Effectiveness of Omeprazole versus Pantoprazole for Symptomatic Relief of Gastro-Esophageal Reflux Disease (GERD)/ Acid Peptic Disease (APD): A Real-World Evidence (RWE) Study
Objective: To compare the effectiveness of omeprazole versus pantoprazole for satisfactory resolution of GERD/APD symptoms. Design: This multicentric, real-world evidence (RWE) study was conducted using data extracted from electronic medical records (EMRs) of anonymized, treatment-naïve, adult GERD/APD patients treated with proton pump inhibitors (PPIs) omeprazole or pantoprazole. The primary endpoint was the proportion of patients achieving satisfactory symptom resolution with 20mg/day omeprazole versus 40mg/day pantoprazole after 14(±7) and 28(±7) days. Secondary endpoints included lifestyle-based patient profile, proportion of patients achieving satisfactory symptom resolution with 40mg/day omeprazole versus 80mg/day pantoprazole after 14(±7) and 28(±7) days, response of patients with comorbidities or regular smoking/ drinking habits, and safety/tolerability of treatment. Results: Data from 300 EMRs for each PPI was analyzed. A higher proportion of patients achieved complete symptom resolution with omeprazole(20mg) than pantoprazole(40mg); the difference was statistically significant for heartburn (21.65% versus 4.85%, p<0.001), regurgitation (33.51% versus 22.47%, p=0.011), and epigastric pain (31.44% versus 16.74%, p<0.001) among others, at 14(±7) days, and for heartburn (p<0.001) and epigastric pain (p<0.001) at 28(±7) days. Omeprazole(40mg) was significantly more effective than pantoprazole(80mg) for complete resolution of bloating at 14(±7) days and of regurgitation and bloating at 28(±7) days. In patients with hypertension, diabetes, or cardiac conditions, omeprazole resulted in better symptom resolution than pantoprazole. In patients with obesity or regular smoking/drinking habits, the PPIs were comparably effective. No adverse events were reported. Conclusion: Omeprazole(20mg) was safe and well-tolerated in patients and was significantly more effective than pantoprazole(40mg) in resolving GERD/APD symptoms at 14(±7) and 28(±7) days.
Introduction
Acid Peptic Disease (APD) collectively refers to medical conditions such as gastro-esophageal reflux disease (GERD), gastritis, gastric ulcer, duodenal ulcer, esophageal ulcer, Zollinger Ellison Syndrome (ZES), and Meckel’s diverticular ulcer [1]. GERD is a multifactorial, often chronic disease caused by a conglomeration of intrinsic and structural mechanisms, causing disruption of esophagogastric junction barrier leading to retrograde flow of acidic gastric contents into the esophagus [2]. In 2020, the global pooled prevalence of GERD ranged from 2.5% to 45.4%, depending on the region [3]. The prevalence of GERD in the Indian population ranged from 5% to 28.5%, as reported in 2021 [4]. Risk factors of the indication can be related to lifestyle, food habits, sleeping habits, and usage of certain medications [5].
The most predominant symptoms of GERD are heartburn and regurgitation. However, atypical and extra-esophageal symptoms are not uncommon; these include, but are not restricted to, hoarseness, throat irritation, epigastric pain, bloating, nausea, and sleep disturbance [5, 6]. The primary goals of GERD treatment are symptom relief, prevention of symptom relapse, healing of erosive esophagitis, and prevention of complications. Treatment options include lifestyle and dietary modifications, pharmacotherapy, and surgery. Pharmacotherapy is directed at neutralization of gastric acid or suppression of its secretion. The latter includes the use of proton pump inhibitors (PPIs), antacids, mucosal protective agents, alginates, histamine 2 receptor antagonists (H2RAs), prokinetics, transient lower esophageal sphincter relaxation (TLESR) reducers, and pain modulators, either singly or in combination [2, 7, 8, 9].
PPIs, the standard of care for GERD/APD, irreversibly bind to and inhibit the hydrogen/potassium ATPase [H+/ K+ ATPase] pump on the parietal cells of the stomach, thus decreasing gastric acid secretion [10]. International guidelines recommend the use of PPIs in addition to other management strategies [11, 12, 13, 14]. PPIs include omeprazole, esomeprazole, pantoprazole, lansoprazole, rabeprazole, and dexlansoprazole [15]. Omeprazole was the first substituted benzimidazole approved by the Food and Drug Administration (FDA) for inhibition of gastric acid secretion and its use is widespread till date owing to the rapid onset of its inhibitory effects and its proven effectiveness [16, 17, 18, 19, 20].
As reported in a recent review on global PPI usage, there are at least 28 million PPI users in 23 countries. Nearly a quarter of the adult population use PPIs and almost two- thirds of PPI users were on greater than or equal to defined daily dose (DDD) of PPIs [15]. An upward trend was observed in PPI prescriptions, with pantoprazole and omeprazole being the top two most-prescribed drugs [21]. There is, however, a dearth of documented data on common clinical practices and outcomes of PPI usage, as rightly pointed out in a recent systematic review by Shanika et al. [15]. Evaluation of PPI effectiveness in Indian patients is important given that epidemiological studies have consistently shown a high prevalence of metabolic syndrome in India (as much as one- quarter of the adult population is thought to be affected and might be on medications for systemic diseases) which makes it crucial to understand whether PPIs are effective in patients with comorbidities [22]. Another important question is whether GERD/APD patients who smoke and/or drink alcohol regularly would benefit from PPI consumption. This real-world evidence (RWE) study was conducted to assess if there is a difference in the current effectiveness of omeprazole versus pantoprazole despite both of them being PPIs with similar mechanism of action. The study also aimed to evaluate the effectiveness of these PPIs amongst the subgroups of adult patients described above. This study also sheds light on the safety and tolerability of these PPIs and informs on lifestyle- related attributes (such as eating, sleeping, exercising habits, etc.) of GERD/APD patients in India.
Methods
This multicentric RWE study was conducted using electronic medical records (EMRs) of 600 patients who were prescribed omeprazole or pantoprazole between March and September 2023 for management of GERD/ APD. The data was collected from 19 physicians located in geographically diverse regions of India. The study was conducted in accordance with the principles of Declaration of Helsinki, Indian Council for Medical Research (ICMR), and Indian Good Clinical Practice (GCP) Guidelines for clinical trials on pharmaceutical products in India, as mentioned in New Drugs and Clinical Trials (NDCT) rules 2019, issued by the Central Drugs Standard Control Organization (CDSCO), Ministry of Health, Government of India. Data collection was initiated only after approval from an independent ethics committee (IEC) was obtained in writing. Since this study involved extracting aggregate data from EMRs and analyzing it in an anonymized manner, informed consent form (ICF) from patients was not required. Therefore, permission for ICF waiver was obtained from IEC in line with ICMR guidelines 2017 before initiation of data collection. Anonymity of patients was maintained throughout the study. Identity parameters of patients, if any, were removed at source while extracting data from EMRs. The patients were identified throughout and after the completion of the study by system-generated unique IDs. The trial was registered with the Clinical Trials Registry of India (CTRI) on March 29, 2023 (reference number: CTRI/2023/03/051166).
Data from adult patients aged ≥18 years was included in the study only once the data satisfied all the following criteria: data showed that patients were treatment naïve (defined as patients who did not receive any anti-acidity or anti-ulcer agent since two weeks prior to commencement of PPI administration under study assessment), duration of treatment with either omeprazole or pantoprazole was at least 4 weeks, and patient information was available in EMRs. Patients on treatment with H2RAs or antacids or combinatorial treatment with PPIs and prokinetics or antacids within two weeks prior to PPI administration, those with ongoing PPI treatment, and those having refractory GERD already treated with PPI for 6-12 weeks were excluded from the study. Patients refractory to PPI treatment and those who were advised against use of PPIs at the discretion of the physician were also excluded. Any other condition that, in opinion of the physician, did not justify use of patient-related information in the study, was also a criterion for exclusion.
A sample size of 578 patients was computed to observe a difference of 9% between the effectiveness of omeprazole versus pantoprazole in achieving symptomatic relief of GERD/APD symptoms (acid eructation, heartburn, and pain on swallowing were considered as main symptoms in the reference used) with 80% power and 5% level of significance [23]. The number of patients was approximated to 600 to account for EMRs with missing or incomplete information.
Data extracted from EMRs included baseline characteristics of patients (age, sex, height, weight, comorbidities, smoking/drinking habits), lifestyle-related information (like eating, sleeping, and exercising habits, etc.), current diagnosis, and severity of GERD/APD symptoms (heartburn, regurgitation, epigastric pain, nausea, vomiting, bloating) before treatment (baseline) and after 14 (±7) and 28 (±7) days from treatment initiation. Severity of each symptom was graded as none or no symptom (score=0), mild (score=1), moderate (score=2), severe (score=3), or very severe (score=4). Additionally, information regarding the impact of GERD/APD treatment on presence or absence of hoarseness/sore throat, sleep disturbance, eating disturbance, productive daily activities, social life, and professional life was also retrieved from the EMRs.
The primary endpoint was the proportion of patients achieving satisfactory resolution of symptoms when treated with omeprazole (20mg) versus pantoprazole (40mg) for 14 (±7) and 28 (±7) days as assessed by the treating physician. The secondary endpoints included patient profile (with respect to daily life activities such as meal, sleep, smoking, and drinking habits, etc.), proportion of patients achieving satisfactory resolution of symptoms when treated with omeprazole (40mg) versus pantoprazole (80mg) for 14 (±7) and 28 (±7) days as assessed by the treating physician, response of patients with comorbid conditions and on regular medications for systemic diseases to treatment with omeprazole versus pantoprazole, response of patients with regular smoking/drinking habits to omeprazole versus pantoprazole, and safety and tolerability of the PPIs.
In addition to the planned endpoints of the study, analysis was performed to evaluate the change in symptom severity score upon treatment with omeprazole (20mg) versus pantoprazole (40mg) and to assess the effect of GERD/APD treatment with omeprazole versus pantoprazole on daily life activities/symptoms (hoarseness/sore throat, sleep disturbance, eating disturbance, productive daily activities, social life, and professional life) based on information available in the retrieved data.
All data analysis was based on the International Council for Harmonization (ICH) E9 document ‘Statistical Principles for Clinical Trials’ and were carried out as per comprehensive statistical analysis plan using SPSS version 28.0.1.1 (IBM Corp., Armonk, NY, USA). The null hypothesis was that there is no difference in effectiveness between omeprazole and pantoprazole while the alternate hypothesis was that there is a difference in effectiveness. All hypothesis testing was carried out at the 5% (2-sided) significance level. Statistical significance was evaluated based on p-value, where, *: p<0.05, : p<0.01, and *: p<0.001. Independent t-test was used to compare age, weight, and height between the two groups at baseline. Categorical variables were reported as number (percentage). The denominator for each percentage was the total number of patients in a treatment group, unless otherwise mentioned. Chi-square test was used for comparison of proportion of patients between the groups. Repeated measures ANOVA with post hoc (Bonferroni correction) analysis was used for evaluation of symptom severity scores. Association of lifestyles with severity and treatment-induced resolution of symptoms was checked using Pearson correlation.
Results
Among 600 adult treatment-naïve GERD/APD patients, 300 each were treated with omeprazole and pantoprazole (Figure 1). The mean ± standard deviation (SD) age was 46.12 ± 14.73 years in omeprazole and 46.81 ± 14.71 years in pantoprazole. The mean weight and height among patients in the two groups were comparable. Overall, there was a similar distribution of patients with no statistically significant differences between the groups with respect to demographic characteristics assessed at baseline. Overall, most patients were diagnosed with APD (61.67%) while some were diagnosed with GERD (36.83%) and a few with both APD and GERD (1.5%). At baseline, the distribution between the groups was comparable for all GERD/APD symptoms. The proportion of patients in each group having comorbid conditions (hypertension, type 2 diabetes mellitus, cardiac conditions, obesity) was also comparable, hypertension being the most common comorbidity (33.83% overall). The proportion of patients with regular smoking/drinking habits was comparable between the groups (Table 1).
- Omeprazole (N=300)
- Pantoprazole (N=300) p-value
- Age (in years)
- Mean ± SD
- 46.12 ± 14.73
- 46.81 ± 14.71
- 0.562
- Median (min, max)
- 45 (18, 80)
- 45 (18, 95)
- Age-group, n (%)
- 18 - 30 years
- 50 (16.67%)
- 38 (12.67%)
- 31 - 40 years
- 71 (23.67%)
- 71 (23.67%)
- 41 - 50 years
- 72 (24.00%)
- 85 (28.33%)
- 51 - 65 years
- 78 (26.00%)
- 70 (23.33%)
- >65 years
- 29 (9.67%)
- 36 (12.00%)
- Weight (in kg)
- Mean ± SD
- 68.66 ± 9.34
- 68.22 ± 9.66
- 0.573
- Median (min, max)
- 69 (40, 89)
- 68 (38, 93)
- Height (in cm)
- Mean ± SD
- 164.13 ± 7.22
- 164.69 ± 7.65
- 0.357
- Median (min, max)
- 165 (147, 184)
- 165 (145, 185)
- Sex, n (%)
- Male
- 164 (54.67%)
- 158 (52.67%)
- 0.624
- Female
- 136 (45.33%)
- 142 (47.33%)
- Diagnosis, n (%)
- APD
- 184 (61.33%)
- 186 (62.00%)
- 0.865
- GERD
- 111 (37.00%)
- 110 (36.67%)
- 0.936
- APD, GERD
- 5 (1.67%)
- 4 (1.33%)
- 0.727
- GERD/APD symptom, n (%)
- Heartburn
- 286 (95.33%)
- 275 (91.67%)
- 0.068
- Regurgitation
- 249 (83.00%)
- 263 (87.67%)
- 0.105
- Epigastric pain
- 280 (93.33%)
- 289 (96.33%)
- 0.096
- Nausea
- 229 (76.33%)
- 240 (80.00%)
- 0.275
- Vomiting
- 184 (61.33%)
- 197 (65.67%)
- 0.271
- Bloating
- 258 (86.00%)
- 250 (83.33%)
- 0.362
- Comorbidity, n (%)
- Hypertension
- 100 (33.33%)
- 103 (34.33%)
- 0.794
- Type 2 diabetes mellitus
- 84 (28.00%)
- 76 (25.33%)
- 0.459
- Cardiac conditions
- 36 (12.00%)
- 44 (14.67%)
- 0.337
- Obesity
- 11 (3.67%)
- 13 (4.34%)
- 0.674
- Regular smoking/drinking habits, n (%)
- Smoking
- 30/300 (10.00%)
- 30/300 (10.00%)
- 0.999
- Drinking
- 33/300 (11.00%)
- 35/300 (11.67%)
- 0.794
Table 1: Baseline characteristics of patients.
Table 1: Baseline characteristics of patients. Abbreviations: APD = Acid Peptic Disease; cm = centimeter; GERD = Gastro-Esophageal Reflux Disease; kg = kilogram Statistical tests used:
- Independent t-test to compare age, weight, and height between the two groups
- Chi-square test to compare distribution of male and female patients, GERD symptoms, comorbidities, and regular smoking/ drinking habits between the two groups Note:
- n (%) is the proportion of patients, as mentioned; ‘N’ is the total number of patients in each group.
- Each patient presented with ≥1 GERD symptom at baseline Among the EMRs analyzed for omeprazole, 194/300 (64.67%) were for omeprazole (20mg), and among the ones analyzed for pantoprazole, 227/300 (75.67%) were for pantoprazole (40mg) (Figure 1). Based on cumulative percentage of patients with symptom resolution at each data accrual point, a significantly higher proportion of patients treated with omeprazole (20mg) achieved complete resolution of heartburn (21.65% versus 4.85%, p<0.001), regurgitation (33.51% versus 22.47%, p=0.011), epigastric pain (31.44% versus 16.74%, p<0.001), nausea (50.00% versus 39.21%, p=0.026), and bloating (51.03% versus 39.21%, p=0.015) at 14 (±7) days compared to those treated with pantoprazole (40mg); the proportion of patients with complete resolution of vomiting was numerically higher in omeprazole (20mg) than pantoprazole (40mg) (53.09% versus 48.90%, p=0.389). At 28 (±7) days, the statistical significance of omeprazole (20mg) over pantoprazole (40mg) persisted for complete resolution of heartburn (75.77% versus 56.83%, p<0.001) and epigastric pain (81.96% versus 63.88%, p<0.001), while complete resolution of regurgitation, nausea, vomiting, and bloating was observed in numerically higher proportion of patients in omeprazole (20mg) compared to pantoprazole (40mg) (Figure 2). The proportion of patients with complete resolution of all baseline symptoms at 28 (±7) days was significantly higher upon treatment with omeprazole (20mg) than that with pantoprazole (40mg) (65.46% versus 33.48%, p<0.001).
Electronic medical records (EMRs) of 600 GERD/APD patients was retrieved: 300 treated with omeprazole and 300 with pantoprazole. In the omeprazole group, 194 patients were treated with 20mg/day and 106 with 40mg/day. In the pantoprazole group, 227 patients were treated with 40mg/day and 73 with 80mg/day. All patient data till 28 days (window period: ±7 days) of treatment was used for analysis.
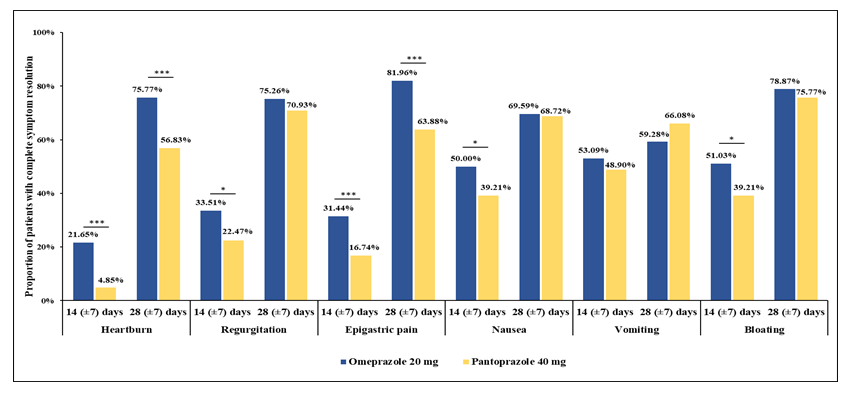
Figure 2: Complete resolution of GERD symptoms: omeprazole (20mg) versus pantoprazole (40mg). Statistical test used: Chi-square test *: p<0.05; ***: p<0.001 Note: Total number of patients: omeprazole (20mg), 194; pantoprazole (40mg), 227. A significantly higher proportion of patients treated with omeprazole (20mg), compared to pantoprazole (40mg), achieved complete resolution of heartburn, regurgitation, epigastric pain, nausea, and bloating at 14 (±7) days. At 28 (±7) days, the proportion of patients with complete resolution of heartburn and epigastric pain was significantly higher when treated with omeprazole (20mg) compared to pantoprazole (40mg).
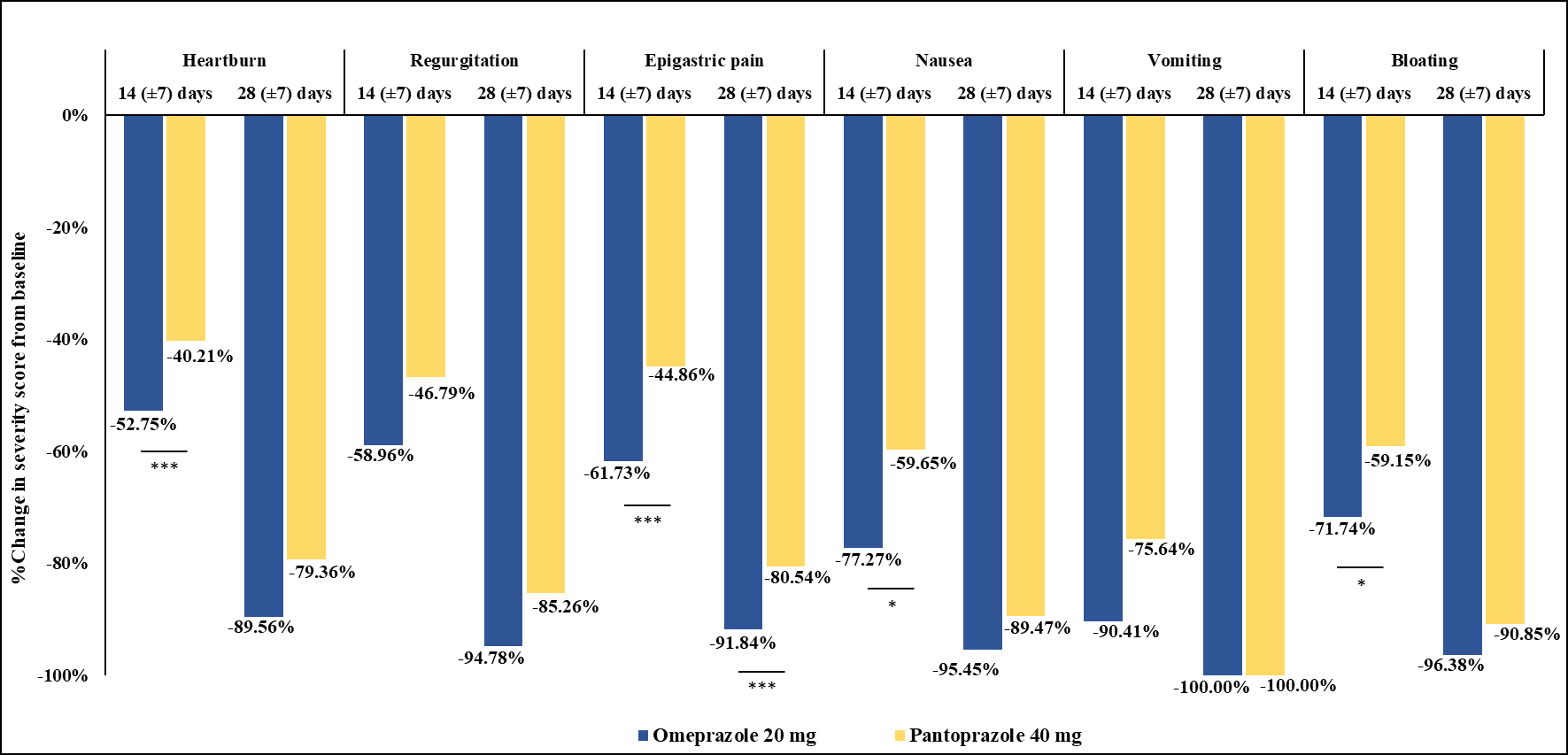
Supplementary Figure 1: Percentage of change in symptom severity score: omeprazole (20mg) versus pantoprazole (40mg). Statistical test used: Repeated Measures ANOVA with post hoc (Bonferroni correction) *: p<0.05; *: p<0.001 Note:** Total number of patients: omeprazole (20mg), 194; pantoprazole (40mg), 227.
Patients in both groups showed significant decrease in severity scores of all individual symptoms as well as in mean total symptom severity score at both 14 (±7) and 28 (±7) days (p<0.001 in all cases; data not shown). At 14 (±7) days, the percentages of decrease in severity scores of heartburn, epigastric pain, nausea, and bloating were significantly higher and that of regurgitation and vomiting were numerically higher in patients treated with omeprazole (20mg) compared to pantoprazole (40mg). A higher percentage of decrease in severity scores of heartburn, regurgitation, epigastric pain, nausea, and bloating in omeprazole (20mg) compared to pantoprazole (40mg) was observed at 28 (±7)
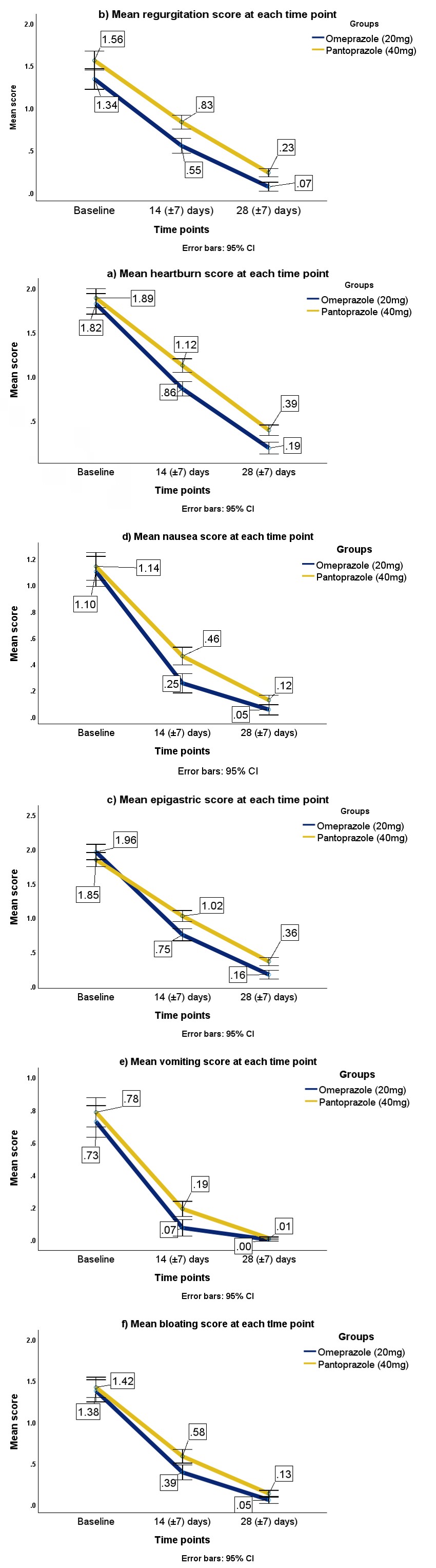
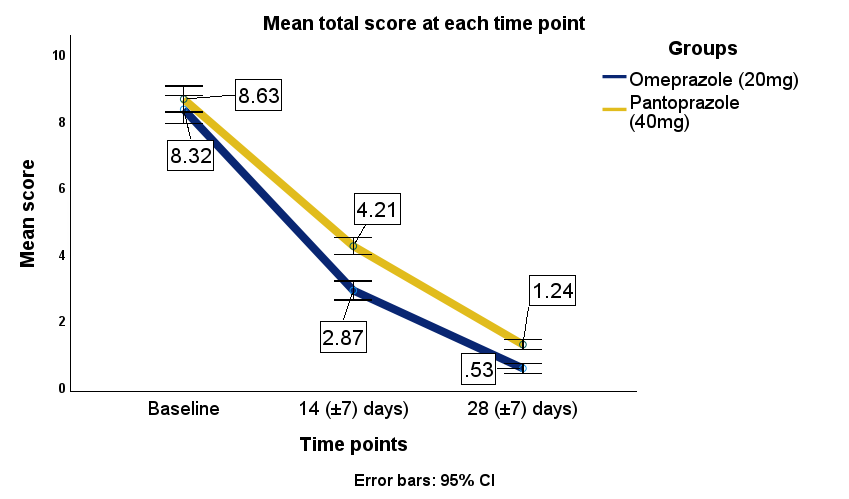
days as well, although statistical significance between the groups was attained only for epigastric pain (Supplementary Figure 1). The percentage of decrease in mean total symptom severity score in omeprazole compared to pantoprazole was significantly higher at 14 (±7) days (65.50% versus 51.22%, p<0.001) and numerically higher at 28 (±7) days (omeprazole, 93.63%; pantoprazole, 85.63%, p=0.177). Repeated measures ANOVA models for the decrease in mean severity scores of each symptom and in mean total symptom severity score are presented in Figure 3 and Figure 4, respectively.
Comparison between patients administered higher doses of the study medications showed that a significantly higher proportion of patients treated with omeprazole (40mg), compared to pantoprazole (80mg), achieved complete resolution of bloating at 14 (±7) days (57.55% versus 39.73%, p=0.019) and that this significant difference between the groups was sustained at 28 (±7) days (83.02% versus 64.38%, p=0.004). Additionally, the proportion of patients who achieved complete resolution of regurgitation was significantly higher among patients treated with omeprazole (40mg) compared to pantoprazole (80mg) at 28 (±7) days (80.19% versus 65.75%, p=0.030). Results of other analyses were comparable between the groups (Supplementary Figure 2).
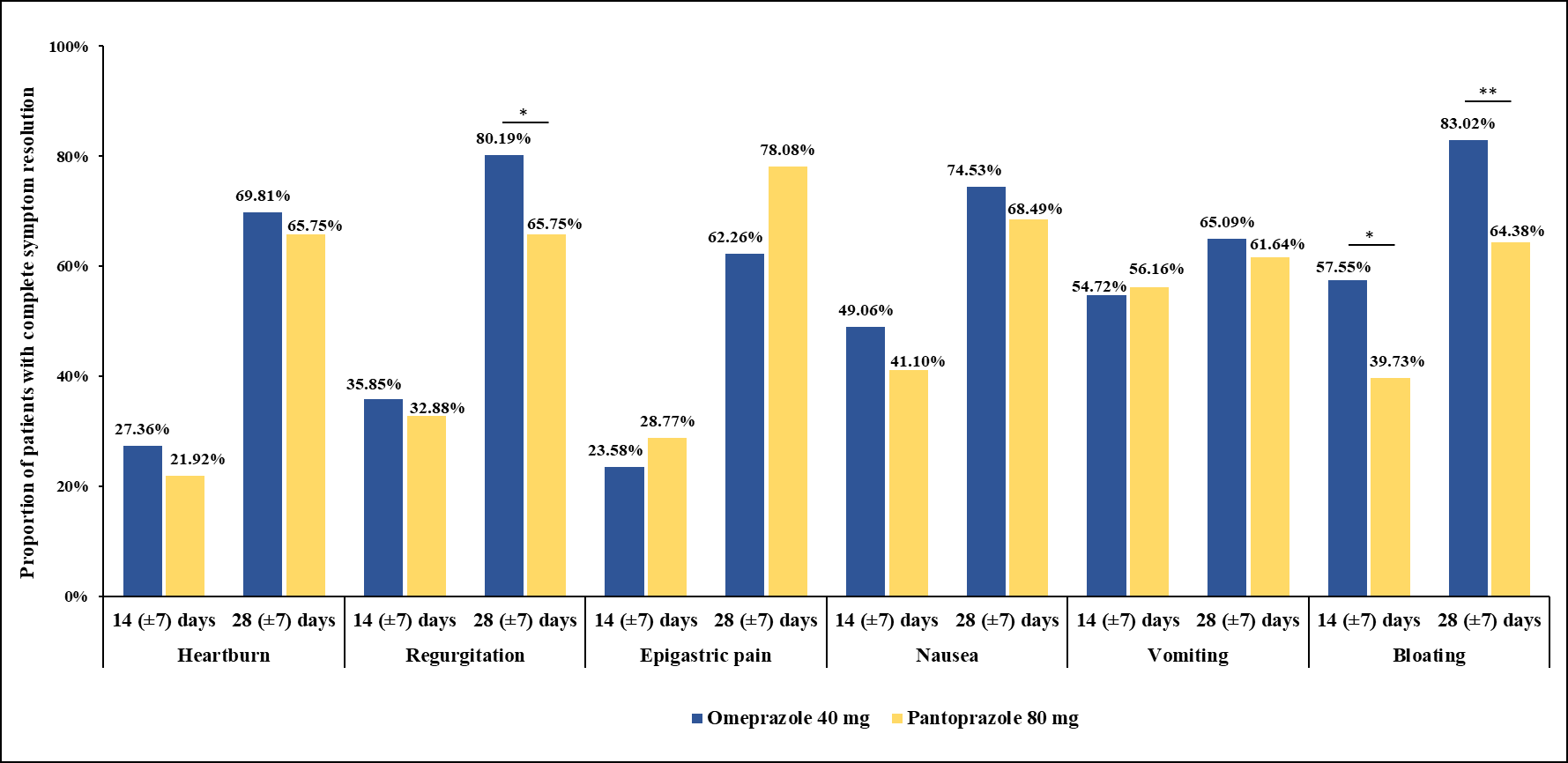
Supplementary Figure 2: Complete resolution of GERD symptoms: omeprazole (40mg) versus pantoprazole (80mg). Statistical test used: Chi-square test *: p<0.05; : p<0.01 Note:** Total number of patients: Omeprazole (40mg), 103; Pantoprazole (80mg),73.
Among the 600 total patients analyzed in this study, 33.83% had hypertension, 26.67% had type 2 diabetes mellitus, 13.33% had cardiac conditions, 4.00% had obesity, 10.00% had regular smoking habits, and 11.33% had regular drinking habits. Results showed that both omeprazole (20mg or 40mg) and pantoprazole (40mg or 80mg) were comparably effective in symptomatic relief of GERD/APD in these subgroups of patients, except a few instances wherein absence of certain symptoms was achieved by a significantly higher proportion of patients treated with omeprazole (20mg or 40mg) compared to pantoprazole (40mg or 80mg) in these subgroups; these endpoints are mentioned here. A progressive increase in the proportion of patients displaying absence of symptoms implies that patients achieved symptom resolution with time. Among hypertensive patients, a significantly higher proportion of patients treated with omeprazole, compared to pantoprazole, showed absence of heartburn at 14 (±7) days (19.00% versus 5.83%, p=0.004) and regurgitation (93.00% versus 83.50%, p=0.035) and nausea (97.00% versus 86.41%, p=0.006) at 28 (±7) days. Among diabetic patients, a significantly higher proportion of patients treated with omeprazole, compared to pantoprazole, showed absence of heartburn at 14 (±7) days (22.62% versus 9.21%, p=0.021) and regurgitation (94.05% versus 80.26%, p=0.008) and bloating (95.24% versus 84.21%, p=0.020) at 28 (±7) days. Among patients with cardiac conditions, a significantly higher proportion of patients treated with omeprazole, compared to pantoprazole, showed absence of nausea at 28 (±7) days (97.22% versus 81.82%, p=0.030) (Supplementary table 1). Effectiveness of omeprazole and pantoprazole was comparable in patients with regular smoking/drinking habits (Supplementary table 2). There were no adverse events reported upon treatment with either omeprazole or pantoprazole, both for low and high doses.
| Absence of GERD symptoms at: | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Baseline | Day 14 (±7 days) | Day 28 (±7 days) | |||||||||
| Hypertension | |||||||||||
| Omeprazole | Pantoprazole | p-value | Omeprazole | Pantoprazole | p-value | Omeprazole | Pantoprazole | p-value | |||
| (n=100) | (n=103) | (n=100) | (n=103) | (n=100) | (n=103) | ||||||
| Heartburn, n (%) | 3 (3.00%) | 2 (1.94%) | 0.624 | 19 (19.00%) | 6 (5.83%) | 0.004** | 71 (71.00%) | 66 (64.08%) | 0.293 | ||
| Regurgitation, n (%) | 12 (12.00%) | 6 (5.83%) | 0.121 | 45 (45.00%) | 38 (36.89%) | 0.242 | 93 (93.00%) | 86 (83.50%) | 0.035* | ||
| Epigastric pain, n (%) | 12 (12.00%) | 3 (2.91%) | 0.013* | 25 (25.00%) | 22 (21.36%) | 0.541 | 75 (75.00%) | 71 (68.93%) | 0.337 | ||
| Nausea, n (%) | 19 (19.00%) | 24 (23.30%) | 0.453 | 73 (73.00%) | 67 (65.05%) | 0.222 | 97 (97.00%) | 89 (86.41%) | 0.006** | ||
| Vomiting, n (%) | 39 (39.00%) | 43 (41.75%) | 0.689 | 92 (92.00%) | 93 (90.29%) | 0.667 | 100 (100.00%) | 103 (100.00%) | 0.999 | ||
| Bloating, n (%) | 9 (9.00%) | 12 (11.65%) | 0.535 | 60 (60.00%) | 56 (54.37%) | 0.417 | 94 (94.00%) | 97 (94.17%) | 0.96 | ||
| Diabetes mellitus | |||||||||||
| Omeprazole | Pantoprazole | p-value | Omeprazole | Pantoprazole | p-value | Omeprazole | Pantoprazole | p-value | |||
| (n=84) | (n=76) | (n=84) | (n=76) | (n=84) | (n=76) | ||||||
| Heartburn, n (%) | 1 (1.19%) | 3 (3.95%) | 0.262 | 19 (22.62%) | 7 (9.21%) | 0.021* | 63 (75.00%) | 49 (64.47%) | 0.147 | ||
| Regurgitation, n (%) | 7 (8.33%) | 5 (6.58%) | 0.674 | 37 (44.05%) | 26 (34.21%) | 0.204 | 79 (94.05%) | 61 (80.26%) | 0.008** | ||
| Epigastric pain, n (%) | 7 (8.33%) | 4 (5.26%) | 0.441 | 26 (30.95%) | 16 (21.05%) | 0.155 | 64 (76.19%) | 51 (67.11%) | 0.2 | ||
| Nausea, n (%) | 18 (21.43%) | 17 (22.37%) | 0.888 | 54 (64.29%) | 50 (65.79%) | 0.841 | 80 (95.24%) | 67 (88.16%) | 0.101 | ||
| Vomiting, n (%) | 34 (40.48%) | 30 (39.47%) | 0.896 | 78 (92.86%) | 65 (85.53%) | 0.133 | 84 (100.00%) | 75 (98.68%) | 0.293 |
Table 2: Impact of GERD treatment in patients with regular smoking/drinking habits: Omeprazole (20mg or 40mg) versus Pantopraz
| Bloating, n (%) | 8 (9.52%) | 11 (14.47%) | 0.332 | 50 (59.52%) | 37 (48.68%) | 0.17 | 80 (95.24%) | 64 (84.21%) | 0.020* |
|---|---|---|---|---|---|---|---|---|---|
| Cardiac conditions | |||||||||
| Omeprazole | Pantoprazole | p-value | Omeprazole | Pantoprazole | p-value | Omeprazole | Pantoprazole | p-value | |
| (n=36) | (n=44) | (n=36) | (n=44) | (n=36) | (n=44) | ||||
| Heartburn, n (%) | 0 (0%) | 1 (2.27%) | 0.362 | 3 (8.33%) | 2 (4.55%) | 0.483 | 20 (55.56%) | 21 (47.73%) | 0.483 |
| Regurgitation, n (%) | 5 (13.89%) | 5 (11.36%) | 0.727 | 13 (36.11%) | 14 (31.82%) | 0.689 | 34 (94.44%) | 35 (79.55%) | 0.053 |
| Epigastric pain, n (%) | 4 (11.11%) | 1 (2.27%) | 0.105 | 7 (19.44%) | 5 (11.36%) | 0.312 | 23 (63.89%) | 22 (50.00%) | 0.211 |
| Nausea, n (%) | 2 (5.56%) | 8 (18.18%) | 0.089 | 24 (66.67%) | 26 (59.09%) | 0.483 | 35 (97.22%) | 36 (81.82%) | 0.030* |
| Vomiting, n (%) | 10 (27.78%) | 12 (27.27%) | 0.96 | 31 (86.11%) | 37 (84.09%) | 0.802 | 36 (100.00%) | 44 (100.00%) | 0.999 |
| Bloating, n (%) | 5 (13.89%) | 7 (15.91%) | 0.802 | 25 (69.44%) | 25 (56.82%) | 0.246 | 35 (97.22%) | 42 (95.45%) | 0.681 |
| Obesity | |||||||||
| Omeprazole | Pantoprazole | p-value | Omeprazole | Pantoprazole | p-value | Omeprazole | Pantoprazole | p-value | |
| (n=11) | (n=13) | (n=11) | (n=13) | (n=11) | (n=13) | ||||
| Heartburn, n (%) | 0 (0%) | 0 (0%) | 0.999 | 4 (36.36%) | 2 (15.38%) | 0.238 | 9 (81.82%) | 10 (76.92%) | 0.771 |
| Regurgitation, n (%) | 1 (9.09%) | 2 (15.38%) | 0.645 | 3 (27.27%) | 6 (46.15%) | 0.342 | 10 (90.91%) | 11 (84.62%) | 0.645 |
| Epigastric pain, n (%) | 2 (18.18%) | 2 (15.38%) | 0.857 | 4 (36.36%) | 5 (38.46%) | 0.912 | 9 (81.82%) | 11 (84.62%) | 0.857 |
| Nausea, n (%) | 2 (18.18%) | 4 (30.77%) | 0.477 | 9 (81.82%) | 11 (84.62%) | 0.857 | 11 (100.00%) | 12 (92.31%) | 0.347 |
| Vomiting, n (%) | 2 (18.18%) | 7 (53.85%) | 0.071 | 11 (100.00%) | 13 (100.00%) | 0.999 | 11 (100.00%) | 13 (100.00%) | 0.999 |
| Bloating, n (%) | 2 (18.18%) | 0 (0%) | 0.107 | 5 (45.45%) | 4 (30.77%) | 0.459 | 10 (90.91%) | 12 (92.31%) | 0.904 |
Table 3: Impact of GERD treatment in patients with regular smoking/drinking habits: Omeprazole (20mg or 40mg) versus Pantopraz
Supplementary Table 1: Impact of GERD treatment in patients with comorbidities: Omeprazole (20mg or 40mg) versus Pantoprazole (40mg or 80mg). Statistical test used: Chi-square test; *: p<0.05; : p<0.01 Note:** n’ is the number of patients with no symptom; ‘N’ is the total number of patients in each group.
| Absence of GERD symptoms at: | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Baseline | Day 14 (±7 days) | Day 28 (±7 days) | ||||||||
| Regular smoking habits | ||||||||||
| Omeprazole | Pantoprazole | p-value | Omeprazole | Pantoprazole | p-value | Omeprazole | Pantoprazole | p-value | ||
| (n=30) | (n=30) | (n=30) | (n=30) | (n=30) | (n=30) | |||||
| Heartburn, n (%) | 1 (3.33%) | 1 (3.33%) | 0.999 | 3 (10.00%) | 3 (10.00%) | 0.999 | 22 (73.33%) | 18 (60.00%) | 0.271 | |
| Regurg itation, n (%) | 3 (10.00%) | 2 (6.67%) | 0.638 | 15 (50.00%) | 10 (33.33%) | 0.19 | 29 (96.67%) | 26 (86.67%) | 0.161 | |
| Epigastric pain, n (%) | 1 (3.33%) | 2 (6.67%) | 0.552 | 4 (13.33%) | 7 (23.33%) | 0.317 | 22 (73.33%) | 20 (66.67%) | 0.575 | |
| Nausea, n (%) | 4 (13.33%) | 5 (16.67%) | 0.718 | 19 (63.33%) | 16 (53.33%) | 0.429 | 28 (93.33%) | 23 (76.67%) | 0.07 | |
| Vomiting, n (%) | 4 (13.33%) | 12 (40.00%) | 0.019* | 29 (96.67%) | 27 (90.00%) | 0.298 | 30 (100.00%) | 30 (100.00%) | 0.999 | |
| Bloating, n (%) | 1 (3.33%) | 1 (3.33%) | 0.999 | 17 (56.67%) | 14 (46.67%) | 0.435 | 28 (93.33%) | 26 (86.67%) | 0.389 | |
| Regular drinking habits | ||||||||||
| Omeprazole | Pantoprazole | p-value | Omeprazole | Pantoprazole | p-value | Omeprazole | Pantoprazole | p-value | ||
| (n=33) | (n=35) | (n=33) | (n=35) | (n=33) | (n=35) | |||||
| Heartburn, n (%) | 1 (3.03%) | 1 (2.86%) | 0.968 | 6 (18.18%) | 3 (8.57%) | 0.242 | 28 (84.85%) | 25 (71.43%) | 0.183 | |
| Regurgi tation, n (%) | 2 (6.06%) | 2 (5.71%) | 0.952 | 16 (48.48%) | 9 (25.71%) | 0.051 | 30 (90.91%) | 28 (80.00%) | 0.204 | |
| Epigastric pain, n (%) | 2 (6.06%) | 2 (5.71%) | 0.952 | 13 (39.39%) | 11 (31.43%) | 0.49 | 28 (84.85%) | 29 (82.86%) | 0.825 | |
| Nausea, n (%) | 8 (24.24%) | 6 (17.14%) | 0.471 | 17 (51.52%) | 14 (40.00%) | 0.342 | 30 (90.91%) | 27 (77.14%) | 0.123 | |
| Vomiting, n (%) | 13 (39.39%) | 16 (45.71%) | 0.596 | 30 (90.91%) | 28 (80.00%) | 0.204 | 33 (100.00%) | 35 (100.00%) | 0.999 | |
| Bloating, n (%) | 2 (6.06%) | 5 (14.29%) | 0.262 | 20 (60.61%) | 16 (45.71%) | 0.218 | 32 (96.97%) | 30 (85.71%) | 0.101 |
Table 4: Impact of GERD treatment in patients with regular smoking/drinking habits: Omeprazole (20mg or 40mg) versus Pantopraz
Supplementary Table 2: Impact of GERD treatment in patients with regular smoking/drinking habits: Omeprazole (20mg or 40mg) versus Pantoprazole (40mg or 80mg). Statistical test used: Chi-square test; *: p<0.05 Note: n’ is the number of patients with no symptom; ‘N’ is the total number of patients in each group.
Information on lifestyle at baseline revealed that 58.5% patients did not have meals at around the same timing every day, 57.5% did not have a gap of 1-2 hrs between dinner and bedtime, 61.67% did not have a light dinner, 60.17% did not get uninterrupted sleep for 6-8 hrs daily, 68.67% suffered from personal/work-related stress, 44.17% patients had long/ late working hours, and most prominently, 88.17% patients did not practice regular physical exercise. However, Pearson correlation coefficient did not show a significant association between maintaining same meal timings daily, having a gap of 1-2 hrs between dinner and bedtime, personal/work-related stress, long/late working hours, or lack of regular physical exercise with severity of heartburn or regurgitation or their resolution post treatment (data not shown). The proportion of patients who showed absence of the impact of GERD/APD on sleep disturbance, eating disturbance, productive daily activities, social life, and professional life upon treatment with omeprazole (20mg or 40mg) was comparable to the corresponding proportion with pantoprazole (40mg or 80mg) at both 14 (±7) and 28 (±7) days. The proportion of patients with absence of hoarseness/sore throat at 14 (±7) days was significantly higher in omeprazole compared to pantoprazole (Supplementary Table 3).
| Absence at: | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Baseline | Day 14 (±7 days) | Day 28 (±7 days) | |||||||
| Omeprazole | Pantoprazole | p-value | Omeprazole | Pantoprazole | p-value | Omeprazole | Pantoprazole | p-value | |
| (N=300) | (N=300) | (N=300) | (N=300) | (N=300) | (N=300) | ||||
| Hoarseness/ sore throat, n (%) | 194 (64.67%) | 194 (64.67%) | 0.999 | 297 (99.00%) | 289 (96.33%) | 0.030* | 299 (99.67%) | 298 (99.33%) | 0.561 |
| Sleep disturbance, n (%) | 125 (41.67%) | 124 (41.33%) | 0.936 | 283 (94.33%) | 276 (92.00%) | 0.258 | 297 (99%) | 295 (98.33%) | 0.477 |
| Eating disturbance, n (%) | 133 (44.33%) | 129 (43.00%) | 0.741 | 282 (94%) | 284 (94.67%) | 0.726 | 297 (99%) | 300 (100.00%) | 0.081 |
| Productive daily activities impacted, n (%) | 167 (55.67%) | 160 (53.33%) | 0.568 | 296 (98.67%) | 293 (97.67%) | 0.362 | 298 (99.33%) | 299 (99.67%) | 0.561 |
| Social life impacted, n (%) | 196 (65.33%) | 205 (68.33%) | 0.435 | 291 (97%) | 295 (98.33%) | 0.28 | 299 (99.67%) | 299 (99.67%) | 0.999 |
| Professional life impacted, n (%) | 199 (66.33%) | 205 (68.33%) | 0.603 | 291 (97%) | 291 (97.00%) | 0.999 | 299 (99.67%) | 298 (99.33%) | 0.561 |
Discussion
This RWE study was conducted to evaluate the effectiveness of two commonly prescribed PPIs, omeprazole and pantoprazole, for symptomatic relief of GERD/APD in treatment-naive patients. Results showed that early symptomatic resolution of heartburn, regurgitation, epigastric pain, nausea, and bloating at 14 (±7) days was evident in a significantly higher proportion of patients treated with omeprazole (20mg) compared to pantoprazole (40mg) and this significant effect was sustained till 28 (±7) days for heartburn and epigastric pain. The proportion of patients with resolution of vomiting at 14 (±7) days and resolution of regurgitation, nausea, vomiting, and bloating at 28 (±7) days was numerically higher in omeprazole (20mg) compared to pantoprazole (40mg). Concomitantly, the percentage of decrease in mean total symptom severity score was significantly higher after 14 (±7) days of treatment with omeprazole (20mg) than that with pantoprazole (40mg).
In a recent observational study on APD patients prescribed 20mg/day or 40mg/day omeprazole, 30.21% patients reported reflux on Day 28 from treatment initiation, implying that 69.79% patients had resolution of reflux [24]. The current study corroborates this data with 65.46% patients achieving complete resolution of all baseline symptoms at 28 (±7) days upon treatment with omeprazole (20mg), which was significantly higher compared to that obtained with pantoprazole (40mg) (33.48%, p<0.001). Considering the major symptoms of heartburn and regurgitation that are included in most studies on GERD/APD, the rate of complete resolution observed in the current study was, respectively, 75.77% and 75.26% for omeprazole and 56.83% and 70.93% for pantoprazole after 28 (±7) days of treatment.
Omeprazole (20mg) has been compared to pantoprazole (20mg) in an RCT of patients with grade I reflux esophagitis; symptom relief rate of all main symptoms (acid eructation, heartburn, pain on swallowing) was found to be 79%
and 84% for omeprazole (20mg) and 70% and 77% for pantoprazole (20mg) after 2 and 4 weeks of treatment, respectively [23]. Another RCT reported complete resolution of reflux symptoms in 44.0% patients after 2 weeks and in 55.0% patients after 4 weeks of treatment with omeprazole (20mg); however, the symptoms monitored in the RCT had very few overlap with those included in the current study Nagahara A, et al. [25]. Being based on real-world data, the current study compared the most-prescribed strengths of the two PPIs, omeprazole (20mg) versus pantoprazole (40mg), and is expected to reflect the present-day scenario of patient response to PPIs. While the earlier observational study reported mild treatment-emergent AEs, unrelated to omeprazole, in 4.17% patients, no AEs were reported in the current study Jain S, et al. [24]. Taken together, this suggests that the PPIs were effective, safe, and well-tolerated.
The current study further showed that patients with comorbidities or regular smoking/drinking habits attain symptom resolution of GERD/APD upon treatment with the study medications. While the latter subgroup of patients responded comparably to omeprazole and pantoprazole, GERD/APD symptoms resolved significantly better upon treatment with omeprazole compared to pantoprazole in patients with comorbidities like hypertension, diabetes, and cardiac conditions. Given that such patients might be on long-term medications for systemic diseases and that several of such medications are known to cause drug-induced esophagitis which, in turn, can be aggravated by GERD/APD, it is a crucial observation that the study medications were effective in this subgroup of patients [26].
The current study also revealed important information regarding lifestyle of GERD/APD patients. Data from this study point to a necessity of reinforcing healthy eating, sleeping, exercising, and general lifestyle routines among GERD/APD patients, if not the adult population in general. In a meta-analysis and meta-regression study from India, risk factors for GERD/APD were outlined as age, body mass index (BMI), non-vegetarian diet, tea/coffee intake, tobacco, and alcohol consumption [4]. While smoking and alcohol consumption have been dealt with in the current RWE study, it would be interesting to screen GERD/APD patients based on these and other risk factors and investigate the effectiveness of PPIs in randomized controlled trials (RCTs) in future.
PPIs being the cornerstone of GERD/APD management, it is crucial to evaluate data on their usage and effectiveness as well as ensure their judicious consumption with respect to both dose and duration of administration. Towards this, the current study provides convincing evidence to support a higher effectiveness of omeprazole in comparison to pantoprazole, particularly omeprazole (20mg) in comparison to pantoprazole (40mg), after as early as 14 (±7) days of treatment initiation. The real-world design of this study effectively mitigates constraints associated with controlled clinical trials and depicts the clinical practices and outcomes of the present day. A strength of the current study is that it included data from patients residing in geographically diverse regions in India with varying food habits and lifestyles and concomitantly reflects on the diversity of healthcare settings across the country. Another merit of this study is the comparatively higher sample size than that in the earlier report (due to SARS-CoV-2 pandemic) [24]. This study not only supports the results of omeprazole use from the earlier study but also provides comparative evidence with another oft-prescribed PPI, pantoprazole [24]. In addition to providing insights into the overall effectiveness of the PPIs, the study delves into response of patients with comorbidities or regular smoking/drinking habits.
The main limitation of this study was that it was based on retrieval of real-world data of patients from EMRs which may have led to potential biases in selection of EMRs. As is true for studies with a similar design, achieving internal validation of data was not completely feasible thus leading to a lack of quality control. Another limitation of the study was that efficacy analysis was subjective and based only on patient- reported outcomes and not on any objective assessment or diagnostic tests. However, the results from this study might serve as a basis for designing controlled and randomized prospective trials to validate the current findings. In the recent review, Shanika et al. noted that 25% users continued PPIs for over a year and 28% of these continued for more than 3 years [15]. Although this review does not include data from India, examining long-term effects of these medications in the Indian population would yield valuable information.
Conclusions
The key finding from this real-world study is that omeprazole (20mg) was observed to be more effective in resolving individual GERD/APD symptoms as well as in facilitating complete resolution of all presenting symptoms at 28 (±7) days of treatment. Its early effectiveness at 14 (±7) days is also significantly higher than that of pantoprazole (40mg). Results from this study further shows that both omeprazole and pantoprazole are effective in patients with comorbidities with omeprazole resulting in significantly better resolution of heartburn, regurgitation, and nausea in hypertensive patients, of heartburn, regurgitation, and bloating in diabetic patients, and of nausea in patients with cardiac conditions. Patients with obesity or with regular smoking/drinking habits also respond well to the treatments. Both the PPIs are safe and well-tolerated, and result in alleviating the impact of GERD/APD on hoarseness/ sore throat, sleep disturbance, eating disturbance, productive daily activities, social life, or professional life, with omeprazole resulting in significantly better resolution of hoarseness/sore throat. Overall, this study reinforces the effectiveness of omeprazole over pantoprazole under real- world circumstances. These findings might guide physicians towards better management of the rising worldwide burden of GERD/APD.
Funding: Funding for this study was provided by Dr. Reddy’s Laboratories Ltd.
Acknowledgement: The authors would like to thank participating investigators for providing electronic medical records of patients. The support of Medclin Research in study conduct, data analysis, and manuscript preparation is acknowledged.
Presentation at Meeting: APASL 2024, Kyoto Japan, 27th to 31st March 2024, PAPER presentation.
Clinical Trial Registration Number: CTRI/2023/03/051166 [Registered on: 29 Mar 2023].
Conflict of Interest: MS, MG, SR, and DB declare no conflict of interest. SM, SK, BK, GD, and RB are employees of Dr Reddy’s Laboratories Ltd.
References
-
National Health Portal of India.
-
Antunes C, Aleem A, Curtis SA (2023) Gastroesophageal Reflux Disease. StatPearls.
-
Nirwan JS, Hasan SS, Babar Z, Conway BR, Ghori MU (2020) Global Prevalence and Risk Factors of Gastro- oesophageal Reflux Disease (GORD): Systematic Review with Meta-analysis. Sci Rep 10(1): 5814.
-
Rai S, Kulkarni A, Ghoshal UC (2021) Prevalence and risk factors for gastroesophageal reflux disease in the Indian population: A meta-analysis and meta-regression study. Indian J Gastroenterol 40(2): 209-219.
-
Chen J, Brady P (2019) Gastroesophageal Reflux Disease: Pathophysiology, Diagnosis, and Treatment. Gastroenterol Nurs 42(1): 20-28.
-
Heidelbaugh JJ, Nostrant TT, Kim C, Harrison RV (2003) Management of gastroesophageal reflux disease. Am Fam Physician 68(7): 1311-1318.
-
Niknam R, Fattahi MR, Manafi A, Khazforoosh S, Mahmoudi L (2015) Management of gastroesophageal reflux disease in adults. Trends in Phramaceutical Sciences 1(2): 65-74.
-
Savarino V, Marabotto E, Zentilin P, Demarzo MG, de Bortoli N, et al. (2021) Pharmacological Management of Gastro-Esophageal Reflux Disease: An Update of the State-of-the-Art. Drug Des Devel Ther 15: 1609-1621.
-
Wang Y-K, Hsu W-H, Wang SSW, Lu C-Y, Kuo F-C, et al. (2013) Current pharmacological management of gastroesophageal reflux disease. Gastroenterol Res Pract 2013: 983653.
-
Ahmed A, Clarke JO (2023) Proton Pump Inhibitors (PPI). StatPearls.
-
Katz PO, Dunbar KB, Schnoll-Sussman FH, Greer KB, Yadlapati R, et al. (2022) ACG Clinical Guideline for the Diagnosis and Management of Gastroesophageal Reflux Disease. Am J Gastroenterol 117(1): 27-56.
-
Hunt R, Armstrong D, Katelaris P, Afihene M, Bane A, et al. (2015) Global Perspective on Gastroesophageal Reflux Disease.
-
Bhatia SJ, Makharia GK, Abraham P, Bhat N, Kumar A, et al. (2019) Indian consensus on gastroesophageal reflux disease in adults: A position statement of the Indian Society of Gastroenterology_._ Indian J Gastroenterol 38(5): 411-440.
-
Kahrilas PJ, Shaheen NJ, Vaezi MF, Hiltz SW, Blacket E, et al. (2008) American Gastroenterological Association Medical Position Statement on the management of gastroesophageal reflux disease. Gastroenterology 135(4): 1383-1391.
-
Shanika LGT, Reynolds A, Pattison S, Braund R (2023) Proton pump inhibitor use: systematic review of global trends and practices. Eur J Clin Pharmacol 79(9): 1159- 1172.
-
Massoomi F, Savage J, Destache CJ (1993) Omeprazole: a comprehensive review. Pharmacotherapy 13(1): 46-59.
-
Saboo B, Mulwani N, Petare AU, Veligandla KC, Pinto CS, et al. (2022)An Evidence-Based Retrospective Study for the Management of Acid Peptic Disease With Omeprazole, a Proton Pump Inhibitor, in Indian Patients With Type 2 Diabetes Mellitus (PRIDE-1). Cureus 14(12): e32332.
-
Klinkenberg-Knol EC, Nelis F, Dent J, Romàn J, Walan A, et al. (2000) Long-term omeprazole treatment in resistant gastroesophageal reflux disease: efficacy, safety, and influence on gastric mucosa. Gastroenterology 118(4): 661-669.
-
Schepp W, Classen M (1989) Omeprazole in the acute treatment of gastric ulcer. Scand J Gastroenterol Suppl 166: 58-62.
-
Shah N, Gossman W (2023) Omeprazole. StatPearls.
-
Ferrara F, Capuozzo M, Celotto V, Ottaiano A, Langella R, et al. (2024) Trend analysis of proton pump inhibitor consumption and expenditure: The real-world evidence. Indian J Gastroenterol 43(3): 645-651.
-
Bhalwar R (2020) Metabolic syndrome: The Indian public health perspective. Med J Armed Forces India 76(1): 8-16.
-
Bardhan KD, Van Rensburg C (2001) Comparable clinical efficacy and tolerability of 20 mg pantoprazole and 20 mg omeprazole in patients with grade I reflux oesophagitis. Aliment Pharmacol Ther 15(10): 1585-1591.
-
Jain S, Kulkarni SS, Mahapatra JR, Todi D, Petare AU, et al. (2023) Effectiveness of Omeprazole in Acid Peptic Disease: A Real-World, Patient-Reported Outcome Measures Study. Cureus 15(7): e41994.
-
Nagahara A, Suzuki T, Nagata N, Sugai N, Takeuchi Y, et al. (2014) A multicentre randomised trial to compare the efficacy of omeprazole versus rabeprazole in early symptom relief in patients with reflux esophagitis. J Gastroenterol 49(12): 1536-1547.
-
Saleem F, Sharma A (2024) Drug-Induced Esophagitis. StatPearls.
- Management of Gallbladder Perforations: A Review
- From The Mouth to the Gut: The Oral Microbiome's Role in Promoting Gastrointestinal Disease
- Case Report: Intraductal Papillary Mucinous Neoplasm (IPMN) Complicated by Portal Vein Plaquing and Biliary Obstruction Mimicking Pancreatic Metastatic Malignancy
- Management of Non-Cirrhotic Portal Hypertension during Pregnancy: A Review
- Case of Splenic Infarction; A Rare Presentation of Complicated Enteric Fever in a Pediatric Patient
- Glimpse of Metabolic-Associated Steatotic Liver Disease [MASLD] in Myanmar