Sudden Death in a Middle-Aged Gentleman
A sudden unexpected death in a healthy individual often leads to panic within a community and it’s frequently associated with malicious mischief. Suicide, infections, genetic or congenital abnormalities may well lead to sudden deaths. All these possibilities are vital in determining the cause of death and facilitate investigation, hence must be considered judiciously. Here, we report a case of a 49-year-old gentleman without underlying medical illness or prior history of heart disease found dead in his home by his wife. Postmortem and histopathology findings determined the cause of death. External examination revealed no obvious injuries whereas 50% narrowing was disclosed in the left anterior descending artery at internal examination. Histology finding showed fibro-fatty replacement of the right ventricle myocardium. Toxicological analyses were unrewarding. It was concluded that the cause of death was arrhythmogenic right ventricular dysplasia. In conclusion, the findings of the forensic autopsy and histopathology facilitated the investigation and established the cause of death. The cause of death attributed to arrhythmogenic right ventricular dysplasia (ARVD). This case demonstrates ARVD can have a late presentation and it should always be borne in mind as a potential cause of death, necessitating this case report.
Introduction
Cardiomyopathy is a disease affecting the myocardium, compromising the contraction of the heart and ultimately leading to heart failure. Arrhythmogenic right ventricular dysplasia (ARVD) is a rare type of cardiomyopathy. It is classified as a rare disease most probably due to under reporting, overlooked or failure to detect. Arrhythmogenic right ventricular dysplasia (ARVD) may present symptoms at any age, but usually arise at a younger age. Nevertheless incidents among older population > 35 years of age have been reported in a few medical literatures. ARVD is currently the second leading cause of sudden cardiac deaths, which accounts for 20% of deaths among population 35 years and younger. This condition is associated with paroxysmal ventricular arrhythmias and is predominantly encountered among males [1].
ARVD affects the desmosomes of the right ventricle myocardium. In addition to providing mechanical strength to tissues, desmosomes are tasked with cell-to-cell adhesions. Abnormalities of these proteins lead to interruption in cell adhesion, especially when under increased mechanical stress or stretch, leading to cell death; progressive loss of myocardium and finally fibro-fatty replacement takes place leaving only the subendocardial layers with normal myocardial tissue [1].
1994 was a momentous year because the World Wide Web was born as well as the diagnostic test for ARVD initially formulated by the International Task Force Criteria for the diagnosis of ARVD which was revised in 2010. [1] A diagnosis of ARVD requires either 2 major criteria or 1 major and 2 minor criteria or 4 minor criteria. In regards to forensic medicine and histopathology the major criteria for ARVD is fibro-fatty replacement of the myocardium [2].
Case Report
A 49-year-old gentleman without underlying medical illness or prior history of heart disease was found dead on his couch by his wife. A post mortem examination was performed within 24 h. The deceased was medium built. Bilateral conjunctiva was congested but no petechial haemorrhages seen. No discernible defensive wound or obvious external injuries.
Heart weighed 345g with 50% narrowing detected in the left anterior descending artery. The myocardium and valves were grossly normal (Figure 1). The left ventricle wall thickness measured 1.7cm, interventricular septum was 0.8cm whereas the right ventricle wall was 0.3cm. Tricuspid valve measured 11.8cm; pulmonary valve was 5.8cm whereas aortic valve and mitral valve measured 6.2cm and 10.2cm respectively. Bilateral lung were edematous. The liver was enlarged weighing 2350gm with nutmeg appearance on cut section. The stomach contained 50mls of brownish digested food content.

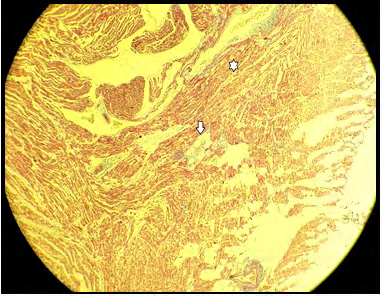
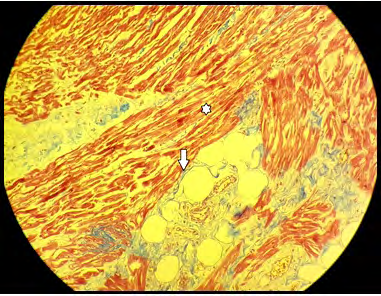
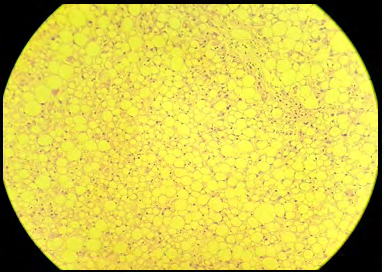
Histopathology findings revealed fibro-fatty replacement on the myocardium of the right ventricle, viewed using Masson’s trichrome stain (Figures 2 & 3) and the hepatic cells demonstrated hepatic macro vesicular steatosis (Figure 4).
Toxicological analyses were unrewarding. Otherwise no other significant pathologies were detected. It was concluded that the cause of death was arrhythmogenic right ventricular dysplasia.
Discussion
This case study concurs that ARVD may well occur among older population. As mentioned previously strenuous activities can further add insult to the existing anomalies in the desmosomes, however this case demonstrates the opposite given that the disease occurred in a previously healthy gentleman at rest. Right ventricle myocardium involvement leads to right ventricular dysfunction subsequently causing ventricular tachycardia, isolated right heart failure and sudden deaths. ARVD may also be non-genetic in origin; congenital abnormalities affecting the right ventricle, myocarditis or viral being potential biases [3, 4]. Furthermore, it is important to differentiate ARVD from other right heart diseases which distinctively affect the right ventricle for instance brugada syndrome [5].
All laboratory investigations for infection and toxicology were negative in this case report. With regard to histopathology, fibro-fatty replacement of the right ventricular myocardium and right ventricular part of the interventricular septum is the chief characteristic of the disease akin to findings in this case study.
Conclusion
The findings of the forensic autopsy and histopathology facilitated the investigation and established the cause of death. This case demonstrates ARVD can have a late presentation and it should always be borne in mind as a potential cause of death, necessitating this case report.
References
-
Li KHC, Bazoukis G, Liu T, Li G, Wu WKK, et al. (2017) Arrhythmogenic right ventricular cardiomyopathy/ dysplasia (ARVC/D) in clinical practice. J Arrhythmia 34(1): 11-22.
-
Papaioannou GI, Apostolopoulos T, Stambola S, Zilidis A, Gialafos J (2009) Late presentation of arrhythmogenic right ventricular cardiomyopathy: a case report. J Med Case Reports 3:7235.
-
Morentin B, Aguilera B, Garamendi PM, Suarez-Mier MP (2000) Sudden unexpected non-violent death between 1 and 19 years in north Spain. Arch Dis Child 82(6): 456- 461.
-
Fontaine G, Fontaliran F, Hebert JL (1999) Arrhythmogenic right ventricular dysplasia. Annu Rev Med 50: 17-35.
-
Altun I, Akin F, Sahin C, Halil Beydilli (2014) An ECG changed the life of a young boy: a case of arrhythmogenic right ventricular dysplasia. BMJ Case Reports 2014.
- Narcotics and Digital Forensics: Bridging Crimes in the Digital Age
- Ethics in Forensic Psychiatry: Principles, Dilemmas, and Human Rights
- Impact of Acute Stress on Attentional Orienting to Social Cues
- Head Injury and Intracranial Hemorrhage in Western Region of Libya
- A Forensic Study on Handedness: Examination of Handwriting Features in Right and Left Handed Writers
- Techniques for Latent Fingerprint Development Using Natural and Synthetic Powders: A Review