Individual Tolerance to Acute Ethanol Intoxication
Relevance: In order to figure out the cause of death and present the evidences to the court, law enforcement authorities instructed forensic medicine experts to carried out differential diagnosis, by using the posthumous exogenous alcoholemia to differentiated between the severity of acute ethanol intoxication, and death caused by alcohol poisoning. However, the experts are difficult to carried out the assessment to determine the severity of alcohol intoxication, even using the following criteria: exogenous alcoholemia level, signs of conditionally fatal ethanol poisoning with trauma. There are differences in the ethanoloxidizing dehydrogenase enzymatic activity, make it easier to determine individual ethanol tolerance, which can be used for forensic medical substantiation to determine severity of acute alcohol intoxication and fatal ethanol poisoning. Purpose of the Study: We carried out the research by evaluating the severity of the acute alcohol intoxication, by taking into account the blood ethanol concentration level and the death caused by the fatal ethanol poisoning; we use the 2 indicators of the ethanol- oxidizing enzymatic activity, which are the alcohol dehydrogenase in liver, and acetaldehyde dehydrogenase in the brain. Material and Methods: Forensic medical experts using 72 corpses to carried out the research, we had identified ethanoloxidizing enzymatic activities in the brain stem and liver and divided into 3 observation groups : Group I – death from fatal ethanol poisoning (FEP) with blood ethanol concentration between the range from 3.0 to 5.3 g/L (22 cases); Group II – death caused by car accidents as the drivers who are having severe ethanol intoxication with vehicle’s mechanical damage, the blood ethanol concentration between the range from 3.0 to 4.8 g/L (25 cases); Group III (controlled group) – death caused by car accidents with vehicle’s mechanical damage without exogenous alcoholemia (25 cases). Results: In the fatal ethanol poisoning group, we compared with the controlled group, there are decrease in enzymatic activities, and there were significant statistically decreases (P<0.05). When comparing these enzymatic activities between IInd and IIIrd group , there were no significant statistically differences (P>0.05). Conclusion: We used the following criteria and indicators to determine the fatal ethanol poisoning: alcohol dehydrogenase (ADH) enzymatic activity is between the range 2.60 - 3.44 c.u.; aldehyde dehydrogenase (ALDH) enzymatic activity is between the range 1.47 - 1.98 c.u.; blood ethanol concentration is between the range from 3.0 to 5.3 g/L. In group I , due to the excessive ethanol amount and the newly formed acetaldehyde, so there are inhibition of alcohol dehydrogenase (ADH) and aldehyde dehydrogenase (ALDH) enzymatic activities. When group II comparing with controlled group, the ethanol-oxidizing enzymatic activities are approximately at the same level. This phenomena can be explained that the individuals have high ethanol tolerance. To determine the individual high ethanol tolerance, using the following criteria: the alcohol dehydrogenase (ADH) enzymatic activity in the liver between the range 3.97 - 4.79 c.u.; aldehyde dehydrogenase (ALDH) enzymatic activity in the brain between the range from 2.29 to 2.89 c.u.; the blood ethanol concentration of the corpse is between the range from 3.0 to 4.8 g/L.
Introduction
Relevance
The forensic medical experts using the gas chromatographic analysis, the blood ethanol concentration in the corpses, in order to determine the acute ethanol intoxication. In order to confirm the diagnosis of the post- mortem alcoholemia level, the blood alcohol concentration (BAC) in living people should be taken into account, to further determine the degree of alcohol intoxication. The degrees of acute ethanol intoxication are distinguished using the following criteria: light (0.5-1.5 g/L), medium (1.5-2.5 g/L), strong (2.5-3.0 g/L), heavy (3.0-5.0 g/L). The blood ethanol concentration in the corpse between the range from 3.0 to 5.0g/L, which corresponds to severe ethanol intoxication with increased risk of adverse effects, and blood ethanol concentration is above 5.0g/L, which are considered conditionally fatal ethanol poisoning. We used the alcohol dehydrogenase and acetaldehyde dehydrogenase enzymes as indicators, which characterized the individual exogenous ethanol tolerance and sensitivity to carried out the differential diagnosis between the severe ethanol intoxication and fatal ethanol poisoning [1, 2, 3].
In the human body, most of the incorporated ethanol is absorbed in the jejunum. Resorption rate increases with empty stomach, and accelerated resorption rate, while drinking with 20% carbonated alcoholic beverages. Low polarization accelerated ethanol molecules entering into the blood, easy penetration of ethanol molecules through cell membranes and their rapid distribution between blood and tissues. Ethanol, barbiturates, and benzodiazepines, they are all freely crossing blood-brain barrier molecules and can cause similar clinical effects. Up to 10 percent ethanol is excreted with exhaled air, sweat and urine. The bulk of exogenous ethanol undergoes enzymatic degradation in the liver by the alcohol dehydrogenase enzyme (ADH). In general, around 7 to 10 grams of ethanol can be oxidized in an hour. Ethanol undergoes oxidation with the alcohol dehydrogenase enzymatic activity, and the acetaldehyde is formed. Acetaldehyde is highly reactive due to its carbonyl group, and are toxic towards the mitochondria and cytosol of internal organs. Acetaldehyde is metabolized by the aldehyde dehydrogenase (ALDH) enzymes. According to the literature, the content of acetaldehyde in the venous blood of the portal vein is between the range from 2 to 20 µmol/ ml [3, 4]. Minor pathways of catabolic oxidation of exogenous ethanol, with the participation of microsomal and catalase. Ethanol-oxidation systems, ensure there is no more than 10% of its amount is being converted. On the other hand, in order to understand the chronic alcohol intoxication, it is very important that we must first understand the processes of ethanol-oxidation enzymatic activity [5, 6, 7, 8].
Forensic medical experts have shown the blood alcohol concentration, cannot act as indicators, to confirm severity of ethanol intoxication and poisoning.
As we have cases when lethal ethanol concentration were found in the blood of drivers, who died from car accidents, but not from ethanol intoxication. Additional criteria are required to characterized individual exogenous ethanol tolerance. In order to have the specific indicators to further confirm the diagnosis of individual ethanol tolerance, we proposed to carried out the research on the ethanol- oxidizing enzymes: alcohol dehydrogenase (ADH) in the liver and acetaldehyde dehydrogenase (ALDH) in the brain stem. These enzymes are responsible for the nodal links of ethanol oxidative conversion, and can serve as important indicators to carry out the differential diagnosis between the fatal ethanol poisoning, severe alcohol intoxication, and rule out the other causes of death.
Purpose of the Study
In order to confirm the forensic evaluation on the severity of acute alcohol intoxication, by taking into account the blood ethanol concentration, and the further understanding of the fatal ethanol poisoning, and then carrying out the research on the ethanol-oxidizing enzymatic activities in the brain and liver tissues.
Material and Methods
Forensic medical experts using 72 corpses to carry out the research, by identifying the alcohol dehydrogenase (ADH) enzymatic activity in the liver hepatocytes tissues, and acetaldehyde dehydrogenase(ALDH)enzymatic activity in the brain stem. We had divided into 3 observation groups: Group I: fatal ethanol poisoning with the blood ethanol concentration between the range from 3.0 to 5.3g/L-22 cases; Group II: death caused by car accidents with drivers who are severe ethanol intoxication with vehicle's mechanical damage, having blood ethanol concentration between the range 3.0-4.8 g/L (25 cases); Group III (controlled group) – death caused by car accidents with vehicle’s mechanical damage without exogenous alcoholemia (25 cases).
The following observation parameters were used in the research: gender, age and blood ethanol concentration are determined by using the gas chromatographic study; alcohol dehydrogenase (ADH) histochemical enzymatic activity in the liver and acetaldehyde dehydrogenase (ALDH) histochemical enzymatic activity in the brain stem neurons. The results were entered into the database, analysis were carried out with grouping, comparison and statistical calculating the significant differences between the observation groups.
In histological preparations, the alcohol dehydrogenase (ADH) histochemical activity (Alcohol: NAD+ - oxidoreductase, EC 1.1.1.1) were identified in the liver tissue by using the E. Pearse method (1972); the acetaldehyde dehydrogenase (ALDH) activity (Acetaldehyde: NAD+ - oxidoreductase, EC 1.2.1.3) in brain stem neurons were identified by the S. M. Zimatkin method (1985) (Figures 1A, 1B).
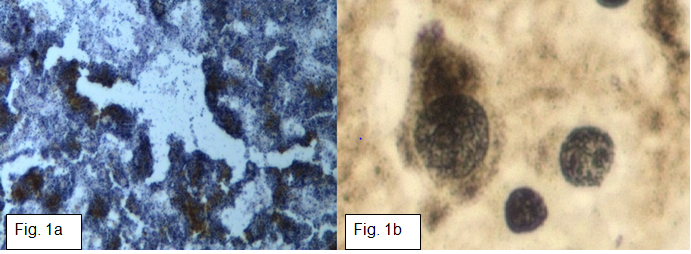
Figure 1a: ADH activity in liver hepatocytes E. Pearce Method Magnification 400. Figure 1b: ALDH activity in brain stem neurons S. Zimatkin Method Magnification 600.
When we are doing research, started by preparing the histopathological slides, according to the traditional routine, as we used fixation method, dehydration, clarification, and dewaxed liver and brain tissues of histological slides, we cut into 10 micrometer thick, and incubated in pyrophosphate buffer (pH 7.4) with the presence of substrates (ethanol for alcohol dehydrogenase (ADH) and acetaldehyde for aldehyde dehydrogenase (ALDH)), coenzyme nicotinamide adenine dinucleotide (NAD+) , and specific dye nitro blue tetrazolium (NBT). In order to understand the enzymatic reaction in dark blue formazan, we have to identified and determined the amount of enzymatic activities in histopathological slides of brain and liver tissues. The histopathological slides were enclosed in polystyrene, examined in the transmitted light microscope, at the magnification of 400 or 600. Using the computer image analysis system (cellSens®, Olympus, Japan) to measured the parameters and recorded in the database. Additionally, frozen sections were prepared using the Julabo CF30 Cryostat (GmbH, Germany). The ethanol-oxidizing enzymatic activities, were equally identified between the cryostat section and paraffin sections of histological materials. Within all of the histological preparations slides of brain and liver tissues, at least 7 manifestations fields with histochemical reactions, in the form of formazan granules were examined, which were measured and calculated in conditional units (c.u.).
Statistical Studies were carried out, using the statistica software package Version 10 (StatSoft®, Inc. 2011, http:// www.statsoft.com). Nonparametric comparisons between observation groups were used for statistical analysis of the researched parameters. We obtained different indicators, assessed and measured by using semi- quantitative measurements.
In all observation groups, forensic medical examiners have given the conclusion, that the laboratory studies have performed variety researches, for example, histological, chemical, biochemical, -excluding the presence of other agents causing intoxication, and pathomorphological changes that could affect confirmation the cause of death. The presented research were approved by the Ethics Committee of Sechenov University and complies with the Ethical Standard Declaration of 1989 (Helsinki).
Research Results
The individuals have been distributed between gender and age in observation groups are presented in (Table 1).
| Gender/Age | Observation Group / Quantity / n | ||
|---|---|---|---|
| Ist Group Fatal Ethanol Poisoning n - 22 | IInd Group Car accidents with severe alcohol intoxication n- 25 | IIIrd Group(Control) Car accidents without alcoholemia n- 25 | |
| Male | 13 | 21 | 15 |
| Female | 9 | 4 | 10 |
| 17-30 years old | 4 | 5 | 6 |
| 31-45 years old | 9 | 6 | 7 |
| 46-60 years old | 6 | 11 | 5 |
| 61-75 years old | 3 | 3 | 7 |
Table 1: Distribution of observations by gender and age.
The predominant age of individuals with blood ethanol concentration, between the range of 30 - 60 years. The controlled group have an even distribution of individuals, between gender and age.
The frequency of identification the severe ethanol intoxication in men are 2-5 times higher than in women. The number of individuals with high ethanol concentration is given in (Table 2).
| Levels of Ethanolemia | Observation groups | |
|---|---|---|
| ( g / L ) | 1st Group: Fatal ethanol poisoning n - 22 | 2nd Group: Fatal injury with high ethanolemia level n - 25 |
| 3,0–3,5 | - | 6 |
| 3,6 – 4,0 | 6 | 7 |
| 4,1 – 4,5 | 11 | 7 |
| 4,6 – 5,0 | 3 | 4 |
| 5,1 – 5,5 | 2 | 1 |
Table 2: The observations with high alcoholemia level.
In general, (50%, half of the 22 observation individuals) blood ethanol concentration in corpses were detected between the range from 4.1 to 5.5 g/L. The two important indicators for fatal ethanol poisoning are the following : alcohol dehydrogenase (ADH) and aldehyde dehydrogenase (ALDH) enzymatic activities, when comparing the enzymatic activities between the fatal ethanol poisoning group and controlled group, we can see there are decrease in enzymatic activities, compared to the controlled group; there were significant statistically differences (P < 0.05).
There is absence of enzymatic activity differences between the group II (trauma without ethanolemia), and group III ( controlled group), ( P>0.05). The ranges of enzymatic activities compared with the injuries indices partially coincided.
Mean values and range of variations between alcohol dehydrogenase (ADH) and aldehyde dehydrogenase (ALDH) enzymatic activities are shown in (Table 3).
- Enzyme activity (c.u.) Mean values & Range of variations
- Group I Fatal poisoning& high ethanolemia
- Group II Trauma & high ethanolemia
- Group III Trauma & absent ethanolemia
- ADH
- 3.10±0.34 2.60–3.44
- 4.38±0.25 3.97–4.79
- 4.05±0.38 3.71–4.69
- ALDH
- 1.62±0.22 1.47–1.98
- 2.52±0.23 2.29–2.89
- 2.12±0.22 1.98–2.41
Table 3: Mean values and range variations of ADH and ALDH activities.
Discussion of the Research Results
In order for the forensic medical experts to carried out the assessment about the severity of acute alcohol intoxication.
We had researched about the alcohol dehydrogenase (ADH) and aldehyde dehydrogenase (ALDH) enzymatic activities. In the group I, bringing all the cases together with fatal ethanol poisoning. The following indicators have given us, the results that have proven the previous published data, that due to excess amount of incorporated ethanol and newly formed acetaldehyde has caused reduced in the alcohol dehydrogenase (ADH) and aldehyde dehydrogenase (ALDH) enzymatic activities. Alcohol dehydrogenase (ADH) enzymatic activity in the liver reduced by 25.5% , the aldehyde dehydrogenase (ALDH) enzymatic activity in the brain stem reduced by 13.6%, blood ethanol concentration between the range from 3.0 to 5.3g/l [9, 10].
We had done research separately, between car accidents cases , and death cases due to lethal ethanol concentration in the blood. This phenomenon told us that the individuals have the ability to maintain active, mental and physical health, even though having the high blood ethanol tolerance as it was written in the literature [11, 12].
In this group with signs and symptoms of high ethanol tolerance, we found: alcohol dehydrogenase (ADH) activity in the liver were determined between the range from 3.97 to 4.79 с.u., aldehyde dehydrogenase (ALDH) activity in brainstem neurons between the range from 2.29 to 2.89 с.u.; blood ethanol concentration between the range from 3.0 to 4.8 g/L.
Thus, signs showing the high individual ethanol tolerance, which reduces the risk of death due to acute ethanol intoxication, even though with high blood ethanol concentration [13, 14]. The data of this study can be used for forensic evaluation of acute alcohol intoxication, and substantiation the causes of death in thanatology and toxicology.
The general theoretical significance of our results are to confirm the possibilities of postmortem forensic analysis, to determine the ethanol-oxidizing enzymatic activities. It is noteworthy that in the first 2 hours after death, there are total inactivation of enzymes, mainly due to the blockade and inhibition of enzymatic reactions, which are caused by lack of energy. At the same time, losing their functionality, even though the enzymes remain structurally intact. First of all, it should be noted that the ethanol oxidation enzymatic activity, acetaldehyde with the participation of alcohol dehydrogenase (ADH)and aldehyde dehydrogenase (ALDH) are energy-consuming; therefore, when carrying out histochemical research on enzymes, oxidized NAD + is additionally introduced into the incubation medium, which is capable of releasing H + ions to activate the blocked histochemical reaction [15, 16]. In our histochemical studies, as well as in the previously works performed by other authors, the residual of alcohol dehydrogenase (ADH) and aldehyde dehydrogenase (ALDH) enzymatic activities in the liver tissue and brain tissues were identified during the first few days after death [17, 18, 19].
Forensic medical experts are often being questioned about what are the possibilities to carried out the assessment, in order to confirm the status of alcohol intoxication. And according to the result, the forensic medical experts had come to the conclusion, that the blood ethanol concentration are the indicator to be characterized for the alcohol intoxication. It is known that low ethanol concentration has psychostimulating effect [20, 21]. The severity of alcohol intoxication, depends on the incorporated ethanol and the functionality of ethanol-oxidizing systems. Usually, severe degree of acute ethanol intoxication are accompanied by impaired consciousness, coma, and loss of the ability to carry out meaningful actions [22, 23]. At the same time, individuals with increased ethanol tolerance are able to perform active actions, even with conditionally lethal blood ethanol concentration.
Conclusion
Postmortem alcohol dehydrogenase (ADH) enzymatic activity in the liver tissues and aldehyde dehydrogenase (ALDH) enzymatic activity in the brain stem are being proven, as additional forensic indicators to determine the severity of ethanol intoxication.
Fatal ethanol poisoning is characterized by combination of blood ethanol concentration between the range from 3.0 to 5.3 g/L, alcohol dehydrogenase (ADH) activity between the range from 2.60 to 3.44 c.u.; aldehyde dehydrogenase (ALDH) activity between the range from 1.47 to 1.98 c.u.;
Individual high ethanol tolerance is characterized by combination of blood ethanol concentration between the range from 3.0 to 4.8 g/L, alcohol dehydrogenase (ADH) activity between the range from 3.97 to 4.79 c.u., aldehyde dehydrogenase (ALDH) activity between the range from 2.29 to 2.89.
Conflict of Interest
The author declares no conflicts of interest.
Financing: The study was not sponsored.
References
-
O’Dean SM, Mewton L, Chung T, Clay P, Clare PJ, et al. (2022) Definition matters: assessment of tolerance to the effects of alcohol in a prospective cohort study of emerging adults. Addiction 117(11): 2955-2964.
-
Wang H, Xu H, Li W, Li B, Shi Q, et al. (2019) Forensic appraisal of death due to acute alcohol poisoning: three case reports and a literature review. Forensic Sci Res 5(4): 341-347.
-
Kriikku P, Ojanpera I (2020) Significant decrease in the rate of fatal alcohol poisonings in Finland validated by blood alcohol concentration statistics. Drug Alcohol Depend 206: 107722.
-
Hoover DJ, Brien JF (1981) Acetaldehyde concentration in rat blood and brain during the calcium carbimide- ethanol interaction. Can J Physiol Pharmacol 59(1): 65- 70.
-
Nuutinen HU, Salaspuro MP, Valle M, Lindros KO (1984) Blood acetaldehyde concentration gradient between hepatic and antecubital venous blood in ethanol- intoxicated alcoholics and controls. Comparative Study Eur J ClinInvest 14(4): 306-311.
-
Prickett CD, Lister E, Collins M, Trevithick-Sutton CC, Hirst M, et al. (2004) Alcohol: Friend or Foe? Alcoholic Beverage Hormesis for Cataract and Atherosclerosis is Related to Plasma Antioxidant Activity. Nonlinearity Biol Toxicol Med 2(4): 353-370.
-
Knabbe J, Protzmann J, Schneider N, Berger M, Dannehl D, et al. (2022) Single-dose ethanol intoxication causes acute and lasting neuronal changes in the brain. Proc Natl Acad Sci USA 119(25): e2122477119.
-
Kubiak-Tomaszewska G, Tomaszewski P, Pachecka J, Struga M, Olejarz W, et al. (2020) Molecular mechanizms of ethanol biotransformation: enzymes of oxidative and nonoxidative metabolic pathway in human. Xenobiotica 50(10): 1180-1201.
-
Daviet R, Aydogan G, Jagannathan K, Spilka N, Koellinger PD, et al. (2022) Associations between alcohol consumption and gray and white matter volumes in the UK Biobank. Nat Commun 13(1): 1175.
-
Jin X, Long T, Chen H, Zeng Y, Zhang X, et al. (2022) Associations of Alcohol Dehydrogenase and Aldehyde Dehydrogenase Polymorphism with Cognitive Impairment among the Oldest-Old in China. Front Aging Neurosci 13: 710966.
-
Anthenelli RM, McKenna BS, Smith TL, Schuckit MA (2021) Relationship between level of response to alcohol and acute tolerance. Alcohol Clin Exp Res 45(7): 1504- 1513.
-
Motschman CA, Warner OM, Wycoff AM, Davis-Stober CP, McCarthy DM (2020) Context, acute tolerance, and subjective response affect alcohol-impaired driving decisions. Psychopharmacology (Berl) 237(12): 3603- 3614.
-
Florence L, Lassi DLS, Kortas GT, Lima DR, de Azevedo- Marques Périco C, et al. (2022) Brain Correlates of the Alcohol Use Disorder Pharmacotherapy Response: A Systematic Review of Neuroimaging Studies. Brain Sci 12(3): 386.
-
Park SH, Lee YS, Sim J, Seo S, Seo W (2022) Alcoholic liver disease: a new insight into the pathogenesis of liver disease. Arch Pharm Res 45(7): 447-459.
-
Paquot N (2019) The metabolism of alcohol. Rev Med Liege 74(5-6): 265-267.
-
Ren T, Mackowiak B, Lin Y, Gao Y, Niu J, et al. (2020) Hepatic injury and inflammation alter ethanol metabolism and drinking behavior. Food Chem Toxicol 136: 111070.
-
Daré BL, Lagente V, Gicquel T (2019) Ethanol and its metabolites: update on toxicity, benefits, and focus on immunomodulatory effects. Drug Metab Rev 51(4): 545- 561.
-
Pigolkin Ju I, Morozov Ju E (2012) Neurohistochemical researches of enzymes in forensic medicine. Tihookeanskij medicinskij zhurnal 1: 76-80.
-
Pigolkin Ju I, Morozov Ju E, Mamedov VK (2012) Medicolegal diagnosis of sharp and chronic alcoholic intoxication. Sudebno-medicinskaja ekspertiza 1: 30-33
-
Allen HC, Weafer J, Wesley MJ, Fillmore MT (2021) Acute rewarding and disinhibiting effects of alcohol as indicators of drinking habits. Psychopharmacology (Berl) 238(1): 181-191.
-
Comley RE, Dry MJ (2020) Acute tolerance to alcohol- induced impairment in cognitive performance. Experimental and Clinical Psychopharmacology 28(6): 659-668.
-
Abrahao KP, Salinas AG, Lovinger DM (2017) Alcohol and the Brain: Neuronal Molecular Targets, Sinapses, and Circuits. Neuron 96(6): 1223-1238.
- Forensic Implications of Adverse Drug Reactions in Schizophrenia A Case Series
- Narcotics and Digital Forensics: Bridging Crimes in the Digital Age
- Ethics in Forensic Psychiatry: Principles, Dilemmas, and Human Rights
- Impact of Acute Stress on Attentional Orienting to Social Cues
- Head Injury and Intracranial Hemorrhage in Western Region of Libya
- A Forensic Study on Handedness: Examination of Handwriting Features in Right and Left Handed Writers