Dermatoglyphics - A Morphological Biomarker in Human Ailments: A Review
The features of the hands have always attracted man to find his future. After research of decades by many, the hand has come to be known as reflection of his self and a useful tool in the diagnosis of psychological, medical and genetic conditions. Finger and palmar dermatoglyphics have been observed to be indicators of certain ailments and health disorders. Their scope may be utilised to predict the problem and implement preventives measures to rectify. India, a developing country, can do with such non-invasive, inexpensive and effective indicators of health. In this paper, the work done by various research scholars has been studied to determine the importance of Finger and palmar dermatoglyphics in the study of ailments.
Introduction
Fingerprints and palmar prints are reproductions of epidermal ridges. The ridges are formed in early stages of formation of embryo and are fully formed by 16th week of intrauterine life. Formation of a dermatoglyphics pattern is guided by the genes present in the embryo. A relationship exists between epidermal ridges and volar pads. The volar pads are formed due to swelling of mesenchyma tissue at the areas of ridge formation and regress when ridges start forming. External pressure on fetal pads and embryonic fetal movements also influence the ridge formation. The ridges so formed remain constant from birth to death till destroyed permanently, except slight changes in dimensions proportionate to the growth of a person.
Fingerprints were used as a mark of evidence in the olden days. According to archaeological survey, fingerprints and palm prints were found on clay artefacts and documents in Assyria and Babylon. Dermatoglyphics were used by Chinese as signature, thousands of years back. Dermatoglyphics is the scientific study of frictional ridge patterns present on the fingers, palms of hands, toes and soles of feet. Initially the purpose of frictional ridges is to create friction between the surface being held and the hand/ feet.
Marcello Malpighi [1] studied skin, its function, form, structure of friction ridges and observed that ridges on skin act as traction between object and skins surface and help in walking and holding objects.
Meyer [2] was the first to observe the individuality and uniqueness of the ridges which he mentioned in his study with diagrams. Sir Galton [3] identified the minutest characteristics of ridges as minutiae, and made observations that friction ridge skin was unique and persistent. The minutiae were later named as Galton’s details.
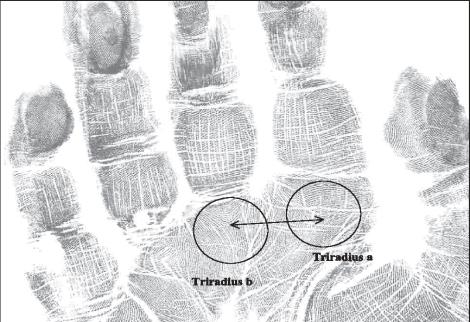
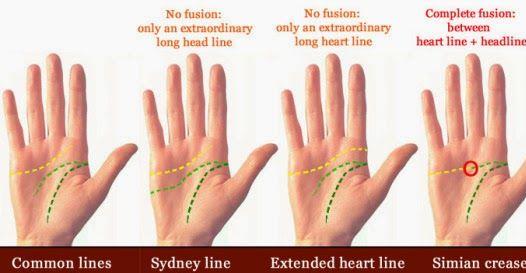
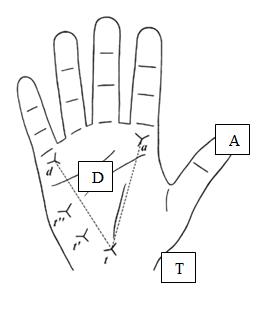
The finger and palm prints contain a lot of information like a map and can be used for research, understanding of potential and talent of a person and as diagnostic tool for study of diseases, besides identification. Personality, temperament and character can also be correlated with fingerprint pattern. Whorls show stubbornness, loop shows lack of perservance, arches denote crude behaviour and composite denotes unreliable character. Features as occurrence of a particular pattern in fingers, ATD angle, a-b ridge count, simian crease and Sydney crease and other measurements in the palm are important in the study of dermatoglyphics.
Harold Cummins [4] analysed and suggested the possible use of dermatoglyphics in clinical medicine. In the recent times, many studies were conducted on finger and palmar dermatoglyphics and relationship between certain types of ridge patterns, palmar lines and individual disorders was obtained.
Gupta, et al. [5] observed high frequency of palmer pattern in thenar and 1st Inter digital area on left palm, with high frequency of Simian Crease on palms of multibacillary leprosy patients.
Ciovirnche, et al. [6] found that thyroid cancer males had a more marked transversality of the A line than the control group and also observed that cancer subjects had a higher incidence of typical and atypical forms of transverses and patterns in the second ID space than the controls.
Abbas, et al. [7] observed that there was presence of 6 or more digital whorls out of 10 digits in patients with breast cancer, whereas Sukre, et al. [8] found increase in the values of median a-b ridge count on left whereas on right hand, it was not significant.
Sharma, et al. [9] concluded that frequency of arches (carpal) was more in deaf of both sexes in the hypothenar area. The pattern frequencies of right hand in III inter - digital area of deaf males was statistically higher than normal hearing males. The occurrence of simian crease was higher in the left hands of deaf in both sexes, and ‘mean’ ridge count was less in the deaf as compared to controls.
A. Rashida, et al. [10] found that more number of patients had high category ‘ATD’ angle of the range of 35- 54 degrees whereas control group had lower range of 25- 44 degrees. The ridge count of ‘a-b’ was found increased in right hand of patients.
Desai, Hadimani [11] observed that diabetes mellitus- Type 2, Hypertension patients showed increased arches and loops in number with decreased ulnar loops and whorls in male study groups when compared to controls while females showed increased number of arches, ulnar loops and whorls with decreased number of radial loops than control group for both hands.
Khan, et al. [12] found an increase in the % of arch patterns in the both hands among female and male cases in epilepsy patients when compared to control group & also observed decreased whorl patterns & termination of main line A mostly in sector 5' in males and females.
Bharadwaj, et al. [13] found in their study on obese children that 29% of them showed increase in the ATD angle value and 17% showed presence of additional triradii. 21% had abnormal endings of the main palm lines whereas 11% had reduced C line.
High frequency of arches in left hand and low frequency of ulnar loops in women with cancer cervix was observed by Sofia, et al. [14] wheras Inamdar, et al. [15] found there was significant increase in frequency of whorls & TFRC in both hands & increased frequency of arches in left hand in carcinoma cervix females. They also found the a-t-d angle, t-d ridge count & ulnar loop frequency was decreased in both hands than controls.
Chinmaya, et al. [16] found that frequency of whorl pattern is correlated/ associated with dental carries (a microbial disease). Dental carries was found negative among students with loop pattern & arches.
Singh, et al. [17] found that there was a prominent decrease in the mean value of the arches and increase in the mean value of the ulnar loops in bronchial asthma (BA) patients compared to the control group.
Walker [18] in their study of autistic children found reduced number of whorls and increased number of arches, lowered ridge counts, and less distinctness in formation of ridge line than normal children. Complete absence of transverse crease was also seen. Purvis-Smith and Menser [19] in their evaluation of the dermatoglyphics of acute leukaemia patients found an increased frequency of anomalous palmar creases and variation of digital pattern frequencies from normal children.
Gupta, Karjodkar [20] found an increased frequency of arch and ulnar loop patterns, decreased frequency of simple whorl patterns on fingertips, decrease in frequency of palmar accessory triradii on right and left hands in Oral carcinoma patients. There also found decrease in atd angle on right hand.
In their study Kulic, et al. [21] observed a high percentage of total variance of dermatoglyphics within patients suffering from hypothyreosis.
Ciovîrnache, et al. [22] found lower total digital ridge count, and fewer ridges between the triradii in virilizing polycystic ovary syndrome (VPO) cases. They found VPO women showed more frequency of patterns in the ID space II & higher incidence of palmar transversal variants than normal women.
Ragavan, et al. [23] found a higher c-d ridge count on right hand in polycystic ovary syndrome patients compared to control females. Angle ‘ADT’ was significantly less in PCOS females than control females & males.
An increase in the loop pattern in the hypothenar area was observed in patients with abnormal karyotype by Srivastava, Rajangam [24]. Simian crease and sydney line were also significantly prominent.
In Triradii of the Palm in Idiopathic Epilepsy patients, Ranganath, et al. [25] observed increased frequency of main line index in both hands, decrease in the ‘adt’ angle in the right hand for females. In male patients, there was a significant increase in the ‘dat’ angle in the right hand and decrease in ‘adt’ angle in both the hands.
In seizure disorders patients, an increased main line index on the right palm and decreased a-b ridge counts on both left and right palms was found by Schaumann, et al. [26].
In a study by Lal, Sureka [27] it was found that the dermatoglyphic traits as a-b ridge count, lateral deviation, c-line pattern, palmar pattern and fingertip pattern presented difference in epileptic patients than control group. Epileptic patients showed more mean values of a-b ridge count in left hand, than controls.
Goshi [28] found that ATD angle increased in both right and left hands of combined series of male and female epileptics.
Jindal, et al. [29] found increased tendencies toward whorls in subjects having class II malocclusion and plain arches in those with class III malocclusion. Significant differences in ATD angle and TRC were observed among malocclusion types.
Gustavson, et al. [30] found significant differences in the dermatoglyphic patterns in individuals with Asocial Behaviour compared to normal samples.
In turner syndrome Bhalla, et al. [31] found that mean total finger ridge count , c-d interdigital ridge count in turners remained higher than the normal females. Occurrence of whorls and arches was noticed in right palm of patients in hypothenar region.
Cam, et al. [32] found that dermatoglyphic patterns at the hypothenar area and areas between at the Ist Inter Digial and thenar sites were different in KS patients compared to controls. They also observed significant differences in radial loops and whorls and arches in KS patients to controls.
Rathee, et al. [33] found that male patients with leukemia showed a higher frequency of digital whorls than male control group. Leukemia patients had more sydney palmar flexion creases than control subjects.
Hassanzadeh, et al. [34] found that in Down syndrome, simian line, ulnar loops, whorl, t'', t''' and t' were significant, whereas arch and interdigital III pattern were more indicative of Klinefelter syndrome.
Curro, et al. [35] found in Wilms tumor (WT) patients higher frequency of arches among males, along with the lower proportion of whorls, & lower mean values of TRC and PII than controls.
Wijerathne, et al. [36] found an increased frequency of whorl patterns along with a higher mean total ridge count in hypertensive samples compared to controls.
Annapurna, et al. [37] in their study observed reduced frequency of arches on the finger tips & increased frequency of patterns in the III interdigital area in males and increased frequency of whorls in females along with decreased d-t ridge count in females, and higher incidence of multiple axial triradii in females.
Conclusions
Dermatoglyphics are important tags due to the fact that they develop in the fetus at specific time’s i.e between 3rd and 6th month of fertilization and stay intact till the decomposition of the body after death.
Dermal and palmar ridges are highly useful tools in medical studies both as an initial diagnostic step and later for screening purposes. Of late, much research has been conducted to determine how dermatoglyphics can predict a range of conditions and diseases. The dermatoglyphic analysis is now a valuable guiding factor for diagnosis of some genetic diseases and genetically determined syndromes than in normal people.
It can be determined based on the studies and other reports that there are clear associations between dermatoglyphics and some health/ genetic disorders. Therefore dermatoglyphics may be treated initially as a diagnostic step for suspicious cases. India being a developing country can do with a cost effective tool to predict the possibility of occurrence of ailments in a person and help individuals to be better equipped to manage.
References
-
Ashbaugh DR (1999) Quantitative-Qualitative Friction Ridge Analysis: An Introduction to Basic and Advanced Ridgeology. 1st (Edn.), CRC Press, pp: 248.
-
McRoberts A (2002) The Fingerprint source book. U.S. Department of Justice Office of Justice Programs, Washington DC, USA.
-
Sudha SI (2013) Fingerprints and biometric Analysis. SSB publication, India.
-
Cummins H, Midlo C (1961) Finger prints, palms and soles: an introduction to dermatoglyphics. Dover publications, New York.
-
Gupta CM, Tutakne MA (1986) An evaluation of palmar flexion creases and dermatoglyphics in leprosy. Indian J Lepr 58(2): 263-275.
-
Ciovirnache M, Dumitriu L, Mogos I, Spandonide T, Damian A, et al. (1986) Dermatoglyphics in thyroid cancer. Endocrinologie 24(3): 171-83.
-
Abbasi S, Einollahi N, Dashti N, Vaez-Zadeh F (2006) Study of dermatoglyphic patterns of hands in women with breast cancer. Pakistan journal of medical sciences Online 22(1).
-
Shivaji BS, Laeeque M, Mahajan A, Shilpa NS (2017) Dermatoglyphics in the identification of women either with or at risk for breast cancer. IJBMS 7(5).
-
Anu S, Singh P, Sood V (2007) Palmar And Digital Dermatoglyphics In Congenitally Deaf Subjects. JPAFMAT 7(1).
-
Andani RH, Kubavat D, Malukar O, Nagar SK, Uttekar K, Patel B (2012) Palmar dermatoglyphics in patients of Thalassemia major. Natl J Med Res 2(3): 287-290.
-
Desai SD, Hadimani GA (2013) Dermatoglyphics and Health. Anatomica Karnataka 7(1): 1-9.
-
Khan K, Jethani SL, Rohatgi RK, Goel D, Ali S (2014) Qualitative palmar dermatoglyphics patterns in cases of idiopathic generalised epilepsy. International journal of research in medical sciences 2(2).
-
Bhardwaj N, Bhardwaj P, Tewari V, Siddiqui MS (2015) Dermatoglyphic analysis of fingertip and palmer print patterns of obese children. International journal of medical science and public health 4(7): 946-949.
-
Sofia P, Velichety SD, Chandrasekharan PA, Ravi Prabhu G (2016) Qualitative And Quantitative Analysis Of Digital Dermatoglyphics In Female Reproductive Cancers. Int J Anat Res 4(3): 2603-08.
-
Inamdar Vaishali V, Vaidya SA, Kulkarni P, Devarshi DB, Kulkarni S, Tungikar Sudhir L (2006) Dermatoglyphics In Carcinoma Cervix. J Anat Soc India 55(1): 57-59.
-
Chinmaya BR, Smitha BV, Tandon S, Khurana C (2016) Dermatoglyphics: an indicator of dental carries in humans. Journal of Indian Association of Public Health Dentistry 14 (3): 272-275.
-
Singh S, Khurana AK, Harode HA, Tripathi A, Pakhare A, Chaware P (2016) Study of fingerprint patterns to evaluate the role of dermatoglyphics in early detection of bronchial asthma(BA). J Nat Sci Biol Med 7(1): 43- 46.
-
Harry A Walker (1977) A dermatoglyphic study of autistic patients Journal of autism and childhood schizophrenia 7(1): 11-21. [INLINE_TABLE:4:0]
-
Gupta A, Karjodkar FR (2013) Role of dermatoglyphics as an indicator of precancerous and cancerous lesions of the oral cavity. Contemporary Clinical Dentistry 4(4): 448-453.
-
Kulic JV, Milicic J, Letinic D, Rahelic D, Zekanovic D (2012) Dermatoglyphics in Patients with Hypothyreosis. Coll Antropol 36(2): 389-94.
-
Ciovirnache M, Ioanitiu D, Ionescu B, Dumitrache C, Milea E, Dumitrache M (1986) Dermatoglyphics in the virilizing polycystic ovary syndrome. Endocrinologie 24(2): 87-96.
-
Ragavan S, Kalyanakrishnan S, Elizabeth SK, Sankarasubbaiah R (2019) Palmar dermatoglyphics – a non-invasive screening tool for polycystic ovary syndrome with substantiating evidence from normal males. International journal of scientific research 8(6): 41-43.
-
Meenakshi S, Balasubramanyam V, Sayee Rajangam (2006) Dermatoglyphics in amenorrhea – qualitative analysis. J Obstet Gynecol India 56(3): 250-254.
-
Ranganath P, Rajangam S, Kulkarni RN (2004) Triradii of the Palm in Idiopathic Epilepsy. J Anat Soc India 53(2): 22-24. [INLINE_TABLE:4:1]
-
Nand Lal, Sureka RK (2012) A study of Dermatoglyphic patterns in epileptic patients. J Anat Soc India 61(1): 26-29.
-
Rashmi CG (2018) Study of ATD angle in epileptic patients- A parameter in palmar dermatoglyphics. Indian Journal of Clinical Anatomy and Physiology 5(3): 406-409
-
Jindal G, Pandey RK, Gupta S, Sandhu M (2015) A comparative evaluation of dermatoglyphics in different classes of malocclusion. Saudi Dent J 27(2): 88-92.
-
Gustavson KH, Modrzewska K, Sjoquist KE (1994) Dermatoglyphics in Individuals with Asocial Behaviour. Upsala Journal of Medical Sciences 99(1): 63-67.
-
Bhalla AK, Marwaha RK, Sharma A, Trehan A, Muralidharan R, et al. (2005) Dermatoglyphics in turner syndrome. International Journal of Anthropology 20(1-2): 111.
-
Cam FS, Gul D, Tunca Y, Fıistik, T, Erdogan MO, Yildiz H, Erdem S, Solak M (2008) Analysis of the dermatoglyphics in Turkish patients with Klinefelter’s syndrome. Hereditas 145: 163-166.
-
Rathee R, Kamal N, Kumar A, Vashist M, Yadav R (2014) Dermatoglyphic Patterns of Acute Leukemia Patients. International Research Journal of Biological Sciences 3(6): 90-93.
-
Hassanzadeh Nazarabadi M, Raoofian R, Abutorabi1 R, Hossein HB (2007) Dermatoglyphic Assessment in Down and Klinefelter Syndromes. IJMS 32(2): 105- 109.
-
Curro V, Mastroiacovo P, Castello M, Romagnoli C, Mastrangelo R, et al. (1982) Palmar dermatoglyphics in Wilms’ tumor. Prog Clin Biol Res 84: 385-391. [INLINE_TABLE:5:0]
-
Annapurna V, Ahuja YR, Reddi YR, Reddy GD, Sudhakar Rao V, et al. (1978) Dermatoglyphic studies in rheumatic heart disease. Hum Hered 28(1): 72-78.
- Narcotics and Digital Forensics: Bridging Crimes in the Digital Age
- Ethics in Forensic Psychiatry: Principles, Dilemmas, and Human Rights
- Impact of Acute Stress on Attentional Orienting to Social Cues
- Head Injury and Intracranial Hemorrhage in Western Region of Libya
- A Forensic Study on Handedness: Examination of Handwriting Features in Right and Left Handed Writers
- Techniques for Latent Fingerprint Development Using Natural and Synthetic Powders: A Review