Case Report: Intraductal Papillary Mucinous Neoplasm (IPMN) Complicated by Portal Vein Plaquing and Biliary Obstruction Mimicking Pancreatic Metastatic Malignancy
Intraductal papillary mucinous neoplasms (IPMNs) are premalignant pancreatic cystic lesions often detected incidentally during imaging studies. Differentiating IPMNs from other pancreatic pathologies, such as chronic pancreatitis or malignancy, poses a diagnostic challenge due to overlapping clinical and radiological features. This case report presents a rare instance of IPMN associated with portal vein plaquing and biliary obstruction in a 77-year-old male, whose medical history included chronic liver disease and diabetes mellitus. Initial imaging via contrast-enhanced computed tomography (CECT) and MRI revealed a cystic lesion in the pancreatic head, main pancreatic duct dilation, biliary obstruction, and portal vein abnormalities. Tumor markers were normal, and endoscopic ultrasound-guided fine-needle aspiration cytology (EUS-FNAC) confirmed the mucinous nature of the lesion without evidence of malignancy. Histopathological examination further validated the diagnosis of IPMN without high-risk stigmata. Notably, the patient’s amoebic serology tested positive, introducing an additional diagnostic dimension. The coexistence of portal vein plaquing, likely related to chronic liver disease, and IPMN presents a unique diagnostic and management challenge. A multidisciplinary approach ensured accurate diagnosis and effective management, which included conservative treatment for the IPMN and alleviation of biliary obstruction. This case underscores the importance of integrating advanced imaging, cytology, and clinical expertise in the evaluation of complex pancreatic lesions while emphasizing the need for ongoing surveillance in low-risk IPMN cases.
Jagdish RK¹*, Kapoor H² and Belagodu MN³
¹Senior Consultant, Gastroenterology, Hepatology, and Liver Transplant Medicine, Pan Metro Group of Hospitals, India ²Chairman and Head, Gastroenterology, Hepatology, and Liver Transplant Medicine, Pan Metro Group of Hospitals, India ³Junior Resident in Internal Medicine, Metro Heart Institute and Multispecialty, India
Introduction
IPMN is a premalignant pancreatic cystic lesion often detected incidentally during imaging studies performed for unrelated reasons. These lesions are categorized into main- duct, branch-duct, or mixed types based on their anatomical origin and radiologic features [1]. Chronic pancreatitis can mimic such presentations, complicating the diagnostic process. This report discusses a rare case of IPMN with coexisting portal vein plaquing and biliary obstruction, which initially raised concerns for pancreatic malignancy.
Case Presentation
A 77-year-old male presented with mild abdominal discomfort and a lump in the right hypochondrium. His medical history included chronic liver disease, controlled diabetes mellitus, and benign prostatic hyperplasia. Initial ultrasonography revealed a pancreatic lesion, necessitating further evaluation via contrast-enhanced computed tomography (CECT). The CECT demonstrated a cystic lesion with enhancing septa in the pancreatic head, alongside dilation of the main pancreatic duct and biliary obstruction.
MRI findings corroborated these results, indicating compression of the distal common bile duct and portal vein abnormalities, suggestive of intraluminal plaquing.
To confirm the diagnosis and exclude malignancy, tumor markers (CA 19-9 and CEA) were tested and found to be within normal limits. EUS-FNAC was performed, and the aspirate analysis identified mucinous cystic features without malignant cells. Histopathological examination confirmed the diagnosis of IPMN with no evidence of high-risk stigmata. Interestingly, the patient’s amoebic serology tested positive, introducing an additional layer of diagnostic complexity (Figures 1 & 2).
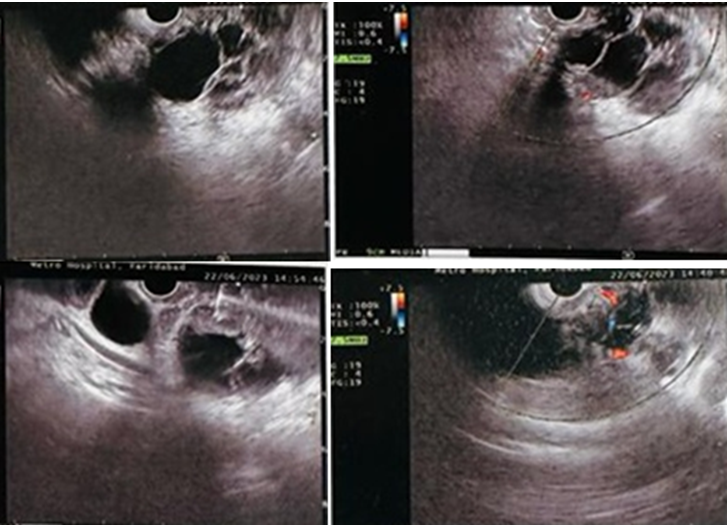
An endoscopic ultrasound (EUS) was performed using an Olympus endoscopic ultrasound scope. It revealed multiple cysts in the pancreatic head and uncinate process, measuring approximately 4.1 × 5.7 cm. These cysts demonstrated multiple septations, with mild dilation of the pancreatic duct noted. The common bile duct appeared normal. Fine-needle aspiration (FNA) of the cyst was performed, and the findings excluded features consistent with a hydatid cyst, such as daughter cysts. The aspirated material was subjected to cytological and histopathological analysis.
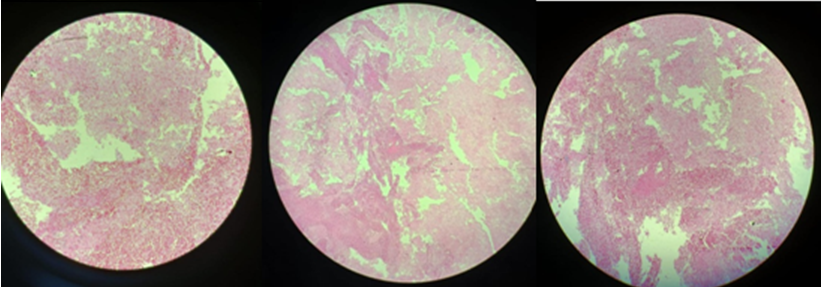
Histopathological evaluation of the aspirated material from the pancreatic cyst confirmed the presence of blood and proteinaceous material. Additionally, foamy macrophages were observed, without any evidence of atypical or malignant cells. The findings were indicative of a mucinous cystic lesion, consistent with an intraductal papillary mucinous neoplasm (IPMN).
Discussion
The coexistence of IPMN with portal vein plaquing and biliary obstruction presents a unique diagnostic challenge. IPMNs are known to exhibit varying degrees of malignant potential based on their size, duct involvement, and associated features such as nodules or biliary obstruction [2]. In this case, radiological findings raised suspicion for a mucinous neoplasm, while EUS-FNAC provided critical histological confirmation.
Portal vein plaquing, observed in this patient, is a rare finding that can be attributed to chronic liver disease or thrombosis-related sequelae [3]. The biliary obstruction, caused by compression from the pancreatic lesion, necessitated further evaluation through ERCP or surgical intervention to prevent complications like cholangitis.
Diagnostic Challenges and Differential Diagnosis
Differentiating IPMN from other cystic pancreatic lesions, such as mucinous cystic neoplasms (MCN) or pseudocysts, requires a combination of imaging and histological analysis. While MRI and CT scans aid in visualizing structural abnormalities, EUS-FNAC is indispensable for obtaining tissue samples for histopathological confirmation [4]. In this case, the lack of malignant cells on cytology and normal tumor marker levels were crucial in ruling out malignancy.
Management and Multidisciplinary Approach
The management of IPMN hinges on its location, size, and risk stratification. High-risk lesions necessitate surgical resection, while low-risk lesions may be managed conservatively with surveillance [5]. In this case, the absence of high-risk features allowed for non-surgical management, focusing on alleviating biliary obstruction and monitoring for disease progression.
Conclusion
This case highlights the importance of an integrated diagnostic approach in managing complex pancreatic pathologies. Multidisciplinary collaboration involving gastroenterologists, radiologists, and hepatobiliary surgeons ensures accurate diagnosis and optimal management. Further studies are warranted to explore the interplay between portal vein abnormalities and pancreatic cystic neoplasms.
References
-
Tanaka M, Chari S, Adsay V, Castillo CF, Falconi M, et al. (2007) International consensus guidelines for the management of IPMN and MCN of the pancreas. Pancreatology 6(1-2): 17-32.
-
Watanabe Y, Endo S, Nishihara K, Ueda K, Mine M, et al. (2018) The validity of the surgical indication for intraductal papillary mucinous neoplasm of the pancreas advocated by the 2017 revised International Association of Pancreatology consensus guidelines. Surg Today 48(11): 1011-1019.
-
Ponziani FR, Zocco MA, Campanale C, Rinninella E, Tortora A, et al. (2010) Portal vein thrombosis: insight into physiopathology, diagnosis, and treatment. World J Gastroenterol 16(2): 143-155.
-
Pozzi-Mucelli RM, Rinta-Kiikka I, Wünsche K, Laukkarinen J, Labori KG, et al. (2017) Pancreatic MRI for the surveillance of cystic neoplasms: comparison of a short with a comprehensive imaging protocol. Eur Radiol 27(1): 41-50.
-
Machado NO, Qadhi HA, Wahibi KA (2015) Intraductal Papillary Mucinous Neoplasm of Pancreas. N Am J Med Sci 7(5): 160-175.
- Management of Gallbladder Perforations: A Review
- From The Mouth to the Gut: The Oral Microbiome's Role in Promoting Gastrointestinal Disease
- Management of Non-Cirrhotic Portal Hypertension during Pregnancy: A Review
- Effectiveness of Omeprazole versus Pantoprazole for Symptomatic Relief of Gastro-Esophageal Reflux Disease (GERD)/ Acid Peptic Disease (APD): A Real-World Evidence (RWE) Study
- Case of Splenic Infarction; A Rare Presentation of Complicated Enteric Fever in a Pediatric Patient
- Glimpse of Metabolic-Associated Steatotic Liver Disease [MASLD] in Myanmar