Fine Needle Aspiration Cytology Aided by Skinfold Caliper in the Diagnosis of Lymphoadenopathy in the Tropics
Cervical lymph node proliferation have been associated with many tropical diseases that may not warrant lymphadenectomy or unguided needle aspiration nowadays. Most palpable cervical lymph nodes in the tropics investigated by fine needle aspiration cytology and have proved to be lymphadenitis. In seven years are 222 patients that had cervical lymph node enlargement and/or multiples were investigated for size with skin fold caliper and aspirated with mounted 23 gauge needle on 2ml/ 5mlhypodermic plunger. Occurring was 55.4% male of age range 25 to 46 years, and 44.6% female whose age were 8 to 56 years. Of both sexes were 10% diagnosed of Human immunodeficiency virus (HIV) of 3 years duration manifestation and were apparently healthy with enlarged and multiple cervical lymph nodes. The texture of nodes varied inconsistency and firm nodes were dominant. Clinically confirmed ill-health patients were 91.4% of 222, and have had multiple visits while 8.6% were on their first visit but because of size and/or number of nodes occurring were aspirated. Of the 6 age group that occurred, 20 – 29 and 30 – 39 were most and more involved respectively showing also in the same position of multiple numbers of nodes occurrence. Largest node was found in 8 years old girl which age group was of less number of nodes. Eight disease conditions were present with 8 years 6 months highest duration prior to investigation. Bilateral side neck node occurrence is 80 cases and, 110 and 32 appeared laterally right and left respectively. In-situ size of node to gross of node was 3:2 dominating while cervical skin fold versus lymph node skin fold plateau was inconsistent and present bizarre ratio of no disease significance. Cyto-morphological findings were specific for varying degrees of inflammation, and acellular slides were found prevalent with seven of the diseases.
Introduction
Fine needle aspiration cytology (FNAC) of lymph node in recent time has become increasingly applicable to the diagnosis of inflammatory and cancer diseases. The significance and importance are in the rapid identification and characterization of diagnosed infecting agents of internal organs and peripheral lymph node. Rapid diagnosis occasioned by fine needle aspiration cytology has in recent time improved [1] from screening of internal organs to interventional by the use of narrow gauge (25-22G) needle and other directional explorative procedures for microscopic examination of sample collected. These clinical and diagnostic practices are not adsorbed of many demerits as there are distortion of histological tissue architecture, inadequacy of samples and bad preparation of slides. These have resulted to limited affirmation of accurate diagnosis and sometimes cause definitive diagnosis to remain subjective to clinician’s opinion. Consequently, accuracy of results from FNAC techniques that require interpretations of well prepared and stained slides should include the cellular features, their distribution pattern, population and types, quality and quantity, and background reaction among other standardized factors. Also, the issue of false positive and especially false negative outcomes makes the techniques considered useless or dangerous [2]. Therefore, it is true that in the presence of well situated site of lesion Aspirator or the preparation of smear may grievously affect outcome of result than other factors [3, 4]. The clinical and radiological correlation with FNAC to ascertain diagnosis has been subjective, and is found useful particularly for rapidity of results, cost effectiveness, and accurate diagnosis [5, 6]. Aiding of clinical examinations with improved technologies is to increase precision of diagnosis as in liver aspiration by FNAC [7, 8] and enhance limited unnecessary procedures particularly in the collection of specimens. There are limited reports of aiding FNAC bio-sampling with electron microscopy for diagnostic precision [9, 10, 11, 12, 13] and in the development of specialized diagnostic techniques [13, 14, 15, 16, 17, 18] but not for clinical examination. Therefore the application of fine none-invasive technology in clinical examination and sample collection to aid FNAC may aim at reduction in inadequacy of sample, [9, 10, 11] increase in site appropriateness of provisionally diagnosed lesion, and produce less skin scaring [12] and be cost effective as required.
Lymphoadenopathy arises from several general body ill-health conditions most of which are associated with immune disorders, [19] benign and cancerous tumors,20 micro-organism infection, and parasite setting [1, 21] When other occult factors cause proliferation and enlarged lymph nodes it is always subject to some genetic disorders, [22, 23] which do result or consequent generalized lymphoadenopathy. Also certain physical stress like sports and trauma have been known as clinical factors to induce lymph secretion and eventual occlusion of lymphoid sinuses and enlargement [24] of inguinal and possibly cervical node. Such sterile conditions are said to vanish or resolve in limited hours without much serious medical attention, while persistent forms may be as occasioned by hidden clinical conditions prior to bodily exercise or trauma. Enlargement and proliferation of cervical lymph node is caused by inflammation due to tuberculosis, tumor and other pulmonary communicating diseases [25] and promoted multiplicity are obvious among different age groups particularly when there is immunodeficiency disorder. Lymph node is common at body loosed and folds regions, and do appear as raised or folded skin depending on site of the region just like skin fold areas, which also include where the skin is designed to fold or to accommodate movement [26, 27]. At other sites where skin fold are non-specific, nodes appearance is produce by infectious micro-organism or by arbitrary application of force to skin, either by the actions of the muscles of the body or by external force. Such folds are easily produced in fitness centers but literally measured by pinching parts of the body with two pincers of caliper [28]. Considering the huge patient benefits and easy associated with FNAC, skin fold caliper, a pincer device mostly designed for use to measure the amount of non- lean tissue on the body was attempted on palpable and prominent lymph nodes to generate analyzable rough estimate of skin folds produced by resident lymph nodes. Analyzed and obtained sizes will be subjected to clinical and laboratory results to ascertain the relationships between size, topography of the skin fold and morphologic characters of lymph nodes to incident of individual disease that may occur.
Materials and Methods
In the seven year study were 222 patients of the Departments of MOPD and SOPD Ebonyi State University Teaching Hospital, Abakaliki from year 2005 to 2012 who were referred having prominent lymph nodes to Department of Morbid Anatomy with their clinical folders and treatment chart from Heart-To-Heart clinic, and request forms indicating provisional diagnosis, clinical summary, and site of sample collection. Following caliper measurement, 100 patients with prominent lymph nodes among the 222 had lumpectomy of their lymph node, samples and request forms were submitted to Department of Morbid Anatomy by the SOPD clinical team. These were paraffin wax processed for general tissue architecture after 10% formal saline fixation. To 122 samples, the clinical sizes of the chosen lymph nodes in-situ were also carried out with Slim Guide skin fold caliper which provided accurate measurement of subcutaneous tissue. The pivoted tips was allowed a jaw pressure of 10g/mm2 and when adjusted provided parallel measurement of skin folds plateau as given by the subcutaneous tissue and the protruded lymph nodes. Further measure of subcutaneous of the adjacent skin area to the lymph node gave credence to the use of the regressive equation to calculate body density ( BD) as follows; BD = 1.10938 – (0.0008267 x sum of 2 skin fold) + (0.0000016 x sum of 2 skin fold) – (0.0002574 x age)29 but for the nodes simple formula of thus; Sizes of node in-situ (S_ni_) == skin fold plateau size (SF_ps_) minus adjacent skin fold size (SF_s_).
Sni = SFps –SFs (1) Mathematically this means, ni =Fps – Fs (2) Therefore area occupation of the skin plateau measured with Skin Fold Caliper was deducible b as shown below. Therefore lymph node size can be found from thus; π(R- r1)2 r2 is same as R2from πr2, R2 = (r1+r2)2, and r2 = (R- r1)2 for figure 1A in-situ before measurement, and during measurement and on application of hand pressure the node site as to increase plateau, and resultant is change of shape and size as in figure 1B. Therefore shape measureable was ellipsoidal lymph node which size was different from lymph node in-situ because of physiochemical changes as tissue fluid is pressed out and inflammatory processes followed. Hence, A= πR1R2- πr1r2. Thus, A =πR1R2- πr1r2, is π(R1R2 – r1r2). The accurate lymph node size was further obtained by subjecting size in-situ to the 100 lymph node excised and fixed. Values obtained were compared with the value of gross nodes after fixation with 10% formal alcohol.
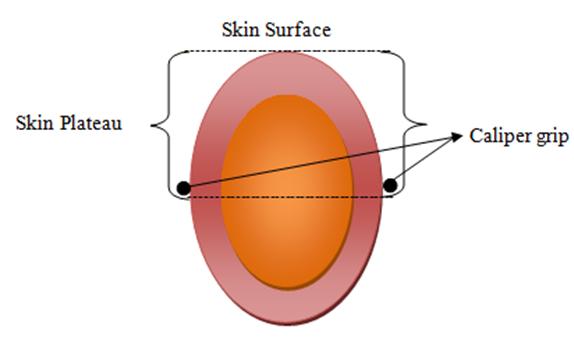
Figure 1A: Cervical Lymph node in-situ before measurement. Figure 1B: Possible position of superficial Cervical Lymph node under the skin, skin plateau formed and Skin Caliper grip.
Slim Guide Skin Ford Caliper Measurement Method
All the patients were made to sit down on a comfortable clinic chair with two hands resting on the arm-rest of both sides of the seat. Patients were inclined in a positive up-right position and asked to focus on color chart mat hung at a distance of 40 meters. This measure eliminates the unnecessary skin folding at the cervical and neck regions which would have increased skin-fold size as patients try to re-adjust neck prior and during measurement with the caliper. Since the caliper can measure up to 280mm and can be read to the nearest 0.5mm with dual springs for consistent measurements, the adjustment in time does not take any significant time during usage. To patients with insufficient prominence but palpable nodes, four fingers were applied at skin touch level without exacting unnecessary pressure few centimeters away from node site, and traced to the node site then minimal pressure applied to detect node position. With gentle and steady fingers, little plateau is made as the node is probed upward, and measurement taken after appropriate adjustment of caliper tips (figure IB). Two measurements were taken and recorded from cervical skin fold and from the node and skin fold.
Fine Needle Aspiration Cytology (Fnac) Method
Aspiration was done immediately after caliper measurement. Lymph node site having been well located and was held with one hand while swabbed clean and dry to decontaminate skin site before the immediate puncture. The nodes were punctured with a mounted 2/5ml syringe with 23 gauge hypodermal needles which had been withdrawn halfway. On piecing the nodes through the skin, the plunger of the syringe was pushed to exact air pressure into the node. The needle is pulled back and forth, sideways up and deeper the node for few seconds making cautious effort not to draw in blood or piece through the nodes. This was to ensure proper aspiration of fluid from across the diameter of each node. On final withdrawal of needle, detach needle from syringe. Pull back the plunger to admit air in with which to push out fluid from needle for smears. Three slides were made from each case. One was allowed to air-dry before all were fixed in 10% formal alcohol for not less than three hours.
Staining of Cytological Slides
The slides were first reassessed for appropriateness and adequate content by naked eye visualization before staining. Two staining techniques were preferred and used to reveal the presence of lymph node cells; for good demonstration of nuclear, cytoplasmic morphologies and general cellular distribution pattern on the background field; that is, popular Harris heamatoxylin and Leishmann. For the presence of Acid Fast Bacilli, Zeihl Neelsen technique was adopted.
Results
Of the 222 patients consulted by the Unit of Cytopathology were from MOPD and SOPD of EBSUTH and now Federal Teaching Hospital Abakaliki, had 55.4% (123) males whose age ranged from 25 to 46 years, and 44.6% (99) females of age range 8 to 56 years. For both sexes, 10% (23) were diagnosed of Human Immunodeficiency Virus (HIV) three years before the clinical manifestation of multiple and/or enlarged cervical lymph nodes. Six of these were males of age range 25-36 years and the remaining 17 females were within the ages of 18-33 years save for one 8 years old girl whose mother tested positive for HIV. Three large lymph nodes were observed on her, which was confirmed to have started reducing in size two months from date of onset of medical regiment. All the 23 patients were apparently healthy as they were on retroviral drug administration program six months after having been clinically established of infection with HIV by Heart-To-Heart clinic. All 222 patients have prominent palpable cervical lymph nodes which sizes varied inconsistently irrespective of age, while the largest nodes were observed with one 8 years old HIV positive girl and three 24 years old male patients (Table 1). Bilateral occurrence of node was 80 cases, and lateral right and left of the neck was 110 and 32 respectively. With 30 of the 80 bilateral nodes in patients appearing more than one node per side and, 2 of cases were found 3 nodes per the two sides but are of varying sizes. The texture of all the nodes varied and firm nodes dominant regardless of number that occurred per patient, and in others of soft consistency were pus-like aspirates obtained, while firm nodes yielded bloody aspirates when no fluid. From the 222 patients involved in the study, 203(91.4%) had been clinically confirmed with ill-health as stated in table II, while 19(8.6%) were at their first visit and because of the size of their lymph nodes and number request were made for fine needle aspiration cytology investigation. These were not cytological confirmed of any particular disease by FNAC not even for reactive hyperplasia which was 2.3% (5 cases) by biopsy specimens while normal is 92% (204), and others were mere inflammation, tuberculosis and others conditions as in table II. Also tuberculosis showed highest prevalence and presented more lymph node proliferations in number and size, and was found to be complication advent from HIV in 7 of the male patients (Tables 1 & 2).
Cytomorphological Finding
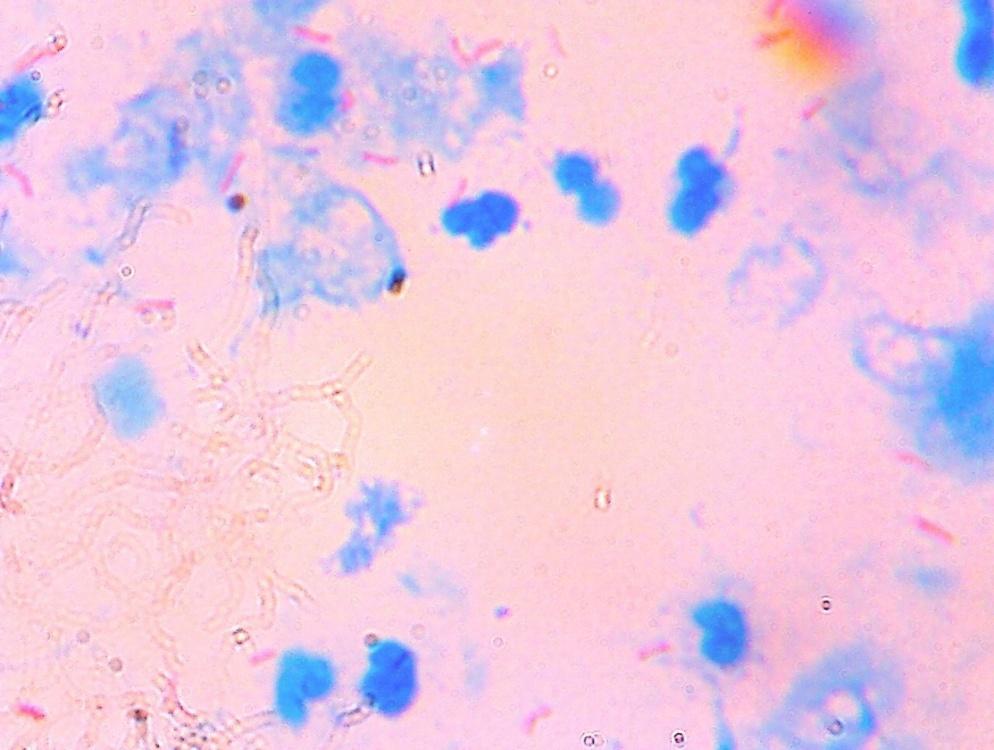
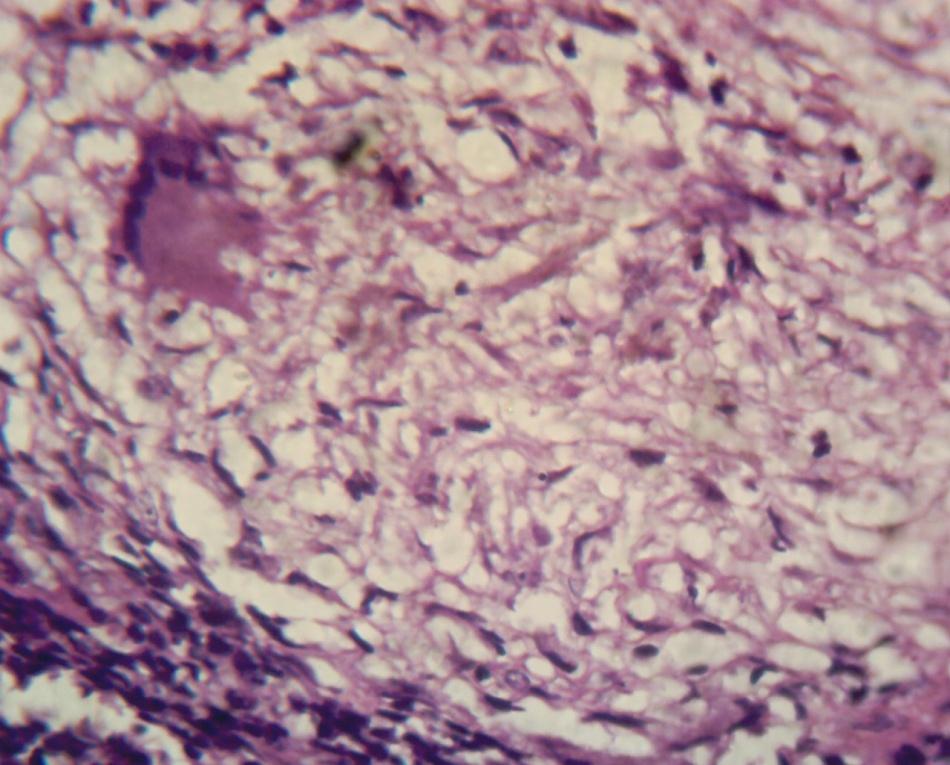
Cytomorphological features varied and in most cases were normal. There was my cobacteria tuberculosis by Acid Fast Bacilli (AFB) method producing lymphocytic proliferation in some slides and in 25 others (Figure 1) were cellular or a cellular and positive for AFB. In the latter, histology of lumpectomy yielded epithelioid cells, Langhan’s cell and caseous necrosis among which were features that supported granuloma (Figure 2).
Skinfold Caliper Finding
Sizes of lymph nodes were found to vary and the largest average size of 13.6mm+-0.42 was obtained from 8 years old girl and two males 22 years old each, who were diagnosed of HIV and TB infections.
Insitu measurement of nodes size was calculated with the formula that eliminates the skin fold size from general size of node and skin fold. Node size = skinfold and node size minus skinfold size. A ratio of 3: 2 (node in-situ size: gross node size) table1.
| Age group | Male | Female | Site of node | In-situ average size (mm) | Total Number of node Observed In-situ | Total number of nodes removed per age group | Gross Average size (mm) | |
| Age group | Male | Female | Left | In-situ average size (mm) | Total Number of node Observed In-situ | Total number of nodes removed per age group | Gross Average size (mm) | Right |
| 8-9 | - | 2 | 3 | 1 | 13.8 | 4 | 2 | 9.8 |
| 10-19 | 12 | 8 | 10 | 18 | 3.7 | 28 | 24 | 1.6 |
| 20-29 | 45 | 35 | 36 | 52 | 12.5 | 88 | 82 | 7.8 |
| 30-39 | 33 | 25 | 30 | 31 | 2.8 | 61 | 58 | 0.7 |
| 40-49 | 17 | 15 | 18 | 22 | 4.5 | 42 | 33 | 1.6 |
| 50-59 | 16 | 14 | 20 | 19 | 4.6 | 39 | 59 | 2 |
| Total | 123 | 99 | 97 | 125 | 262 | 258 |
Table 1: Clinical statistics as found in the age groups of both sexes cervical lymph node with skin fold caliper.
- Diseases
- Males
- Females
- Duration of node occurrence on
- Duration of illness before node occurrence
- Malaria
- 3
- 5
- 2 weeks - 1 month
- 2 days
- Drug Reaction
- 4
- 10
- 3 weeks - 3 months
- 3 weeks
- HIV
- 6
- 17
- 1 – 8.6 years
- 1.6 years
- Tuberculosis (TB)
- 50
- 23
- 2 years (Discovered at the chronic stage)
- 2 years
- Chronic Bronchitis excision (Recurrent)
- 20
- 6
- 2 - 5 years
- 3 months
- Typhoid Disease
- 28
- 22
- 4 – 8 months
- 1 week
- Chronic Pneumonia
- 10
- 15
- 3 – 6 years
- 2 weeks
- Sarcoidiasis
- 2
- 1
- Total
- 123
- 99
Table 2: Diseases and Clinical characters presented by diseases.
Discussion
FNAC has been of great use in the diagnosis of various lesions and diseases prior to intra-operative and post- operation [2, 9, 20, 29] This informed of the approach which warranted dimensional and statically evaluation of nodes in-situ and the comparison of the cytology finding with many negative and positive cases associated with lumpectomy. The idea was as well to confirm whether FNAC of cervical lymph node can reveal TB and other diseases of patients as is possible with other sites in the body [30]. However the study revealed 11.8% success of the organism – Mycobacterium tuberculosis among other cellular feature (figure II). Also since majority of FNA cytology proved negative for histologically positive cases, common sense from morphology lumpectomy is to confirm such cases that were positive granted that clinical history supports histomorphologic features, as figure 3 has shown.
Consequently, the failure of FNA cytology to ascertain the extent of diseases were obvious in this study and command the conclusion that FNA cytology may not be the ideal request for nodular TB in screening designs as well as other diseases with lymph node enlargement and proliferation [31]. Reasons for the failure did not preclude consistence of nodes but inclusively size, age and shape. Also it has been reported in studies that complication of immunodeficiency virus (HIV) include TB which might end patient’s life or put patients in multiplicity of complications, and other diseases may evolve from same virus or similar types. Reports were that TB in an individual could provoke several disease conditions as patient immunity dwindles [32]. Therefore, the presence of other diseases complication cannot be considered as a feature for FNAC accuracy as shown in this study.
In situ search also refers to as clinical evaluation of patients was attempted by using Slim guide skin fold caliper because of its reliability in measurement [1, 33, 34]. However, the result from multiple nodes per patient was found size distinguishable (table I) and informed no specific relationship with disease type. Comparison of size in-situ and gross gave variation in the average ratio of 3: 2 (in situ: gross), but the finding has no significance in FNAC ability to predict positive case of any disease. Hence FNAC positivity of TB and other diseased lymph node was not size dependent from this study as was possible in developing adult [35]. The 11.3% positive FNAC lymph node TB were all of soft consistence and exude pale fluid tinged with blood. This may be as a result of lymph node structural damage by such disease and necrosis was resultant. Such finding has not been report of lymph node TB to our knowledge. From figure 2 it is evident that amidst lymph node reaction against the organism, necrosis occurs and pus formed as in infectious necrosis. For other diseases morphologic features were evident of lymphocyte proliferation save for sarcoidiasis in which stained slides were plain and acellular. Even size justification cannot be attempted because same sizes were found of typhoid disease, chronic bronchitis and pneumonia. Extra 48 lymph nodes were observed in-situ, and statistics show 29 to 19 extra nodes (male to female) resulted, meaning that 123 males and 99 females showed significant considerable difference when multiple proliferation of lymph node in sex involvement was analyzed. Consequently, does this finding have any clinical diagnostic importance to predicting accurately different types of diseases before laboratory investigation result? Again, considerable significance was found in age groups (20 – 29) and (30 – 39) producing 28 extra nodes than others. When this was related to the general population in the study in which these two age groups contributed 62% of patients, showing that there was obvious remarkable clinical significance capable of influencing patho- physiological and socio-medical judgments. This is because these age groups are the work force age for farming in the tropics regardless of sex, and may hardly have access to affordable quality healthcare. It is interesting to note that no case of malignancy was established by FNAC and biopsy diagnoses. Several of clinical signs and symptoms were not pointer towards suspicion of such disease in our study. Does this mean that cervical lymph node proliferation or and multiplication is not associated with malignancy in the tropics? Our response to this question is as in a study [36], and answer may not be required since the sample size was not that much (as many Clinician hardly request for cervical node FNAC) for the years under search and the fact remained unresolved since the geographical location is prone to lymphoma and or any other malignant lesion that is noted to produce lymphoadenopathy [37]. Conclusively, FANC is not 100% accurate for lymph node TB diagnosis, and should be considered based on the consistency of node rather than size, age of node and shape. Also multiplicity and proliferation of lymph nodes in age groups are possible occurrence, and may not affirm or predict type and age of disease or diseases that prompted such clinical manifestation. Again, lymph node plateau and skin fold presence that produced measureable differential ratio in size may be of subjective clinical importance when tropical diseases are considered.
References
-
Lee H, Yoon TJ, Figueiredo JL, Swirski FK, Weissleder R (2009) Rapid detection and proliling of cancer cells in fine-needle aspirates. Proceedings of the National Academy of Sciences of the USA. 106(30): 12459- 12464.
-
Metcalfe MS, Bridgewater FHG, Mullin ES, Maddern GJ (2004) Useless and dangerous fine needle aspiration of hepatic colorectal metastases. British Medical J 328: 507-508.
-
Snead DRJ, Vryenhoet P, Pinder SE, Evans A, Wilson HRM et al (1997) Routine audit of breast fine needle aspiration (FNA) cytology specimens and aspirator inadequate rates. Cytopathology 8: 236-247.
-
Singh N, Ryan D, Berncy D, Calamini G, Sheaff MT (2003) Inadequate rates are lower when FNAC samples are taken by Cytopathologist. Cytopathology 14: 327-331.
-
Buley ID, Roskell ED (2000) Fine needle aspiration cytology in tumor diagnosis: Uses and limitations. Clinical Oncol 12: 166-171.
-
Derek E Roskell, Ian DB (2004) Fine needle aspiration cytology in cancer diagnosis. Is quick, cheap, and accurate when used appropriately. BMJ 329 (7460) 244-245.
-
Herszenyi L, Farinati F, Cecchetto A, Marafin L, De Maria Della Libera G, et al. (1995) Ultrasound guided fine-needle aspiration biopsy diagnosis of hepatocellular carcinoma. Orv Hetil 136(29): 1545- 1549.
-
Michielsen PP, Dugsburgh IK, Francque SM, Vander Planken M, van Mark EA, et al. (1998) Ultrasound guided fine needle puncture of focal liver lesions. Review and personal experience. Acta Gastroenterol Belg 61(2): 158-163.
-
Dabbs D, Silverman JF (1989) Selective use of electron microscopy in fine needle aspiration cytology. Arch Pathol Lab Med 113: 1353-1356.
-
Yazdi HM, Dardick I (1988) What is the value of electron microscopy in fine needle aspiration biopsy? Diagn. Cytopathol 32: 880-884.
-
11. Wills EJ, Carr S, Philips J (1987) Electron microscopy in the diagnosis of percutaneous fine needle aspiration specimens. Ultrastruct Pathol 11: 361-387.
-
Njordgren H, Akerman M (1982) Electron microscopy of fine needle aspiration biopsy from soft tissue tumors. Acta Cytol 26: 179-188.
-
Mackay B, Fanning T, Bruner JM, Steglich MC (1987) Diagnostic electron microscopy using fine needle aspiration biopsies.Ultrastruct Pathol 11: 659-672.
-
Castro MR, Gharib H (2003) Thyroid fine needle aspiration biopsy; progress, practice and pitfalls. Endocrine Pract 9: 128-136.
-
Odselius R, Falt K, Standell L (1987) A simple method for processing cytologic samples obtained from body cavity fluids and by fine needle aspiration biopsy for ultra structural studies. Acta Cytol 31: 194-198.
-
Lazzaro AV (1983) Technical note: Improved preparation of fine needle aspiration biopsy for electron transmission microscopy. Pathology 15: 399- 402.
-
Akhtar M, Bakry M, Nash EJ (1986) An improved technique for processing aspiration biopsy for electron microscopy. Am J Clin Pathol 85: 57-60.
-
Di Sant’ Agnese PA, de Mesy Jensen KL, Bonfiglio TA, King DE, Patten SF Jr (1985) Plastic–embedded semi- thin section of fine needle aspiration biopsies with dibasic staining diagnostic and didactic applications. Acta Cytol 29: 477-483.
-
Orell SR, Phillips J eds (1997) The role of fine needle biopsy in the investigation of thyroid diseases and its diagnostic accuracy. In: The thyroid, fine needle biopsy and cytological of thyroid lesions. Monographs in clinical cytology. 14: 8-9 (chapter 3).
-
Frable WJ (1983) Fine needle aspiration biopsy. A review. Human Pathol. 14: 9-28.
-
Vinay K, Abul KA, Nelson F, Robbins and Cotran Pathologic Basis of diseases Unit II, Disease of organ system. Chapter 11. Blood vessels (Frederick J Schoen). Benign tumour-like conditions- Lymphagiomas. 7th (Edn), Elsevier Publisher- Saunders 2004. Pp: 511-554.
-
Jon C Aster (2004) Diseases of white blood cells, lymph nodes, spleen and thymus . In: Robbins and Cotran Pathologic Basis of disease. 7th (Edn) Pp: 661- 709.
-
Schulz TF (2001) KSHV/HHV8-associated lymphoproliferations in the AIDS setting. Eur J Cancer 37(10): 1217-26.
-
Hecht JL, Aster JC (2000) Molecular biology of Burkitt’s lymphoma. J Clinical Oncol 18(21): 3707-21.
-
Shipp MA (1994) Prognostic factors in aggressive Non-Hodgkin’s lymphoma: Who has ‘high-risk’ disease? Blood 83: 1165-1173.
-
Gharib H, Goellner JR (1993) Fine needle aspiration biopsy in the investigation of thyroid: an appraisal. Ann Intern Med 119: 282-289.
-
Dorland’s illustrated Medical Dicionary for health consumers (2007) 27th (Edn), Pp: 645-646.
-
Mackenzie B Facts about fat (www), available from htpp: //www. Brain Mac.uk fat. Htm (assessed 10/7/2012).
-
Jackson AS, Pollock M (1985) Practical Assessment of Body Composition. Physician Sport Med 13(5): 76-90.
-
Buscaini L, Fornari F, Bolondin L, Colombo P, Livraghi T, et al. (1990) Ultrasound- guided fine needle biopsy of focal liver lesions: techniques, diagnostic accuracy and complications. A retrospective study on 2019 biopsies. J Hepatol 11: 344-348.
-
Handa UA, Palta, H Mohan, Punia RP (2002) Fine needle aspiration cytological diagnosis of tuberculosis lymphadenitis. Tropical Doctor 32: 147- 149.
-
Ahuja A, Ying M, Yuen YH (2001) Power Doppler sonography to differentiate tuberculosis of cervical lymphadenitis from nasopharyngeal carcinoma. AJNR Am J Neutrorsdiol 22(4): 735-740.
-
Jha BC, Dass A, Nagarkar NM (2001) Cervical tuberculosis lymphadenitis: changing clinical pattern and concepts in management. Post Grad Med 77 (905): 185-187.
-
Bays HE, González-Campoy JM, Bray GA, Kitabchi AE, Bergman DA, et al. (2008) Pathogenic potential of adipose tissue and metabolic consequences of adiposity hypertrophy and increased visceral adiposity. Expert Rev Cardiovascular 6(3): 343-368.
-
Blair S (2002) The public health problem of increasing prevalence rates of obesity and what should be done about it. Mayo Clinic Proceedings 2: 109-113.
-
Onimawo LA, Cole AH (2002) A longitudinal study of changes in the body composition of young adult Nigerian. J Sci 1: 47-113.
-
Kim BM, Kim EK, Kim MJ, Yang WI, Park CS , et al. (2007) Sonographially guided core needle biopsy of cervical lymphadenopathy in patients without known malignancy. J Ultrasound Med 26: 283-591.
- Forensic Implications of Adverse Drug Reactions in Schizophrenia A Case Series
- Narcotics and Digital Forensics: Bridging Crimes in the Digital Age
- Ethics in Forensic Psychiatry: Principles, Dilemmas, and Human Rights
- Impact of Acute Stress on Attentional Orienting to Social Cues
- Head Injury and Intracranial Hemorrhage in Western Region of Libya
- A Forensic Study on Handedness: Examination of Handwriting Features in Right and Left Handed Writers