Dealing with Death: A UK Perspective
There are about half a million deaths in England and Wales annually [1]. Most of these deaths are from natural causes, whether that be through natural illness, unfortunate circumstances or simply ‘old age’. Approximately 55% of deaths can be accounted for when a medical practitioner issues a document certifying the death as being due to known medical conditions.
Editorial
Death Investigation in England and Wales
There are about half a million deaths in England and Wales annually [1]. Most of these deaths are from natural causes, whether that be through natural illness, unfortunate circumstances or simply ‘old age’. Approximately 55% of deaths can be accounted for when a medical practitioner issues a document certifying the death as being due to known medical conditions.
Of this half a million deaths, about 45% will not be clear cut [2]. These will be cases where a doctor is unable to immediately identify the cause of death and so referral is made to the coroner for investigation and usually attended by the police who conduct an initial investigation at the scene on behalf of the coroner.
The vast majority of the deaths referred to coroners will be deemed as ‘non-suspicious’ where there is no suspected third-party involvement. The coroner may or may not request that a post mortem (PM) examination of the body takes place by a pathologist to assist in the identification of the cause of death. Approximately two thousand deaths annually will be treated as ‘suspicious’ from the outset [3].
Usually, the pathologist asked to conduct such an autopsy is a ‘hospital pathologist’ known as a ‘histopathologist’ who is trained in autopsy practice. A histopathologist is a medical doctor who specialises in the examination of human tissue under a microscope and assists in the diagnosis of disease in both the living and the dead. In a death case, the report from the pathologist will go with other evidence gleaned by the coroner who will decide on a cause of death and issue a death certificate accordingly. Autopsy practice is normally ancillary to the main role of disease diagnosis that histopathologists perform, and therefore conducting autopsies is outside of their National Health Service contracts, so they are conducted as part of a private arrangement between the histopathologist and the coroner.
Of the two thousand cases annually dealt with as deaths where there is the possible involvement of a third person, the coroner in consultation with the police will order what is known as a ‘forensic post mortem’ examination, and a ‘Home Office Registered Forensic Pathologist’ (HORFP) will be called upon to conduct this examination. Of these forensic cases, approximately one third have historically transpired to have been homicide [4]. If a homicide is suspected, the coroner will suspend their investigation until the police investigation is complete.
The decisions made by the police and the coroner in the early stages of an unexplained death are therefore very important contributors to the outcome. Failure to identify a suspicious death may lead to the homicide being undetected because an untrained histopathologist may not pick up on indicators pointing to foul play. A homicide can be missed or at best, vital forensic evidence could be lost. The initial investigation can be a difficult call. If the wrong decision is made it could be fatal to the investigation.
The Coronial System
The system of death investigation in England and Wales is complex and its origins based in history and commonly referred to as the ‘coronial’ system [5]. The coronial system was established in England during the reign of Richard 1st [5]. The word ‘Coroner’ was derived from the original title of ‘Crowner’ and their purpose was primarily the collection of revenue to support King Richard’s conquests in the Holy Land. This was done by establishing an inquisition into the death of a person and recovering any assets due but also enquiring as to the cause of death with a view of identifying cases of murder and in particular suicides. Suicide was an offence against god, and therefore all assets of the deceased were taken by the state and became the property of the King [5] (See also Jones and Milne, 2023 for a history) [6].
The primary role of a coroner in modern times is to inquire into the death of a human being within their jurisdiction. Their role was directed by several statutes and rules but has now been consolidated into current legislation under the Coroners and Justice Act 2009. Section 1 of the Act defines the primary role of the coroner to investigate a death where the body lies within their jurisdiction if:
- The deceased died a violent or unnatural death;
- The cause of death is unknown; or
- The deceased died while in custody or otherwise in state detention.
In practical terms, this is any death where a medical practitioner cannot issue a Medical Certificate of Cause of Death (MCCD).
The purpose of the coronial investigation is to establish who the deceased was, how, when and where the deceased came by their death and the particulars required to register the death [7].
The detailed guidance as to the role of the coroner is set out in the ‘Guide to Coroners Services’ [8]. Coroners are independent judicial appointees and are paid and funded by local authorities. Their governmental oversight lies with the Ministry of Justice and since July 2013, all newly appointed coroners must be legally qualified. This new requirement is controversial in some quarters as it is argued it may lead to unnecessary autopsies being ordered by legally qualified coroners, nervous about calling the cause of death because they are not knowledgeable about medical issues [9].
Carpenter, et al. [9] further claimed that there is an over reliance on the medical reports from the pathologist rather than the scene report outlining the circumstances of the death, resulting in more focus on the ‘science’ rather than the investigation. This is due to the perceived superiority of the ‘scientific’ medical evidence verses what is seen as less scientific circumstantial and physical evidence from the police investigation at the scene [9].
This over reliance on autopsy demonstrates a risk averse approach which is driven partly by a fear of missing homicides. If the coroner makes the call without the post mortem (PM), and it is wrong, it is the coroners fault. If a PM is conducted and the outcome is wrong, it is the pathologists’ fault [9]. The opinion that there is a risk averse attitude of coroners is supported by Luce [10] and Smith [11]. Over reliance on the medical cause of deaths can lead to less consideration as to why the death occurred which the medical evidence cannot reveal [9].
The 2009 Coroners and Justice Act created the post of ‘Chief Coroner’ whose main responsibility is to provide support, leadership and guidance for coroners in England and Wales. The 2009 Act also introduced the concept of ‘Medical Examiners’. This was due to recommendations of Dame Janet Smith in the 2003 public enquiry which took place following the conviction of Dr Harrold Shipman for murdering what is estimated to be at least 215 of his patients dating back to the 1970’s [11]. The necessity for medical examiners was reinforced by the Francis Inquiry into the Mid Staffordshire Foundation Trust [12] and the Kirkup Inquiry into the Morecambe Bay disaster [13], where it was recognised that the quality of the Medical Certificate of Cause of Death (MCCD) reports completed by doctors was flawed [14, 15, 16, 17, 18]. The medical examiners system, unlike the system of the same name in other jurisdictions, will not replace coroners, but acts as an oversight second opinion for all deaths except those which are referred to coroners from the outset. It is still unclear how medical examiners when appointed will interact with coroners but speculation was made by the interim National Medical Examiner, Professor Peter Furness for which the title of his lecture to the Medico- legal Society in 2012 sums up the possibilities; ‘Mutualism, Commensalism or Parasitism?’ [19]. Since, that lecture the system of medical examiners has been piloted in various parts of the country and a review of these pilot studies found that the quality of death certification by doctors improved; there was more consistency of reporting to coroners where a doctor could not issue a certificate and a better liaison with next of kin. In one pilot area the medical examiner altered the MCCD in 83% of cases and in another site 33% required ‘major changes’ [20]. Figure 1 appears complex but in fact the medical examiners system will, in theory, improve the quality of death investigation and assist to reduce the potential for missed homicide in those cases where a doctor has issued a death certificate (MCCD).
Overview of Process for Death Certification
from ONS Clinical Governance data on patterns and trends / issues Invitation to reissue MCCD Notification Death Verification of Fact of death & decision whether to notify coroner Scrutiny of MCCD & info MCCD Prepared by QAP & copied to ME with Statutory information to registrar of Ext. examination & discussion with confirmed or certified cause of doctor & relatives Option: Records provided for ‘Early Scrutiny’ Deaths Advice provided by ME to referred as Notifiable a result of scrutiny Coroner deaths & enquires doctors / QAP, coroner and/or coroner’s officers ’ Form 100A Form Initial Assessment Initial Assessment Talk with Initial Discussion relatives etc. if required and with a doctor when a death is reported / notified Decision to investigate decide whether Advice that investigation is to investigate not required Key:
Doctors, clinicians & other healthcare staff Service officers and staff Process step(s) carried out by:
Confirmation If new concerns raised during registration of deaths for which ME has issued a ME-2 Registration Burial or MCCD Issued to informant Cremation usually before burial / cremation (except if urgent or after green form from Registrar or coroner’s order/cert .
where inquest) Form 99 or 120 & 121 Form 100B
Investigation Investigation
Coroner’s Post Mortem
Inquest
Coroner’s burial order
if required or certificate for cremation The inquest stage of the investigation may be suspended as a result of criminal proceedings, public inquiry or an investigation by another country into a death in their jurisdiction and then either resumed or not resumed.
Registrars, funeral directors & Medical Examiners’ Coroners and their cemetery / crematorium staff Abbreviations & Notes: QAP = Qualified attending practitioner. ME = Medical examiner. Statutory information required with the copy of the MCCD may be documented in records.
External examination may be delegated in certain conditions. The Coroner Form is issued by a coroner for deaths that have been reported, notified or referred, but do not need to be investigated.
Types of Death Investigation
All deaths in England and Wales must be registered with the Registrar of Births, Marriages and Deaths.
This registration is required under the Births and Deaths Registration Act 1953 and registration must take place before the body can be released for burial or cremation and the financial and legal affairs can be settled. Before the registrar can make an entry of the death in the register of births marriages and deaths and thereby issue a death certificate to the next of kin, they must be in receipt of a MCCD issued by a medical practitioner if the legal conditions are met. These conditions are described in Table 1 and termed as a ‘non-suspicious community death’. If these conditions are not met, the next of kin will require a certificate issued by a coroner. The undertaker will require a copy of the death certificate from the registrar prior to disposal of the body. If the body is to be cremated, a second medical practitioner must verify the cause of death before the body is released by the undertaker. This is clearly because once destroyed by fire, no further examination can take place, whereas, if the body is buried, it can be exhumed and examined later if further information comes to light which casts doubt on the original cause of death [21].
Therefore, a death will fall into one of three categories which will determine the way in which it is investigated. Table 1 briefly explains these. We therefore see three broad categories of non-suspicious; unknown (or ‘grey’) and suspicious.
| Investigation | Decision Maker | Outcome | Process |
|---|---|---|---|
| Non-suspicious community death | Doctor | Certificate Issued | A death certificate (MCCD) may be issued by a doctor (under Births and Deaths Registration Act 1953) who has provided care during the last illness and who has seen the deceased within 14 days of death or has seen the body after death and where there are no circumstances leading to suspicion of third party involvement (ONS, 2010). These are normally deaths which occur in the community or in hospital settings and are expected due to terminal illness and are not routinely referred to the police or the coroner for investigation. |
| Non-suspicious death where conditions for Doctor to issue a certificate are not satisfied | Coroner | Coronial Investigation. Certificate issued after decision or inquest | In circumstances of unexpected death where the deceased was not being treated for an illness and/or has not been seen within 14 days of death, the case must be referred to a coroner (Births and Deaths Registration Act 1953). The police will normally inquire into the death on behalf of the coroner who may, depending on the circumstances of the case, order there to be a post mortem examination of the body and may also order an inquest (Coroners and Justice Act, 2009). |
| Suspicious Death | Coroner Police | Police Investigation followed by Coronial Investigation | Where death is unexpected and unexplained and there are circumstances which arise as to the possibility that there may have been a third-party involvement, the coroner will be informed, but the police will conduct an initial investigation. If the results of that investigation allay fears of third party involvement in the death, the case will be referred back to the coroner to complete investigations and consider whether an inquest is required. If, however the outcome of the initial investigation points towards third party involvement, the police will commence a homicide investigation. In such cases, the coroner’s investigation will be suspended until the outcome of the homicide case or the case has been heard by a Crown Court. |
| Hospital Death | Doctor and NOK[1] | Post Mortem for learning purposes | If a person dies in hospital whist being treated, the next of kin can ‘consent’ to a post mortem to discover the cause of death. This is done in the interests of learning and future death prevention. However, such post mortems are rare in recent years, which have caused some concern amongst the pathology profession as this source of data is being eroded [22]. |
Table 1: Investigation of Death.
The Initial Police Investigation
The police will be involved in the initial investigation of the death only in circumstances where a doctor cannot certify from known facts regarding the patients’ medical condition. Upon the report of a sudden and unexpected death, a police officer will be deployed to the place where the body has been discovered or currently lays, which could be the hospital if admission had taken place or death had occurred on route to the hospital. It will be the responsibility of that police officer to make an initial assessment of the death as to whether there may be third party involvement or not; in other words, to treat the death as ‘suspicious’, or to satisfy themselves that no suspicious circumstances exist [23]. There is no clear guidance, even within the ‘grey literature’ which sets out a process for this part of the investigation.
If it is thought that the death may be suspicious, medical assistance will be required to provide an initial opinion as to the medical cause of death. A ‘police doctor’ sometimes referred to as a ‘Force Medical Examiner (FME) may be called to the scene but unlike forensic pathologists, they are not trained to provide a medico-legal cause of death [23]. Other than pronouncing that ‘life is extinct’, the FME may not be able to offer any expert opinion as to the cause and surrounding circumstances of the death apart from in the most obvious of cases. There is a lack of nationally accepted advice regarding the process of having a doctor contracted by the police attending unexplained deaths, and there is no law or national policy in relation to the need for a medical professional to declare that life is extinct. At this stage, if the first attending officer considers that the death may be suspicious, the investigation will be referred to detective officers and crime scene examiners. If the view remains that expert medical opinion on the cause of death is required, the services of a HORFP will be called to conduct a forensic PM examination and to advise at the scene if appropriate [23]. However, the HORFP will not be called if the view of the attending police officers is that there are no suspicious circumstances, and it is considered that the case is a straightforward non-suspicious coroners’ case. If no suspicious circumstances are identified, the police officer will arrange for the body to be recovered by an undertaker and a report will be completed for the information of the coroner. Based upon the police report and any other facts gleaned from the deceased’s medical records and witness evidence, the coroner will decide on the conduct of the coronial investigation and whether a non-forensic PM examination is required.
Prior to a homicide investigation commencing, the most likely scenario is that there will be a reported incident of some kind. This may be a fight, an accident or a discovery of a body. In any event there is typically limited information and so a uniformed police officer is deployed [24]. The Murder Investigation Manual (MIM) [23] describes the priorities of the first attending officers and is known as the ‘Five Building Block Principles’ outlined in Figure 2 [23].
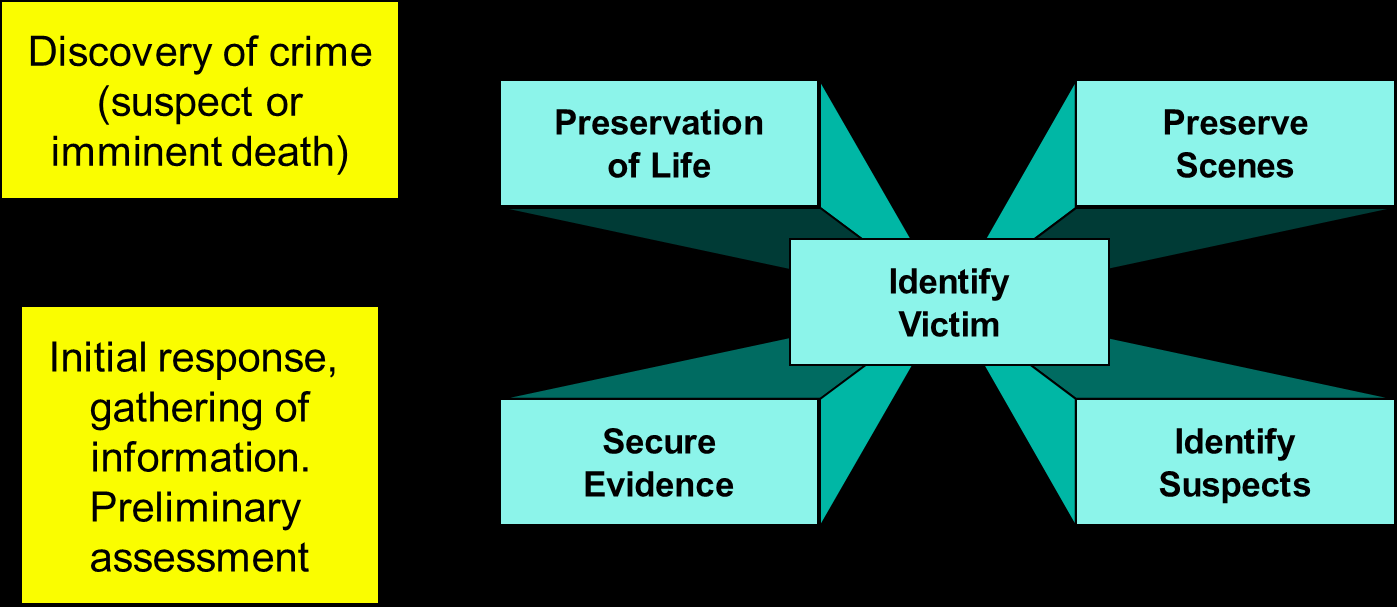
These five principles are self-explanatory with the preservation of life clearly being the overriding one. The MIM [23] describes processes and acknowledges that identifying whether a death is a potential homicide can be very difficult, and states that all cases should be treated as a homicide until the evidence proves otherwise [23]. However, it offers little guidance to officers on decision making. One of the main weaknesses is that the document was written for the Senior Investigating Officer (SIO) and not the officers who are most likely to attend, few of which would have ever heard of the manual [25].
Some scenes are easier to identify than others [26], such as those described as ‘self-solvers’ (as opposed to ‘whodunits’) – cases where the person responsible is obvious [26].
The importance of the police initial response to crime more generally is also important to the outcome [27, 28].
The first stage of the investigation is sometimes referred to as the ‘Golden Hour’, which is the period most critical to the investigation in terms of losing evidence and identifying witnesses [29].
The Coronial Investigation
The reason that the coroner is an important figure in the potential for homicides to be missed is because of their gate keeping and decision-making role in death investigations referred to them. Because only the coroner can authorise a PM examination under Section 14.1 of the Coroners and Justice Act (2009), any erroneous decision leading to a missed homicide may be shared between the police and the coroner.
However, the coroner does rely on the police report and opinion in making directions as part of their investigation.
If the police investigation at the scene is inadequate, the decision making thereafter may be flawed [9, 30]. There are political influences which can shape the decisions of professional death investigators, especially when suicide is suspected where there is great pressure to reclassify for the sake of grieving relatives [31].
Another area of external influence relates to terminally ill people where the euthanasia debate is often encountered [32]. It can therefore be seen that there are outside influences to decision making other than the actual evidence from the scene and at autopsy. There are also social issues which can affect an investigation into a death such as a reluctance of some police officers to examine a dead body or do not know what to look for [31]. There may be objections to the invasive PM process on ethical or religious grounds [4].
There have been several academic studies in relation to shortcomings in the current coronial system, none of which have been ‘fixed’ by the 2009 Coroners and Justice Act, which introduced largely cosmetic changes and has been viewed by many within the system as a missed opportunity [33]. The deaths caused by Dr Harold Shipman, the Marchioness disaster and the Alder Hay tissue scandal all highlighted that the system is not watertight [34].
Although there have been several reviews dating back to 1920, there has been no significant change in a system which is embedded in history [35, 36, 37].
Whatever the shortfalls of the coronial system, the one of the main reasons for the coronial investigation is to identify suspicious deaths where third party involvement is suspected, in other words ‘homicide’. If the coroner’s inquest cannot identify a cause of death, the jury will normally return what is termed an ‘open verdict’ – this means that the cause of death cannot be established and doubt remains as to how the deceased came to their death. There were over 1700 open verdicts in England and Wales in 2015 [1] and although the majority tend to be possible but unproven suicides, this is the arena where unidentified homicides are most likely to be found [1].
References
-
MoJ (Ministry of Justice) (2016) Coroners Statistics.
-
MoJ (Ministry of Justice) (2014) Coroners Statistics.
-
Jones D (2016) The Role of Forensic Pathologists. Home Office Forensic Pathology Unit pp: 1-2.
-
Hutton P (2015) A review of forensic pathology services in England and Wales. The Home Office pp: 1-107.
-
Knight B (2008) Crowner: Origins of the Office of Coroner. Britannia History.
-
Jones D, Milne R (2023) The Coronial System: A Short History. International Journal of Forensic Sciences 8(2): 1-5.
-
Fairbairn C (2014) Coroners Investigations and Inquests. Standard Note SN/HA/3981. House of Commons Library.
-
MoJ (Ministry of Justice) (2014a) A Guide to Coroner Services for Bereaved People.
-
Carpenter B, Tait G (2010) The Autopsy imperative: Medicine, law, and the coronial investigation. Journal of medical humanities 31(3): 205-221.
-
Luce T (2003) Death Certification and Investigation in England, Wales and Northern Ireland: The Report of a Fundamental Review 2003. Stationery Office.
-
Smith J (2004) 1. The Shipman Inquiry–Death Certification. Medicine Science and the Law 44(4): 280- 287.
-
Francis R (2010) Robert Francis Inquiry Report into Mid-Staffordshire NHS Foundation Trust. The Stationery Office: London, UK.
-
Kirkup B (2015) Morscombe Bay Failings could happen again. The Health service journal 125(6454): 16-17.
-
Fernando D, Oxley JD, Nottingham J (2012) Death certification: do consultant pathologists do it better?. Journal of clinical pathology 65(10): 949-951.
-
James DS, Bull AD (1996) Information on death certificates: cause for concern? Journal of clinical pathology 49(3): 213-216.
-
Roulson J, Benbow EW, Hasleton PS (2005) Discrepancies between clinical and autopsy diagnosis and the value of post mortem histology; a meta‐analysis and review. Histopathology 47(6): 551-559.
-
Slater DN (1993) Certifying the cause of death: an audit of wording inaccuracies. Journal of clinical pathology 46(3): 232-234.
-
Swift B, West K (2002) Death certification: an audit of practice entering the 21st century. Journal of clinical pathology 55(4): 275-279.
-
Furness P (2012) Coroners and medical examiners: mutualism, commensalism or parasitism? Medico-Legal Journal 80(3): 86-101.
-
Furness PN, Fletcher AK, Shepherd NA, Bell B, Shale D, et al. (2016) Reforming Death Certification: Introducing Scrutiny by Medical Examiners. Department of Health pp: 1-18.
-
(2016) Introduction of Medical Examiners and Reforms to Death Certification in England and Wales: Policy and Draft Regulations. Department of Health pp: 1-92.
-
Burton JL, Underwood JCE (2003). Necropsy practice after the “organ retention scandal”: requests, performance, and tissue retention. Journal of clinical pathology 56(7): 537-541.
-
ACPO (2006) Murder Investigation Manual.
-
Feist A and Newiss G (2000) Watching the Detectives: Analysing hard to solve homicide investigations. Unpublished Report for the Home Office Policing and Reducing Crime Unit.
-
Fox J (2013) An evaluation of the effectiveness, use and future of police professional practice publications. ProQuest University of Surry pp: 1-349.
-
Waddington PAJ (2003) Investigating Murder: detective work and the police response to criminal homicide. Oxford: Clarendon Press. The British Journal of Criminology 44(1): 142-144.
-
Steer D (1980) Uncovering Crime: The Police Role, Crown Publishers, New York, United States.
-
Eck EJ (1983) Solving Crimes: The Investigation of Burglary and Robbery, Washington DC, USA.
-
Cook T, Tattersall A (2010) Blackstone’s Senior Investigating Officers’ Handbook, In: 6th (Edn.), Oxford University Press.
-
Jones D, Milne R (2016) Fatal call - getting away with murder: a study into influences of decision making at the initial scene of unexpected death. Doctor of Criminal Justice Studies University of Portsmouth pp: 1-247.
-
Timmermans S (2006) Post Mortem: How Medical Examiners Explain Suspicious Deaths. University of Chicago press, USA, pp: 1-367.
-
Materstvedt LJ (2003) The Euthanasia Debate. Palliative medicine 17(387): 392.
-
Cooper H, Leigh MAMS, Lucas S, Martin I (2007) The coroner’s autopsy. The final say in establishing cause of death?. Medico-Legal Journal 75(3): 114-119.
-
Berry C, Heaton-Armstrong A (2005) A review of the coroner system in England and Wales: a commentary. Clinical medicine 5(5): 455-459.
-
Palmer R (2012) Death and the coroner: some reflections on current practice and proposed reforms. Medicine Science and the Law 52(2): 63-70.
-
(2021) National Police Chief’s Council. Major Crime Investigation Manual. NPCC.
-
Office for National Statistics (2010) Guidance for doctors completing Medical Certificates of Cause of Death in England and Wales. Certification Advisory Group pp: 1-16.
- Forensic Implications of Adverse Drug Reactions in Schizophrenia A Case Series
- Narcotics and Digital Forensics: Bridging Crimes in the Digital Age
- Ethics in Forensic Psychiatry: Principles, Dilemmas, and Human Rights
- Impact of Acute Stress on Attentional Orienting to Social Cues
- Head Injury and Intracranial Hemorrhage in Western Region of Libya
- A Forensic Study on Handedness: Examination of Handwriting Features in Right and Left Handed Writers