Management of Gallbladder Perforations: A Review
Introduction: Gallbladder perforation (GBP) is a rare but life threatening complication. It has a varied clinical presentation, at times being diagnosed at time of surgery. Hence it poses a challenge to the surgeons. Timely diagnosis and optimal management lead to good outcome. Material and Methods: This study is a prospective analysis of patients presenting with GB perforation form Jan 2021 to December 2024. Traumatic and iatrogenic perforation of GB were excluded from the study. Parameters assessed were clinical presentation, risk factors, comorbidity status, diagnostic investigations, clinical course, management, and outcome. All patients were subjected to CECT scan and USG of the abdomen. They were classified as per Anderson’s modification of original Niemeier’s classification and treated accordingly. Results: 24 patients of GB perforation presented during the study period. 1 patient had Grade I perforation, 15 Grade II and 8 Grade III. In 7 patients (Grade III perforation) diagnosis was made at time of surgery. 23 patients underwent elective surgery with good outcome. 8 patients had wound infection and there was no mortality. Conclusion: Strong clinical suspicion, timely investigation, early intervention with optimization of the patient followed by definitive surgery leads to good outcome.
Introduction
Gallbladder perforation is a life-threatening complication. It is known to occur in 2% of patients with gallbladder diseases and 30% with acute cholecystitis [1]. It has a high risk of morbidity and mortality it being reported in 12-42% cases [2]. Hence it necessitates awareness of the pathology, timely and appropriate management including investigations for an optimal outcome. The present study evaluates our experience of management of GB perforation and reviews the contemporary management as available in literature.
Material and Methods
This is a prospective analytical study of patients with GB perforation presenting to our department over three years from January 2021 to December 2024. Patients with traumatic and iatrogenic GB perforation were excluded from the study. This study was initiated after institutional ethics committee clearance. Parameters assessed were clinical presentation, comorbidity status, diagnostic investigations, clinical course, management, average in-hospital stay and outcome. All patients were subjected to USG of abdomen and CECT Scan of abdomen. Based on imaging, GB perforations were classified as per Anderson’s modification of original Niemeier’s classification and treatment was instituted accordingly. Analysis was done using SPSS software.
Results
Results: A total of 24 (M: F=17: 7) patients of GB perforation presented during the study period. During the same period 289 patients of Acute cholecystitis had presented to us. Their age ranged from 32 to 85 years (mean: 66 years). 8 patients were found to have hypertension and 5 patients’ diabetes. 12 patients presented with acute cholecystitis. One presented with shock. 13 patients had leucocytosis. Liver function test was altered in 7 patients. Ultrasonography of the abdomen identified gall stone disease in all patients. Besides, it revealed Gall Bladder perforation in 8 patients and pericholecystic fluid collection in 13 patients. CECT scan revealed pericholecystic collection in fourteen patient and perforation in 16 patients. 1 patient had Type I perforation, (at fundus). He presented with biliary peritonitis with shock. He was found to have a Giant D2 diverticulum -Lemmels syndrome with dilated CBD (2cm) and choledocholithiasis on CECT Scan. He was optimized by drainage of collection with image guided percutaneous insertion of drain, followed by ERCP with sphincterotomy and stenting. He was thereafter subjected to interval laparoscopic cholecystectomy with choledocho-duodenostomy six weeks hence. There were 15 patients with Type II perforation (7 at fundus) all of whom were diagnosed preoperatively. 12 patients had Tokyo Grade II acute cholecystitis of which 6 had presence of pericholecystic bilious collection with raised WBC count. They were treated with USG guided transhepatic percutaneous cholecystostomy. Percutaneous drainage was also done in 6 patients with collection. Following optimization, they were subjected to interval cholecystectomy after 6 weeks. 2 patients were found to have associated choledocholithiasis. They were subjected to ERCP with sphincterotomy, clearance of CBD and stenting and interval cholecystectomy after 6 weeks. 3 patients were preoperatively suspected to have malignancy along with perforation on imaging, the diagnosis of which was confirmed on image guided biopsy. 2 of these patients were subjected to extended cholecystectomy with administration of adjuvant chemotherapy. They are on regular follow up 17 &12 months post -surgery. 1 patient was detected to have distant metastasis. He was started on chemotherapy with palliative intent and died 3.5 months later. All the 12 patients with Type II perforation presenting with acute cholecystitis were subjected to laparoscopic cholecystectomy, however in 3 patients (25%) there was need for conversion to open, with one patient being subjected to laparoscopic subtotal cholecystectomy. 2 patients of malignancy were subjected to open extended cholecystectomy. There were 8 patients with Type III perforation (5 at fundus). However, 7 of these were detected to have perforation at the time of surgery. Only in one patient, CECT Scan revealed perforation preoperatively. In the other 7 CECT Scan showed dense adhesions suggestive of acute on chronic cholecystitis. 5 patients underwent laparoscopic cholecystectomy with stapled resection of duodenal sleeve. The other three patients, underwent laparoscopic cholecystectomy converted to open, with cholecystectomy and segmental transverse colectomy. The histopathology of all the three patients was xantho- granulomatous cholecystitis.
Discussion
Gall Bladder perforation is an uncommon complication with incidence rate of 2% in patients with gallbladder diseases and 30% with acute cholecystitis [1]. In the present study the incidence was 8.3% of GB diseases, which compares with the available literature evidence [1, 3]. It is a paradox that GB perforation commonly occurs in patients with acute cholecystitis a pathology commonly seen in females, but GB perforation is predominantly seen in males. This fact has been corroborated by various studies, with male predominance seen in present study too (70.83%) [3, 4, 5]. The most common implicated site of GB perforation is its fundus, it being most prone to ischemia [3, 6]. In the present study 54.16% (13 patients) were found to have perforation located at the fundus. Factors like gallstones diabetes mellitus, prolonged use of steroid, malignancy, cirrhosis, immunosuppressive state, atherosclerosis and hypertension are known risk factors for GB perforation [1, 2, 3, 7, 8, 9, 10]. In the present study 33.33% (8 patients) had hypertension, 20.8 % (5 patients) diabetes and 12.5 % (3 patients) had Ca Gall Bladder.
GB perforation is classified as per Andersons Modification of original Neimeiers classification into four types as shown in Table I [11, 12]. GB perforation commonly occurs as a sequalae of GB obstruction which leads to increased intraluminal cholecystic pressure, ischaemia, necrosis leading to perforation [13]. This may lead to either generalised biliary peritonitis (type-1 perforation or localised biliary peritonitis (type- II perforation). Occasionally the perforation site may form a fistulous tract and communicate with either adjacent structures (type-III perforation) or with biliary tree (type IV perforation). The distribution of type of perforations in patients in the present study is as shown in Table I. Type II perforation is commonly encountered. The finding of 62.5 % (15 patients) having Type II perforation in the present study is in accordance with other studies in the literature [14, 15, 16].
| Description | Nos of Patients | |
|---|---|---|
| TYPE I | Acute free perforation, where the perforation is into the peritoneal cavity without any protective adhesions | 1 |
| TYPE II | Sub-acute perforation, where the perforation is walled off by adhesions from the peritoneal cavity with a surrounding abscess | 15 |
| TYPE III | Chronic perforation, where there is fistulous communication between the gallbladder and the bowel | 8 |
| TYPE IV | Chronic perforation, where there is fistulous communication between the gallbladder and the biliary tree | 0 |
Table 1: Distribution of Patients with Gall Bladder Perforation as Per Anderson’s modification of original Niemeier’s classificat
The clinical features of GB perforation are vague and not specific. They usually present with pain in right upper quadrant pain, fever, and jaundice [2]. The summary of the presenting clinical features of patients in our study is given in Table II. Presence of fever, tachycardia with leucocytosis, altered liver function test raises the suspicion of perforation. Patients with free perforation (Type I) may have a rapid clinical deterioration and present in septic shock as our one patient of Type I did. Laboratory investigations including Leucocytosis (seen in 13 patients in the present study), alteration in LFT (seen in 7 patients in the present study) do not confirm the diagnosis, though they help in corroborating the clinical suspicion [7]. In this context appropriate imaging plays a pivotal role in confirming the diagnosis and in guiding the treatment. Plain X ray abdomen does not contribute much in diagnosis except for in Type III perforation wherein serial X-rays may reveal change in the position of gall stones within the intestinal lumen (Tumbling sign) causing transient Intestinal Obstruction [3, 17].
| Acute Cholecystitis | Xantho-Granulomatous Cholecystitis | Choledocholithiasis | GB Cancer | Lemmels Syndrome | |
|---|---|---|---|---|---|
| TYPE 1 | 1 | ||||
| TYPE II | 12 | 2 | 3 | ||
| TYPE III | 5 | 3 | 1 | 1 |
Table 2: Clinical Presentation of Patients with Gall Bladder Perforation.
Ultrasonography of the abdomen remains not only the first investigation but also the most common and preferred investigation to be performed for detecting gall bladder perforation. In the present study too, it was performed in all patients. However, the reported rate of detection of GB perforation is only 70%, with inability to visualize the site of perforation in some cases [18, 19]. The most specific USG findings suggestive of Gall Bladder perforation is the “Sonographic Hole Sign” [20]. The other findings suggestive of GB perforation are detection of gallstones outside of the gall bladder, intraperitoneal free fluid in patients (Type I perforation), Gangrenous cholecystitis with micro abscess and haemorrhage within GB wall along with collection adjacent to GB and bulging and layering of the gallbladder wall, and rarely hepatic abscess in case of perforation of the medial wall of gall bladder within the hepatic parenchyma [3,21-
23]. In the present study only in 33.33% (8 patients) could USG detect GB Perforation; however, it did reveal presence of pericholecystic fluid in 54.16% (13 patients) raising the suspicion of GB perforation. CECT Scan is the investigation of choice to confirm the diagnosis of GB perforation, owing to its high accuracy rate [24]. Its sensitivity is 69.2%, compared to 38.5% of USG of the abdomen [19]. Findings suggestive of perforation on CECT scan includes presence of defect in the wall of GB, extraluminal gall stones, pericholecystic or intraperitoneal free fluid and presence of gas within GB wall [24, 25, 26]. Besides these, extra GB findings such as inflammation of the duodenum and hepatic flexure of the colon also confirms the clinical suspicion of GB perforation. In our study CECT scan had confirmed the diagnosis of GB perforation in 66.66% (16 patients), malignancy in 12.5% (3 patients) and dense adhesions in 29.1% (7 patients).
Type I perforation (Acute free perforation) calls for an emergent surgical intervention the access being either laparoscopic or open depending on the expertise available. It is associated with a high conversion rate from laparoscopic to open with the reported incidence being as high as 75% [27]. Besides when the critical view of safety cannot be achieved, a subtotal cholecystectomy is recommended ensuring prevention of iatrogenic bile duct injury [28]. There is an emerging consensus to treat these patients, if possible, initially with image guided insertion of percutaneous drainage to drain the collection, optimizing the patient and then subject the patients to cholecystectomy after 3 -4 weeks [29]. This approach, especially in patients with co- morbidities and or associated pathology leads to improved outcome and decrease in mortality [30]. In our study too, we had one patient with type I perforation with Lemmels syndrome (Giant D2 diverticulum) with dilated CBD and choledocholithiasis. He was initially subjected to drainage of collection with image guided percutaneous insertion of drain, followed by ERCP with sphincterotomy and stenting. He was thereafter subjected to interval laparoscopic cholecystectomy and choledocho-duodenostomy.
The optimal management of Type II gallbladder perforation has yet to be defined. The treatment options include image guided percutaneous catheter drainage of the gallbladder followed by interval cholecystectomy; emergency cholecystectomy with local lavage; and at times only percutaneous catheter drainage of the gallbladder and abscess with antibiotics. Study by Chang -Wei Ke and Shuo-Dong Wu has shown that compared to emergency cholecystectomy, percutaneous catheter drainage of the gallbladder followed by interval cholecystectomy was associated with lower rate of need to convert to open cholecystectomy, lower intraoperative bleeding, shorter duration of postoperative abdominal drainage, shorter hospital stays after cholecystectomy, fewer admissions to the ICU and decreased post operative morbidity [31]. Abusedera et al have shown that only percutaneous catheter drainage is a safe and effective option when treating patients with localized disease, particularly in elderly with co-morbidities and who are not good surgical candidates [32]. They found that 70% of these patients did not have recurrent cholecystitis and did not require any further interventions after interval removal of the catheter. In our study 9 patients of Tokyo Grade II acute cholecystitis with perforation were treated with USG guided transhepatic percutaneous cholecystostomy and interval cholecystectomy. 6 of these patients had peri GB collection which was also drained percutaneously. 2 patients had associated CBD calculi for which they were subjected to ERCP Sphincterotomy with CBD clearance and stenting.
Gall bladder carcinoma presenting with perforation is rare. Perforation in these patients could be attributed to impairment of the blood supply induced by intramural thrombosis [33]. Oohashi et al have reported spontaneous gallbladder perforation in two patients of adeno-squamous carcinoma of gall bladder [34]. In our study there were three patients who on CECT Scan had features suggested of malignancy which was confirmed on biopsy done preoperatively. One of the patients had distant metastasis and wad treated with chemotherapy with palliative intent. The other 2 patients had contained perforation within the liver and Grade 1 ECOG status. They were subjected to open extended cholecystectomy and administered adjuvant chemotherapy. Both the patients are doing well and are on regular follow up 17 &12 months post -surgery. Performing laparoscopic cholecystectomy and obtaining a critical view of Calot’s safety triangle may be difficult in patients with Type II perforation presenting with acute cholecystitis. In such a situation conversion to open cholecystectomy or performing a subtotal cholecystectomy is recommended [35]. In our study 12 patients with Type II perforation presenting with acute cholecystitis were subjected to laparoscopic cholecystectomy, however in 3 patients (25%) there was need for conversion to open, with one patient being subjected to laparoscopic subtotal cholecystectomy. The reason to convert to open was inability to obtain Critical View of safety owing to adhesions.
Type III GB perforation is observed commonly in patients with chronic cholecystitis [36]. If detected preoperatively, one can plan the surgery well. However, because of the chronic inflammation induced fibrosis, preoperative diagnosis of perforation is difficult [37]. Most of the Type III GB perforation are diagnosed intraoperatively [38]. In our study too, of the 8 patients with Type III, 7 were diagnosed intra-operatively. The postulated pathogenesis of cholecysto- enteric fistula is an obstructing stone in the gallbladder neck or cystic duct causing ischemic necrosis and perforation of the gallbladder, forming a walled-off abscess. This abscess perforates in the adjacent bowel lumen leading to fistulous communication. As a result, apart from cholecystectomy, these patients often require additional surgical procedures to repair the fistula [39, 40]. Duodenum due to its proximity is the most common site of cholecysto-enteric fistula [41]. In our study 5 patients of 8 (62.5%) had cholecysto-duodenal fistula. They underwent laparoscopic cholecystectomy with stapled resection of duodenal sleeve. The other three patients, had fistulous communication with transverse colon. They underwent laparoscopic cholecystectomy converted to open, with cholecystectomy and segmental transverse colectomy. All the three patients were diagnosed to have xantho-granulomatous cholecystitis on histopathology. The summary of treatment given to our patients is given in Table III. There was no mortality in our study. However, morbidity in form of wound infection was seen in 33.33.% (8) patients- 1 with Grade I perforation, 5 in Grade II and 2 in Grade III
perforation. They were treated with antibiotics as per the sensitivity culture report. The average in hospital stay of all these patients’ post-surgery was 7 days with patients of Grade III perforation having extended stay for more than 5 days owing to the suture line on the bowel.
| Type I (n=1) | Type II (n=5) | Type III (n=8) | |
|---|---|---|---|
| Interval lap chole (+/- dismantling of fistula) | 5 | 5 | |
| Interval lap converted to OC (+/- dismantling of fistula) | 3 | 2 | |
| Bail out- Lap subtotal chole | 1 | ||
| Interval OC (+/- dismantling of fistula) | 3 | 1 | |
| Extended cholecystectomy | 2 | ||
| Choledochoduodenostomy | 1 |
Table 3: Treatment of Gall Bladder Perforation.
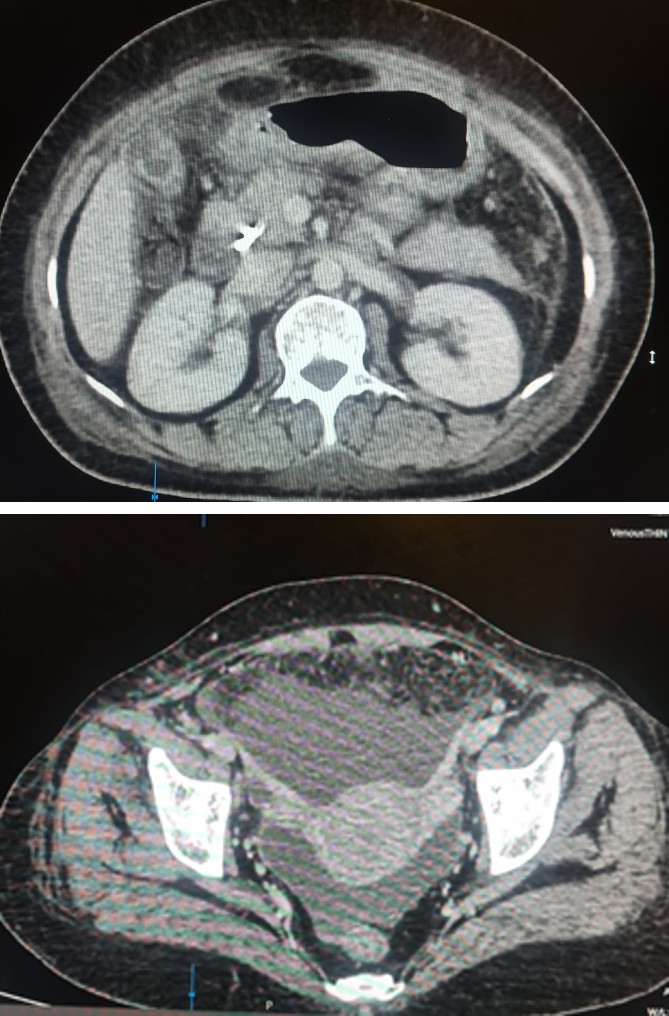
CECT Scan A: Grade I Perforatio.
CECT Scan B: Pelvic Collection.
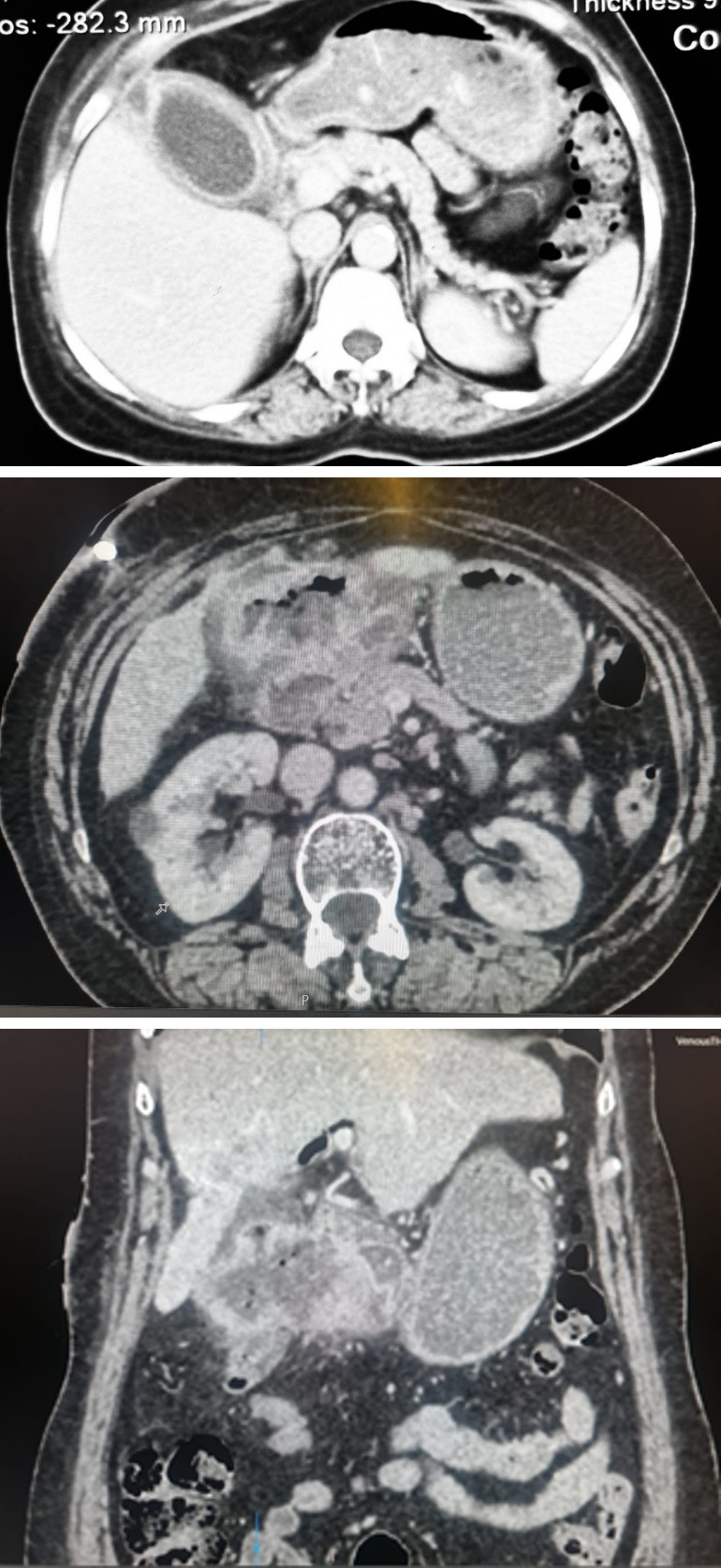
CECT Scan: Grade II Perforation.
CECT Scan: Grade III Perforation.
Conclusion
Spontaneous, non-iatrogenic perforation of gall Bladder perforation is not uncommon. A timely CECT Scan helps in confirming a strong clinical suspicion of GB perforation. Image guided placement of percutaneous pigtail catheter and ERCP if necessary, helps to optimize the patient before subjecting the patient to definitive surgery with good post operative outcome.
Conflicts of Interest
The authors declare no conflict of interest.
References
-
Ausania F, Guzman SS, Alvarez GH, del Rio PS, Nuñez EC (2015) Gallbladder perforation: morbidity, mortality, and preoperative risk prediction. Surg Endosc 29(4): 955-960.
-
Date RS, Thrumurthy SG, Whiteside S, Umer MA, Pursnani KG, et al. (2012) Gallbladder perforation: case series and systematic review. Int J Surg 10(2): 63-68.
-
Derici H, Kara C, Bozdag AD, Nazli O, Tansug T, et al. (2006) Diagnosis and treatment of gallbladder perforation. World J Gastroenterol 12(48): 7832-7836.
-
Roslyn JJ, Thompson JE, Darvin H, DenBesten L (1987) Risk factors for gallbladder perforation. Am J Gastroenterol 82(7): 636-640.
-
Bedirli A, Sakrak O, Sözüer EM, Kerek M, Güler I (2001) Factors effecting the complications in the natural history of acute cholecystitis. Hepato-gastroenterology 48: 1275-1278.
-
Isch JH, Finneran JC, Nahrwold DL (1971) Perforation of the gallbladder. Am J Gastroenterol 55(5): 451-458.
-
Albisher HM, Foula MS, Alghusnah ES, Abdelhafiz T (2023) Risk factors and outcomes in acute perforated gallbladder: A retrospective cohort study. Asian J Surg 46(6): 2299-2303.
-
Lo HC, Wang YC, Su LT, Hsieh CH (2012) Can early laparoscopic cholecystectomy be the optimal management of cholecystitis with gallbladder perforation? A single institute experience of 74 cases. Surg Endosc 26(11): 3301-3306.
-
Sayed L, Sangal S, Finch G (2010) Spontaneous cholecysto-cutaneous fistula: a rare presentation of gallstones. J Surg Case Rep 5(5): 5.
-
Stefanidis D, Sirinek KR, Bingener J (2006) Gallbladder perforation: risk factors and outcome. J Surg Res 131(2): 204-208.
-
Anderson BB, Nazem A (1987) Perforations of the gallbladder and cholecystobiliary fistulae: a review of management and a new classification. J Natl Med Assoc 79(4): 393-399.
-
Niemeier OW (1934) Acute free perforation of the gallbladder. Ann Surg 99(6): 922-924.
-
Cruz RJ, Nahas J, de Figueiredo LFP (2006) Spontaneous cholecystocutaneous fistula: a rare complication of gallbladder disease. Sao Paulo Med J 124: 234-236.
-
Williams NF, Scobie TK (1976) Perforation of the gall bladder: analy sis of 19 cases. Can Med Assoc J 115: 1223-1224.
-
Isch J, Finnerman JC, Nahrwold DL (1971) Perforation of gall bladder in acute cholecystitis. Am J Gastroenterol 55: 550-551.
-
Menakuru SR, Aman LK, Behera A, Singh R, Katariya RN (2004) Current Management of Gall Bladder Perforations. ANZ J Surg 74: 843-846.
-
Theodorou D, Theodorou SJ, Gkogkos V, Ziogas D (2024) The “Tumbling Gallstone Sign” of obstructive Gallstone Ileus”. Journal of Gastrointestinal and Liver Disease: JGLD 33(2): 158-158.
-
Sood BP, Kalra N, Gupta S, Sidhu R, Gulati M, et al. (2002) Role of Sonography in diagnosis of gallbladder perforation. J Clin Ultrasound 30: 270-274.
-
Kim PN, Lee KS, Kim IY, Bae WK, Lee BH (1994) Gallbladder perforation: comparison of US findings with CT. Abdom Imaging 19(24): 239-242.
-
Shapira-Rootman M, Mahamid A, Reindorp N, Nachtigal A, Zein A (2015) Diagnosis of GB perforation by Ultrasound. Clin Imaging 39(5): 827.
-
Seyal AR, Parekh K, Gonzalez-Guindalini FD, Nikolaidis P, Miller FH, et al. (2014) Cross sectional imaging of perforated Gall Bladder. Abdom imaging 39(4): 853-874.
-
Revzin MV, Scoutt L, Smitaman E, Israel GM (2015) The Gall Bladder: Uncommon GB conditions and unusual presentations of the common GB pathological processes. Abdom Imaging 40(2): 385-399.
-
Lardiere-Deguelte S, Ragot E, Amroun K, Piardi T, Dokmak S, et al. (2015) Hepatic Abscess: Diagnosis and management. J Visc Surg 152(4): 231-243.
-
Tsai M-J, Chen J-D, Tiu C-M, Chou Y-H, Hu S-C, et al. (2009) Can Acute cholecystits with GB perforation be detected preoperatively by Computed Tomograoghy in ED? Correlation with clinical data and computed tomography features. Am J Emerg Med 27(5): 574-581.
-
Boruah DK, Sanyal S, Sharma BK, Boruah DR (2016) Comparative evaluation of Ultrasonography and cross-sectional imaging in determining gall bladder perforation in accordance to Niemeiers classification. J Clin Diagn Res 10(8): TC15-TC18.
-
Morris BS, Balpande PR, Morani AC, Chaudhary RK, Maheshwari M, et al. (2007) The CT appearances of GB perforation. Br J Radiol 80(959): 898-901.
-
Stefanidis D, Sirinek KR, Bingener J (2006) Gallbladder perforation: risk factors and outcome. J Surg Res 131(2): 204-208.
-
Kristo G (2024) An overview of the management of gallbladder perforations. Glob J Surg Case Rep.
-
Abusedera MA, Khaliel M, Hassan AEMA (2017) Surgical and non-surgical treatment of non-traumatic gallbladder perforation. The Egyptian Journal of Radiology and Nuclear Medicine 48: 43-49.
-
Huang CC, Lo HC, Tzeng YM, Huang HH, Chen JD, et al. (2007) Percutaneous transhepatic gall bladder drainage: a better initial therapeutic choice for patients with gall bladder perforation in the emergency department. Emerg Med J 24(12): 836-840.
-
Ke C-W, Wu S-D (2018) Comparison of Emergency Cholecystectomy with Delayed Cholecystectomy After Percutaneous Transhepatic Gallbladder Drainage in Patients with Moderate Acute Cholecystitis. J Laparoendosc Adv Surg Tech A 28(6): 705-712.
-
Abusedera MA, Khaliel M, Hassan AEMA (2017) Surgical and non-surgical treatment of non-traumatic gallbladder perforation. The Egyptian Journal of Radiology and Nuclear Medicine 48(1): 43-49.
-
Namikawa T, Kobayashi M, Okabayashi T, Okamoto K, Akimori T, et al. (2007) Clinicopathological analysis of idiopathic perforation of the gallbladder. Surg Today 37: 633-637.
-
Oohashi Y, Shirai Y, Wakai T, Nagakura S, Watanabe H, et al. (2002) Adenosquamous carcinoma of the gallbladder warrants resection only if curative resection is feasible. Cancer 94: 3000-3005.
-
Okamoto K, Suzuki K, Takada T, Strasberg SM, Asbun HJ, et al. (2018) Tokyo Guidelines 2018: flowchart for the management of acute cholecystitis. J Hepatobiliary Pancreatic Sci 25(1): 55-72.
-
Quiroga-Garza A, Alvarez-Villalobos NA, Angeles-Mar HJ, Garcia-Campa M, Muñoz-Leija MA, et al. (2021) Localized gallbladder perforation: a systematic review of treatment and prognosis. HPB 23: 1639-1646.
-
Rikki S, Amit M, Samita G, Bir S, Parul J (2011) Management of gall bladder perforation evaluation on Ultrasonography: report of six rare cases with review of literature. J Med Life 4(4): 364-371.
-
Gunasekaran G, Naik D, Gupta A, Bhandari V, Kuppusamy M, et al. (2015) Gallbladder perforation: a single center experience of 32 cases. Korean J Hepatobiliary Pancreat Surg 19(1): 6-10.
-
Doko M, Zovak M, Kopljar M, Glavan E, Ljubicic N, et al. (2003) Comparison of surgical treatments of gallstone ileus: preliminary report. World J Surg 27: 400-404.
-
_Doherty GM, Way LW (2003) Biliary Tract. In: Way_ _LW, Doherty GM (Eds.), Current Surgical Diagnosis &_ _Treatment. (11__th_ _Edn.), McGraw-Hill, New York, pp. 595-_ _624._
-
Nuño-Guzmán CM, Marín-Contreras ME, Figueroa- Sánchez M, Corona JL (2016) Gallstone ileus, clinical presentation, diagnostic and treatment approach. World J Gastrointest Surg 8(1): 65-76.
- From The Mouth to the Gut: The Oral Microbiome's Role in Promoting Gastrointestinal Disease
- Case Report: Intraductal Papillary Mucinous Neoplasm (IPMN) Complicated by Portal Vein Plaquing and Biliary Obstruction Mimicking Pancreatic Metastatic Malignancy
- Management of Non-Cirrhotic Portal Hypertension during Pregnancy: A Review
- Effectiveness of Omeprazole versus Pantoprazole for Symptomatic Relief of Gastro-Esophageal Reflux Disease (GERD)/ Acid Peptic Disease (APD): A Real-World Evidence (RWE) Study
- Case of Splenic Infarction; A Rare Presentation of Complicated Enteric Fever in a Pediatric Patient
- Glimpse of Metabolic-Associated Steatotic Liver Disease [MASLD] in Myanmar