschall Medizin 26(6): 470-477.
-
Yang SE, Jung SH, Kim SH, Kim A, Kim HK, et al. (2012) Typhoid Fever Complicated by Intussusception, Splenic Infarction, and Hepatitis. Journal of The Korean Society of Emergency Medicine 23(3): 439-442.
-
Anand AC, Kataria VK, Singh W, Chatterjee SK (1990) Epidemic multiresistant enteric fever in eastern India. Lancet 335(8685): 352.
-
Mandal S, Mandal MD, Pal NK (2009) In vitro activity of gentamicin and amikacin against Salmonella enterica serovar Typhi: a search for a treatment regimen for typhoid fever. Eastern Mediterranean Health Journal 2(15): 264-268.
-
Hitchcock JR, Cook CN, Bobat S, Ross EA, Flores-Langarica A, et al. (2015) Inflammation drives thrombosis after Salmonella infection via CLEC-2 on platelets. J Clin Invest 125(12): 4429-4446.
-
Saini R, Jesrani G, Gupta M, Gupta S, Chhabra A (2021) Salmonella paratyphi-induced splenic vein thrombosis: A case report on infrequent cause of acute abdomen. Turk J Emerg Med 21(4): 210-213.
- Management of Gallbladder Perforations: A Review
- From The Mouth to the Gut: The Oral Microbiome's Role in Promoting Gastrointestinal Disease
- Case Report: Intraductal Papillary Mucinous Neoplasm (IPMN) Complicated by Portal Vein Plaquing and Biliary Obstruction Mimicking Pancreatic Metastatic Malignancy
- Management of Non-Cirrhotic Portal Hypertension during Pregnancy: A Review
- Effectiveness of Omeprazole versus Pantoprazole for Symptomatic Relief of Gastro-Esophageal Reflux Disease (GERD)/ Acid Peptic Disease (APD): A Real-World Evidence (RWE) Study
- Glimpse of Metabolic-Associated Steatotic Liver Disease [MASLD] in Myanmar