Suicide Mortality in Benghazi City
Back ground: It is estimated that over 800 000 people die by suicide and that there are many suicide attempts for each death. The impact on families, friends and communities is devastating. Aim of the study: This study was conducted to describe the suicidal deaths in Benghazi City, Libya. Methodology: Data were collected from the cases of suicidal deaths admitted to Aljala hospital (accident hospital in the city) in a 5-year period (A retrospective study)from 2011 to 2015. The cases were grouped according to age number of subjects every year, methods of suicide. All data were statistically analyzed. Findings and Conclusion: The total number of cases was 108 cases, the majority was males. hanging was the most common method of suicide in both sexes, especially in middle age group. The current study focused on the methods and aspects of suicidal deaths in “Benghazi City”, which may help in prevention and treatment of this problem, accordingly. We recommended psychological assessment and support for chronic illnesses’ patients for early monitoring of committing suicide tendency
Introduction
Benghazi is the second largest city in Libya and the main city (or capital) of the Cyrenaica region (or ex-Province), located in the North of Africa. Benghazi is located half way between Tripoli in the West (a distance of approximately 1000 km between these cities) and Cairo in the East (also approximately 1000 km). Benghazi city population is approximately 1 million. Majority of the population in are Libyans, with a very low number of foreigners.
Because Libya is an Islamic country (Muslims represent 100% of the total population), It is considered to be a criminal act onto the self. Suicide is one of the leading causes of death worldwide and an important public health problem [1, 2]. It is the third leading cause of death among young people in the United States [3].
Aim of the study
The aim of the current study is to describe the extent of the suicide mortality in the city of Benghazi, and to set an initial starting point for further researches all over the country.
Methodology
The total number of cases of the present work was 108 deceased persons due to suicidal acts (55 males and 53 females). They were examined at the Ministry of Justice Forensic Medicine Administration in Benghazi city, Libya, between January 2011 and December 2015. Cases were determined to be suicidal according to many items including general prosecutor’s investigations, external examination, autopsy findings and the final reports from the medicolegal examiners in charge of these cases. As regards the age of the studied persons, they were grouped and all data were statistically analysed (Tables 1-5 & Figures 1-4).
Results
| Frequency | Percentage | |
|---|---|---|
| 0-14 | 10 | 9.7% |
| 15-19 | 19 | 17.4% |
| 20-24 | 19 | 17.4% |
| 25-29 | 18 | 16.5% |
| 30-34 | 3 | 2.7% |
| 35-39 | 9 | 8.2% |
| 40-44 | 12 | 11% |
| 45-49 | 6 | 5.5% |
| 50-54 | 6 | 5.5% |
| 55-59 | 1 | 0.9% |
| 60+ | 7 | 6.4% |
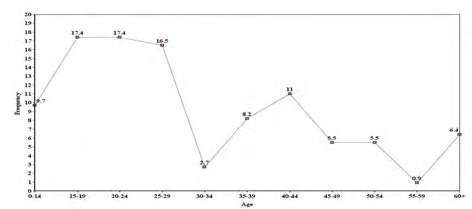
Table 2: Age and frequency of suicidal deaths (overall).
| Frequency | Percentage | ||
|---|---|---|---|
| 0-14 | 5 | 9.40% | |
| 15-19 | 16 | 30.10% | |
| 20-24 | 8 | 15.09% | |
| 25-29 | 4 | 7.50% | |
| 30-34 | 1 | 1.80% | |
| 35-39 | 7 | 13.20% | |
| 40-44 | 0 | 0% | |
| 45-49 | 4 | 7.50% | |
| 50-54 | 4 | 7.50% | |
| 55-59 | 1 | 1.80% | |
| 60+ | 3 | 5.60% |
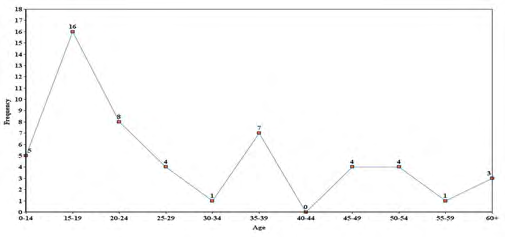
Table 4: Age and frequency of suicidal deaths (Female).
| Cause of Death | Frequency | Percentage |
|---|---|---|
| Hanging | 38 | 34.8% |
| Drug | 14 | 12.8% |
| Burn | 15 | 13.7% |
| Unknown | 19 | 17.3% |
| Gunshot | 9 | 8.2% |
| Foreign | 3 | 2.7% |
| Stabbing | 6 | 5.5% |
| Scalding | 1 | 0.9% |
| Cut Wound | 1 | 0.9% |
| Drowning | 1 | 0.9% |
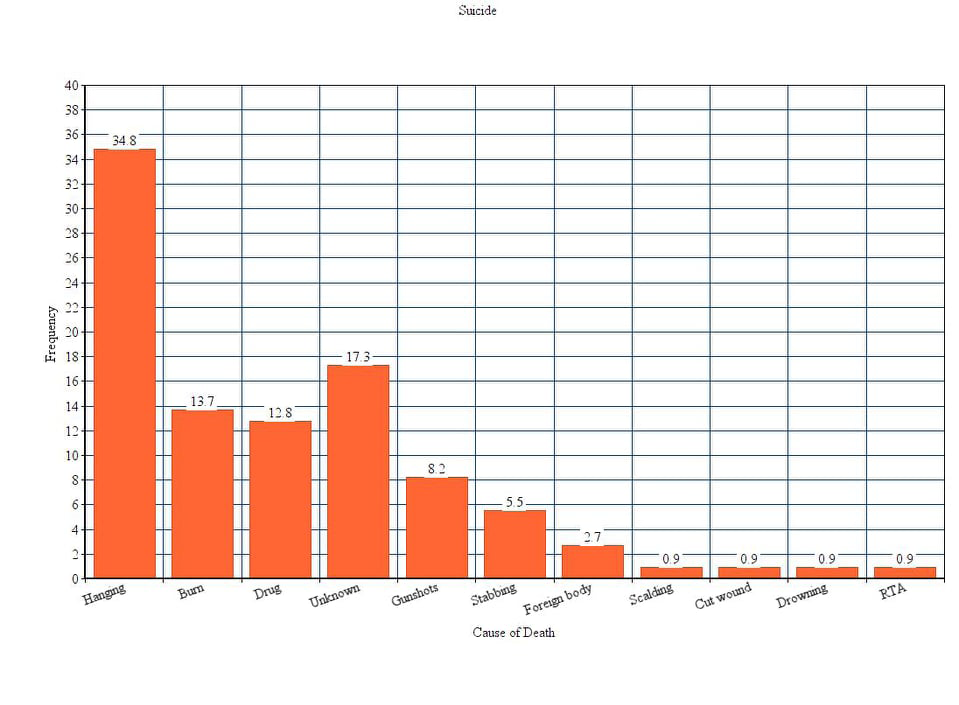
Table 1: Suicide (cause of death in detail).
| Cause of Death | Frequency | Percentage | |
|---|---|---|---|
| 0-14 | 10 | 9.7% | |
| 15-19 | 19 | 17.4% | |
| 20-24 | 19 | 17.4% | |
| 25-29 | 18 | 16.5% | |
| 30-34 | 3 | 2.7% | |
| 35-39 | 9 | 8.2% | |
| 40-44 | 12 | 11% | |
| 45-49 | 6 | 5.5% | |
| 50-54 | 6 | 5.5% | |
| 55-59 | 1 | 0.9% | |
| 60+ | 7 | 6.4% |
Table 3: Sex and cause of death (female).
| Cause of Death | Frequency | Percentage | |
|---|---|---|---|
| 0-14 | 5 | 9.40% | |
| 15-19 | 16 | 30.10% | |
| 20-24 | 8 | 15.09% | |
| 25-29 | 4 | 7.50% | |
| 30-34 | 1 | 1.80% | |
| 35-39 | 7 | 13.20% | |
| 40-44 | 0 | 0% | |
| 45-49 | 4 | 7.50% | |
| 50-54 | 4 | 7.50% | |
| 55-59 | 1 | 1.80% | |
| 60+ | 3 | 5.60% |
Table 5: Sex and cause of death (male).
Discussion
In the Current Study, Age and Frequency of Suicidal Deaths (Overall) as Follow
Age group from 0-14 was 10%, age group from 15-19 was 19%, age group from 20-24 was 19, age group from 25- 29 was 18%, age group from 30-34 was 3%, age group from 35-39 was 9%, age group from 40-44 was 12%, age groups from 45-54 was 6%, 55-59 was 1% and above 60 was 7%.
Age and Frequency of Suicidal Deaths (Female)
Age group from 0-14 was 5 out of 41 females (9.4%), age group from 15-19: was 16(30.1%), age group from 20- 24: was 8(15.09%), age group from 25-29: was 4(7.5%), age group from 30-34: was 1(1.8%), age group from 35-39: was 7(13.2%), age group from 40-44: was 0(0%), age group from 45-49: was 4(7.5%), age group from 50-54: was 4(7.5%), age group from 55-59: was 1(1.8%) and above 60: was 3(5.6%).
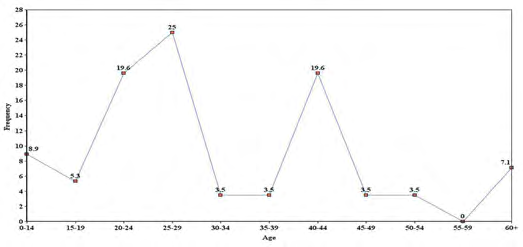
Age and Frequency of Suicidal Deaths (male)
0-14- was 9%, 15-19 was 5%, 20-24 was 19%, 25-29 was 25%, 30-34 and 34-39-were 3%. 40-44-was 9%, 45-49 and 49-54 were 3%, 55-59 was 0% and above 60 was 7%.
Suicide (cause of death in detail)
Hanging: 38(34.8%), Drug:14 (12.8%), Burn:15 (13.7%), Unknown: 19 (17.3%), Gunshot: 9 (8.2%), Foreign body: 3(2.7%), Stabbing: 6(5.5%), Scalding: 1(0.9%), Cut wound: 1(0.9%), Drowning: 1(0.9%).
Sex and Cause of Death (female)
Hanging: 21(38.8%), Drug: 9(16.6%), Burn: 7 (12.9%), Unknown: 10 (18.5%), Gunshot:1(1.9%), Foreign body: 1(1.9%), Stabbing: 4(7.5%), Scalding: 0(0.%), Cut wound: 0(0%), Drowning: 1(1.9%).
Sex and Cause of Death (male)
Hanging: 17(30.3%), Drug: 5(9%), Burn: 8 (14.2%), Unknown: 9 (16%), Gunshot: 8(14%), Foreign body: 2(3.5%), Stabbing: 4(7%), Scalding: 1(2%), Cut wound: 1(2%).
This rate was not close to the lowest rates reported for men in the high income countries of the Eastern Mediterranean and also the low and middle income countries of the Americas [3, 4, 5, 6, 7]. On the other hand, the lower rate of suicide in Libya could be attributed to the Islamic law or doctrine in which suicide is condemned and is considered to be a criminal act onto the self.
We think that this might have a role in preventing many vulnerable individuals from committing these acts. The relatively low average suicide rate was also studied in another Islamic country, Saudi Arabia, and was 1.1/100,000 population per annum according to a study in 2005 [8]. Another study in Dammam, the second largest city in Saudi Arabia, there was an outstandingly decrease in suicide rate in this city from 2.55/100,000 population in 2003 to 1.15/100,000 population in 2007 [9].
The gender ratio (male:female) in the overall period of study was 1.1, These rates are considered to be different from the global rates. It is much differ from another study performed in the main Turkish city “Istanbul”, they reported a male to female ratio of 2.39,9 nd another study done in South India with a male: female ratio (2:1) [10].
The highest number of cases of both gender were in the middle age group, These results were concomitant with other studies in Malaysia [11] and Turkey [9] and South India [10] appearing that the third decade had the maximum number of suicidal cases.
In the current study, hanging was the most common method of suicide in both sexes, and represented 34% of the total suicidal deaths specially in middle age group. Hanging could be attributed partly because the tools to do it are so readily available.
The second common method was burning, poisoning, drowning, firearms, and stabbing. These results were in agreement with other studies in many other countries as hanging is a leading method of suicide in Germany and Japan and it is the second leading suicide method after intoxications in India [12, 13, 14]. In US, despite the fact that the suicide patterns differ according to the states, hanging was reported to be the second leading method of suicide after firearms in general [15].
In a similar middle-east city, in Dammam, two different studies affirmed that firearms, self-burning and falling from height were the next most common methods of suicide after hanging [16, 17].
Conclusion and Recommendations
Suicide rate in Benghazi city is much lower than other rates worldwide. However, it is still considered a public health problem and should be given high priority with regard to prevention. We recommend more detailed studies across Libya for evaluation and further assessment. Moreover, similar studies should be done concurrently for both suicide deaths and attempted suicide as well. We also recommend testing the psychological tendency for committing suicide.
References
-
Sharma BR, Gupta M, Sharma AK, Sharma S, Gupta N, et al. (2006) Suicides in Northern India: comparison of trends and review of literature. J Clin Forensic Med 14(6): 318-326.
-
Murray CJL, Lopez AD (1996) The global burden of disease: a comparison assessment of mortality and disability from diseases, injuries, and risk factors in 1990 and projected to 2020. Harvard School of Public Health.
-
Krug E, Dahlberg L, Mercy J, Zwi A, Lozano R (2002) World report on violence and health. World Health Organization.
-
WHO (1999) Figures and facts about suicide. World Health Organization.
-
Yip PS (1996) Suicide in Hong Kong, Taiwan and Beijing. Br J Psychiatr 169(4): 495-500.
-
Peden M, McGee K, Sharma G (2002) The injury chart book: a graphical review of the global burden of injuries. World Health Organization.
-
Reza A, Mercy JA, Krug E (2001) Epidemiology of violent deaths in the world. Inj Prev 7(2): 104-111.
-
Elfawal MA (1999) Cultural influence on the incidence and choice of method of suicide in Saudi Arabia Am J Forensic Med Pathol 20(2): 163-168.
-
Uzün I, Büyük Y, Gürpinar K (2007) Suicidal hanging: fatalities in Istanbul retrospective analysis of 761 autopsy cases. J Forensic Leg Med 14(7): 406-409.
-
Kanchan T, Menezes RG (2008) Suicidal hanging in Manipal, South India – victim profile and gender differences J Forensic Leg Med 15(8): 493-496.
-
Murty OP, Cheh LB, Bakit PA, Hui FJ, Ibrahim ZB, et al. (2008) Suicide and Ethnicity in Malaysia. Am J Forensic Med Pathol 29(1): 19-22.
-
Ojima T, Nakamura Y, Detels R (2004) Comparative study about methods of suicide between Japan and the United States. J Epidemiol 14(6): 187-92.
-
Joseph A, Abrajam S, Muliyil JP, Prasad J, Minz S, et al. (2003) Evaluation of suicide rates in rural India using verbal autopsies, 1994–1999. BMJ 326(7399): 1121- 1122.
-
Wiesner G (2004) Suicidal methods: a comparison between East and West Germany. Epidemiological, forensic and sociomedical aspects. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz 47(11): 1095-1106.
-
Shields LB, Hunsaker DM, Hunsaker JC (2005) Suicide: a ten-year retrospective review of Kentucky medical examiner cases. J Forensic Sci 50(3): 613-617.
-
Al OM Madni, Kharosha MA, Zaki MK, Murty OP (2010) Trends of suicide in Dammam Kingdom of Saudi Arabia. J Forensic Med Toxicol 27(2): 56-60.
-
Al Madni OM, Kharoshah MA, Zaki MK, Ghaleb SS (2010) Hanging deaths in Dammam, Kingdom of Saudi Arabia. J Forensic Legal Medicine 17(5): 265-268.
- Forensic Implications of Adverse Drug Reactions in Schizophrenia A Case Series
- Narcotics and Digital Forensics: Bridging Crimes in the Digital Age
- Ethics in Forensic Psychiatry: Principles, Dilemmas, and Human Rights
- Impact of Acute Stress on Attentional Orienting to Social Cues
- Head Injury and Intracranial Hemorrhage in Western Region of Libya
- A Forensic Study on Handedness: Examination of Handwriting Features in Right and Left Handed Writers