Death Confirmed After the First Administration of Coronavirus Vaccine Recognized by Health Authorities and Compensated
We describe a case in which the health authorities in Italy established a causal link between the death of a 72-year-old man and the administration of the anti-COVID vaccine. After the administration of the first dose of the ChAdOx1 nCov-19 vaccine (AstraZeneca), which took place in 2021, the man-who was in excellent physical condition, as evidenced by a series of clinical tests carried out shortly before the inoculation-began to experience frequent illnesses. Hospitalization was of no avail: the elderly man died after 15 days of hospitalization and 43 days from the administration of the vaccine. The autopsy confirmed that the cause of death was attributable to the vaccination against COVID-19. For this reason, in 2024, the deceased's family received compensation of approximately €100,000. Specifically, the Hospital Medical Commission-which acted on behalf of the Italian Ministry of Health in the administrative procedure aimed at granting the compensation-outlined a picture of "multi-organ failure" in "consumptive coagulopathy." In fact, during the autopsy, the presence of thrombi (mainly affecting the arterial microcirculation) in many organs was ascertained, attesting to the direct correlation between the vaccination and the death.
Abbreviations
EMA: European Medicines Agency; VITT: Vaccine Immune Induced Thrombotic Thrombocytopenia.
Introduction
With the outbreak of the COVID-19 pandemic, several SARS-CoV-2 vaccines were authorized on an emergency basis.
Following the recommendations of the European Medicines Agency (EMA), the European Union authorized the use of four vaccines, allowing a gradual return to pre- pandemic life. In detail, the BNT162b2 vaccine (Pfizer- BioNTech) was approved on December 21, 2020 [1]; another vaccine, mRNA-1273 (Moderna) [2] was approved on January 6, 2021; the third vaccine, ChAdOx1 nCov-19 (AstraZeneca) was approved on January 29, 2021 [3]; finally, the fourth vaccine was Ad26.COV2.S (COVID-19 Vaccine
Jansen–Johnson & Johnson) and was authorized on March 11, 2021 [4].
In various countries, several adverse effects occurred- sometimes fatal [5] and all this generated hesitation, suspicion, and distrust towards these vaccines in the general population [6, 7]. The Italian Constitutional Court has repeatedly reiterated that the State can impose (or strongly recommend) vaccination because the individual’s freedom of self-determination can be limited for the protection of a collective good (which, in the case of vaccination, is the protection of public health), but it has always also added that the State must take charge of the damage to health that may result (rare and generally of a minor nature) for the duty of social solidarity that weighs on the entire community and for the full implementation of the right to health, which is also constitutionally recognized.
Clinical Report
Information on the patient who had died in mid- June 2021, which was provided to me (MG) just prior to performing the autopsy, revealed that at the beginning of May 2021 he had received the first dose of the AstraZeneca vaccine (Vaxzevria). Two weeks after the administration of the vaccine the first symptoms appeared, namely a widespread erythema over the entire body, with a slight feeling of dizziness and tiredness. Subsequently, the patient was admitted to the emergency department at the beginning of June where he had arrived due to the persistence of the
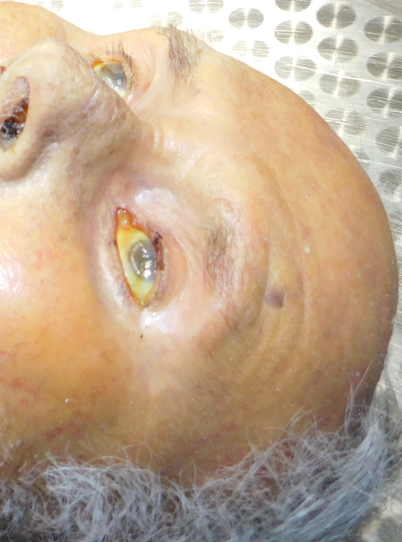
1. Diffuse yellowish skin color (Figure 1);
widespread erythema over the entire skin area that had already been present for 10 days and was associated with other symptoms. In fact, upon arrival at the emergency room, the following conditions were described: dyspnea, morbilliform skin rash, and fever.
He had remote medical history of arterial hypertension under pharmacological treatment. He reported that the erythematous skin rash and fever had appeared in the days following the administration of the vaccine, without any improvement in symptoms during the weeks since then. Hospitalization diagnosis was acute renal failure in a patient with fever and erythematous reaction.
During the 15 days of hospitalization, the following developed: generalized erythroderma with hyperosmolar dehydration, Stevens–Johnson syndrome, acute renal failure, consumption coagulopathy, severe cholestatic cytolytic involvement of the liver, soporous state, subdural hematoma in the right fronto-parietal subthecal area of 10 mm maximum thickness, and multiorgan failure. After 43 days from the administration of the vaccine, the patient died due to multiorgan failure in a suspected reaction to the AstraZeneca vaccine.
I was then charged with performing an autopsy to clarify and specify the cause of death. The subject was of tall stature (183 cm), male sex, robust build, and Caucasian ethnicity. The patient had:

2. Yellowish sclerae (Figure 2);
3. Mouth with complete edentulism entirely altered by the presence of blood clots and crusts (internally and externally) with brownish fluid leaking from the mouth when the body was moved (Figure 3);

4. Purpuric lesions all over the body-more evident on the posterior surface of the body (Figure 4);

5. Lungs of normal weight (left lung 658±257g, right lung 741±274g) [8]-on the left: 625g and on the right: 817g with areas of consolidation of hemorrhagic appearance; 6. The trachea had hemorrhagic petechiae; 7. There was an absence of pleuro-pericardial effusions; 8. Upon prior opening of the skull, nothing significant was observed on its deep surface and in the galea capitis. The skullcap was intact and symmetrical. The cranial vault was isolated and little blood material was leaking. The vault and the base of the skull were free from fracture lesions. Only a very small subdural blood layer was evident in the right fronto-parietal subthecal area; 9. The heart weighed 438 g normal (381±56g), pericardium was without particular alterations. On section, the myocardium of the left ventricle appeared diffusely discolored. The parietal endocardium without alterations and the atrioventricular valves had modest fibrosis. Aortic and pulmonary valves were normally shaped. The coronary ostia was normally positioned; the coronary arteries, examined in their entire course and in their main branches, presented an overall regular caliber without particular stenotic alterations; 10. Histologically, in the various areas there were thrombi and microthrombi, consisting of deposits of proteinaceous material, with abundant red blood cells and rare leukocytes trapped and occluding-entirely or partially-the vessel lumen, more evident at the skin and renal level but also present in numerous other districts. Thrombi and microthrombi were also present in the cerebral circulation (Figure 5A and 5B);
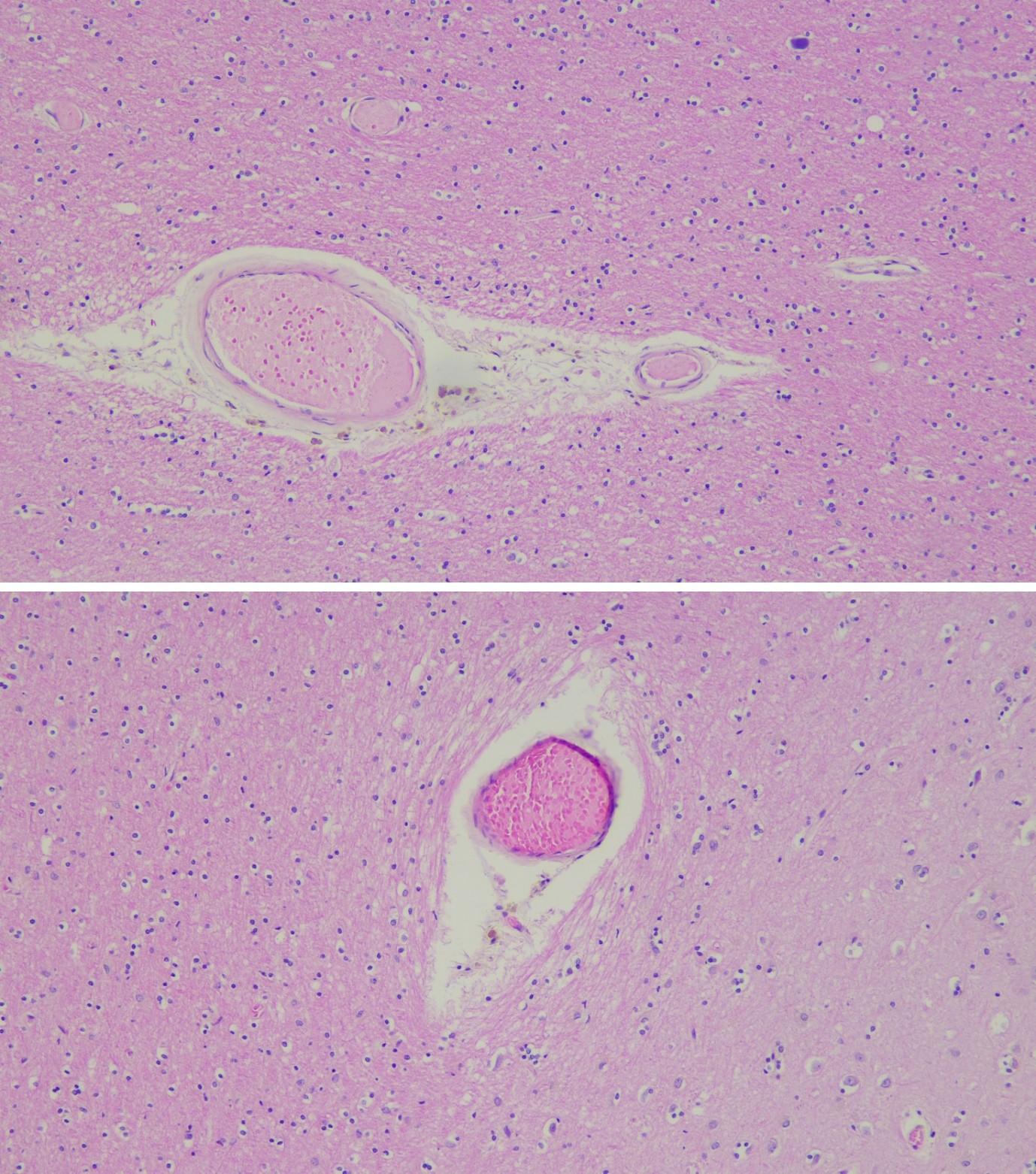
Figure 5A and 5B: Brain (H&E 20×): Evident Complete Microthrombi or Larger Vessels Partially Thrombosed, Arrows.
11. The skin showed widespread microthrombi in the vessels of the papillary dermis and reticular dermis (Figure 6);
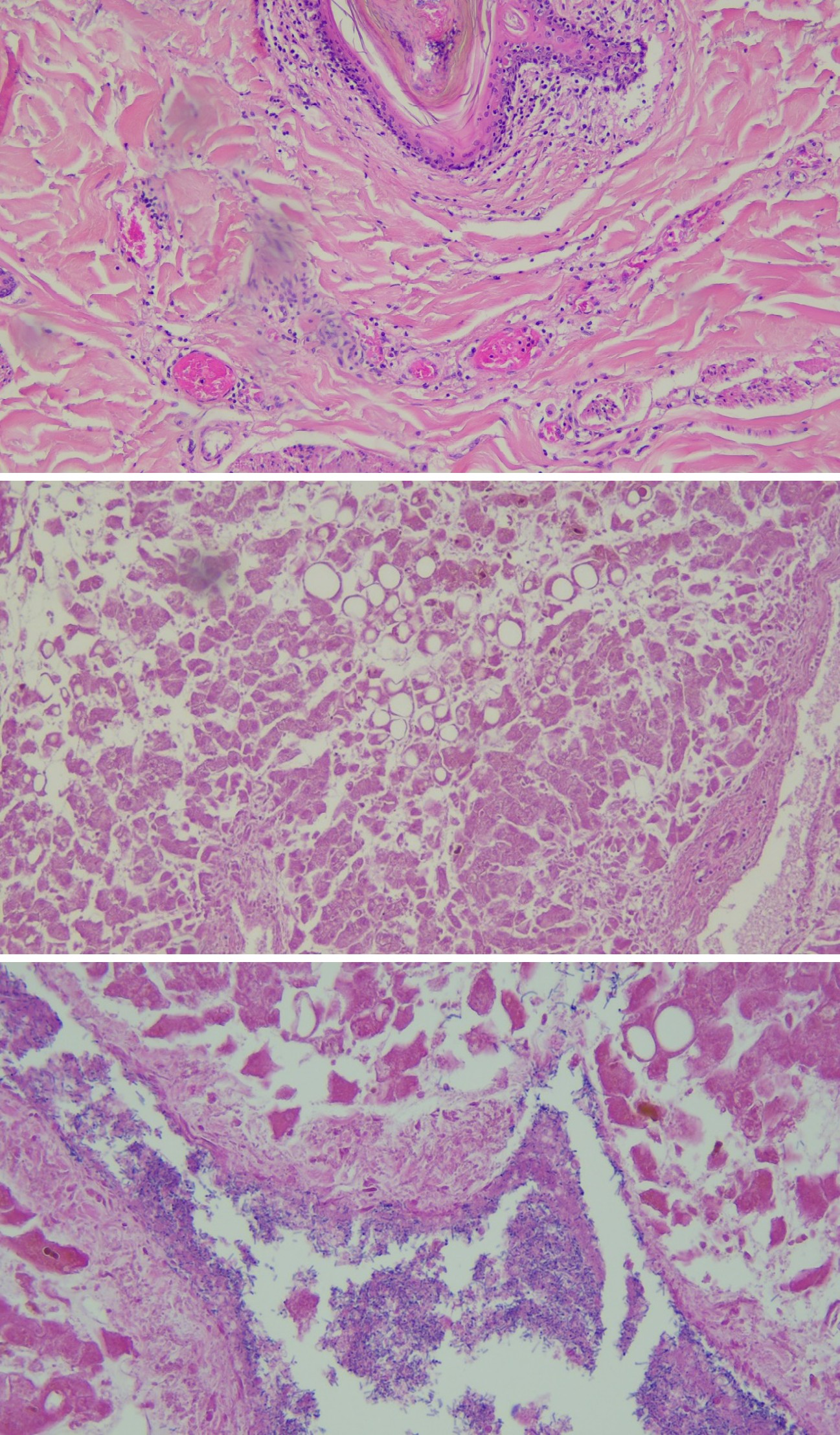
12. The liver showed micro and macrovesicular steatosis, significant cholestasis, tissue autolysis and abundant endovascular gram-positive bacilli of probable origin from post-mortem proliferation; vascular microthrombi were very rare (Figure 7A and 7B).
Figure 7A and 7B: Liver (H&E 10×, H&E 20×): Micro and Macrovesicular Steatosis, Significant Cholestasis, Abundant Intravascular Gram-Positive Bacilli of Likely Post-Mortem Proliferation Origin.
13. In the kidneys we located the most striking finding, in fact there were widespread microthrombi, even in the glomerular capillaries (Figure 8A-8D);
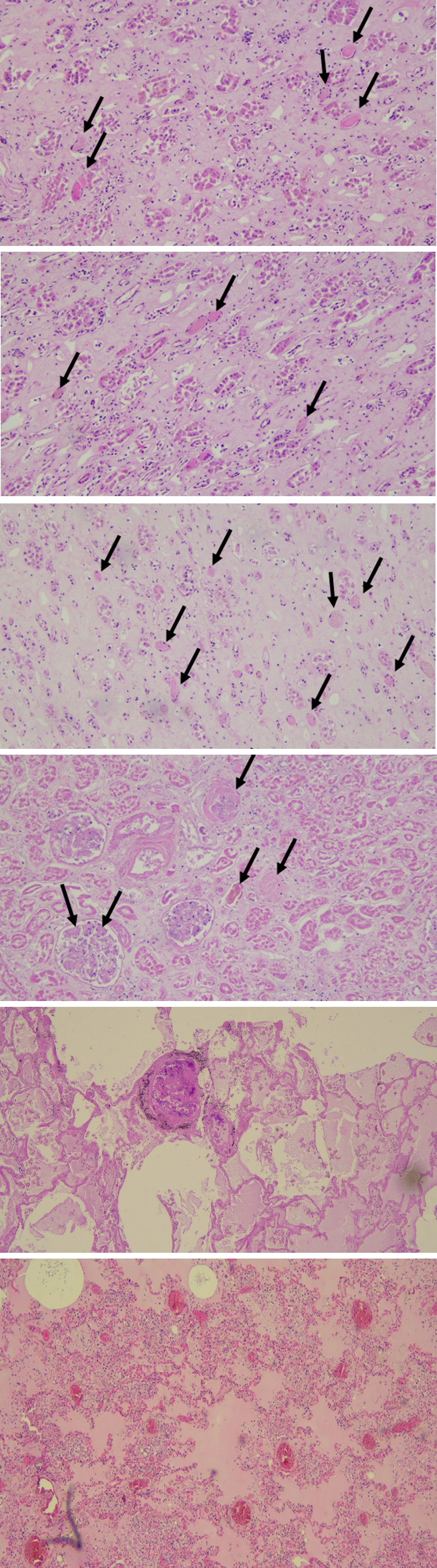
Figures 8A-8D: Kidneys (H&E 10×): There were Widespread Vascular Microthrombi (Arrows).
14. There was an absence of necrosis of the myocardiocytes; there was moderate myocardial fibrosis related to the patient’s age;
15. Pulmonary edema of moderate entity was evident. The basal areas showed alveolar blood suffusion with rare microthrombi also in the capillaries of the alveolar septa, with diffusely congested villous capillaries (Figures 9A-9C).
Figure 9A-9C: Lungs (H&E 10×): Moderate Pulmonary Edema, Congestion of Alveolar Capillary Vessels, Rare Microthrombi.
It was a very complex picture in which we highlighted thrombi and micro-thrombi in many organs, which mainly affected the arterial microcirculation.
We described the patient’s death as multiorgan failure in consumption coagulopathy.
Discussion
The key differences between VITT (Vaccine-Induced Immune Thrombotic Thrombocytopenia) and DIC (Disseminated Intravascular Coagulation) are the cause and mechanism of the disease. VITT is an autoimmune disorder induced by certain vaccines, which causes an immune reaction that damages the cells lining the blood vessels, leading to thrombosis (clot formation) and thrombocytopenia (low platelet count). DIC, on the other hand, is a condition in which abnormal and widespread clotting of the blood occurs in the microvessels, often in response to a serious illness or infection, such as sepsis. In other words, VITT is an immune disorder, while DIC is a clotting disorder, with different causes and mechanisms. According to the American Society of Hematology [9], vaccine-induced immune thrombocythemia (VITT) is defined as a clinical syndrome characterized by the following abnormal laboratory and radiological values and occurring in individuals vaccinated with Ad26.COV2. S or ChAdOx1 nCoV-19 vaccines 4–42 days after vaccination.
Here are the symptoms:
- Development of thrombosis at uncommon sites, including cerebral venous sinuses/splanchnic vein thrombosis;
- Mild to severe thrombocythemia. However, a normal platelet count does not exclude the possibility of this syndrome in its early stages;
- Positive antibodies against platelet factor 4 (PF4) detected by enzyme-linked immunosorbent assay;
- Significantly elevated D-dimer values (>4 times the upper limit of normal).
The case we are describing here met many (three out of four), but not all, of the criteria required for the diagnosis of VITT, as PF4 antibodies had not been tested. Unfortunately, the lack of PF4 antibody testing was a limitation of our study, but the case occurred in a peripheral hospital and this test was not available.
Fourteen days after the first dose of vaccine, the patient presented symptoms and rapidly developed a complex clinical situation, and 43 days after receiving the vaccine he died. Laboratory tests revealed a D-dimer value always between 2000 and 1800 mg/dL (n.v. <243); the platelets fluctuated significantly with values between 600x103µL decreasing drastically in the last days with values of 71, 52, and then 47x103µL at the last measurement before death.
As already described, in the autopsy, we found the presence of microthrombi in many organs, such as brain tissue, skin, and kidneys; these thrombi were present mainly in small capillary vessels. In larger vessels the lumen was only partially occluded by the thrombi.
In April 2021, just a few months after the administration of millions of doses of Ch-AdOx1 nCoV-19 vaccines on a global scale, the New England Journal of Medicine published three articles reporting the adverse events collected [10, 11, 12]. In these studies, the onset of the disease occurred between 6 and 24 days after the administration of the AstraZeneca vaccine. In the case in question, the symptoms appeared approximately 2 weeks after the vaccination, and 15 days’ hospitalization was necessary.
Similar cases to ours have already been described in Italy, such as the case described by Fanni D, et al. [13].
In Italy, the death of an 18-year-old girl due to thrombosis 16 days after the first dose of the AstraZeneca vaccine was received at an open vaccination day caused a great stir in public opinion. After this case, this vaccine was no longer indicated in Italy for women under 50 years of age [14, 15].
In Thailand in March 2024, 28 cases of death were described, which occurred after the AstraZeneca vaccination [16]; in this series, however, no case of VITT was described.
Another nine cases of death after the Vaxzervria vaccine were described in Germany in 2021, although in only two of these cases was an autopsy correlation established between vaccination and death [17].
Wiedmann M, et al. [18] had described a series of cases of five women who died and underwent autopsy, with hemorrhage and thrombocytopenia after administration of the first dose of ChAdOx1 nCOV-19 (AstraZeneca).
Several systematic reviews have been carried out to establish causal relationships between death and anti- COVID-19 vaccines; for example, studies from Sessa F, et al. [19] and Saluja P, et al. [20], which are aimed at demonstrating that despite the great emotional impact on the general population adverse events of anti-COVID-19 vaccines continue to be very rare.
Conclusions
The incidence of VITT, although rare, has in fact occurred in two or three people out of 100,000 vaccinated with the Vaxzervria vaccine. The incidence has been higher than in recipients of the Comirnaty vaccine, suggesting a causal relationship between these events and adenovirus-based vaccines [21, 22].
Autopsy always plays a vital role in describing the pathophysiology of the disease and the causes of death.
This case described by us also confirms the importance of autopsy-a diagnostic tool always fundamental to confirm a clinical diagnosis-in this case death related to the anti- COVID-19 AstraZeneca vaccination. For this reason, in 2024, the deceased’s family received compensation of approximately €100,000. The appropriate Hospital Medical Commission that acted at a local level as a body of the Italian Ministry of Health in the administrative procedure aimed at granting the compensation, outlined a picture of “multi- organ failure” in “consumptive coagulopathy.” In fact, during the autopsy, the presence of thrombi (mainly affecting the arterial microcirculation) in many organs was ascertained, attesting the direct correlation between the vaccination and the death.
Finally, on May 7, 2024, the EMA issued a notice that the AstraZeneca anti-COVID vaccine is no longer authorized for use.
The scientific community must work hard to reduce the feeling of vaccine hesitancy among the general population by scrupulously following the cases of fatal adverse reactions. We firmly believe that the autopsy-also in this case-played a fundamental role in establishing the causal links between vaccination, adverse events, and death. The autopsy is also the greatest tool for clarity in a clinical therapeutic process and in the clinical–pathological and morphological evaluation of a pathology.
Describing adverse events does not mean fueling fears and doubts, but it does mean clarifying the physiopathological mechanisms of adverse events and demonstrating how many cases of deaths are mistakenly believed to be linked to the vaccine are, in fact, not-together with an accurate and in- depth collection of anamnestic data before vaccination.
The adverse event cases described, which should always be considered extremely rare, should not change our view of the benefits provided by immunization to combat this global health crisis.
This study was carried out at the Pathology Unit of the “A. Cardarelli” Regional Hospital of Campobasso, Italy.
Authors’ Contributions
Massimiliano Guerriero performed the autopsy and prepared the manuscript. The biomedical laboratory technician Raimondo Carnevale helped during the study of the case in question. The laboratory technician Domenico Consiglio processed the tissues and prepared all the slides.
Ethics Statement
We obtained written consent from the relatives of the deceased for the use of this case for teaching and research. We ensured in the text that no reference was made to the deceased’s identity.
Ethics
The manuscript is in accordance with the rules of the Institutional Ethics Committee.
Conflict of interest
None
Funding
None.
References
-
EMA (2021) EMA Recommends First COVID-19 Vaccine for Authorisation in the EU.
-
EMA (2021) EMA Recommends COVID-19 Vaccine Moderna for Authorisation in the EU.
-
EMA (2021) EMA Recommends COVID-19 Vaccine AstraZeneca for Authorisation in the EU.
-
EMA (2021) EMA Recommends COVID-19 Vaccine Janssen for Authorisation in the EU.
-
European Centre for Disease Prevention and Control (2021) Suspected Adverse Reactions to COVID-19 Vaccination and the Safety of Substances of Human Origin. ECDC: Stockholm, Sweden.
-
Schwarzinger M, Watson V, Arwidson P, Alla F, Luchini S (2021) COVID-19 vaccine hesitancy in a representative working-age population in France: A survey experiment based on vaccine characteristics. Lancet Public Health 6(4): e210-221.
-
Solís Arce JS, Warren SS, Meriggi NF, Scacco A, McMurry N, et al. (2021) COVID-19 vaccine acceptance and hesitancy in low- and middle-income countries. Nat Med 27(8): 1385-1394.
-
de la Grandmaison GL, Clairand I, Durigon M (2001) Organ weight in 684 adult autopsies: new tables for a Caucasoid population. Forensic Sci Int 119(2): 149-154.
-
Aleem A, Nadeem AJ (2025) Coronavirus (COVID-19) Vaccine-Induced Immune Thrombotic Thrombocytopenia (VITT). Treasure Island (FL): StatPearls Publishing.
-
Schultz NH, Sørvoll IH, Michelsen AE, Munthe LA, Lund-Johansen F, et al. (2021) Thrombosis and thrombocytopenia after Ch-AdOx1 nCoV-19 vaccination. N Engl J Med 384(22): 2124-2130.
-
Greinacher A, Thiele T, Warkentin TE, Weisser K, Kyrle PA, et al (2021) Thrombotic thrombocytopenia after ChAdOx1 nCov-19 vaccination. N Engl J Med 384(22): 2092-1101.
-
Scully M, Singh D, Lown R, Poles A, Solomon T, et al. (2021) Pathologic antibodies to platelet factor 4 after ChAdOx1 nCoV-19 vaccination. N Engl J Med 384(43): 2202-2211.
-
Fanni D, Saba L, Demontis R, Gerosa C, Chighine A, et al. (2021) Vaccine-induced severe thrombotic thrombocytopenia following COVID-19 vaccination: a report of an autoptic case and review of the literature. Eur Rev Med Pharmacol Sci 25(15): 5063-5069.
-
ANSA English (2021) 18-year-old dies after having AstraZeneca vaccine.
-
Regioni.it (2021) AstraZeneca for young people: clarifications expected from the Technical Scientific Committee. Regioni.it-n. 4088.
-
Dul-Amnuay A (2024) Case study of autopsy findings in a population of post-COVID-19 vaccination in Thailand. Am J Forensic Med Pathol 45(1): 45-50.
-
Schneider J, Sottmann L, Greinacher A, Hagen M, Kasper HU, et al. (2021) Postmortem investigation of fatalities following vaccination with COVID-19 vaccines. Int J Legal Med 135(6): 2335-2345.
-
Wiedmann M, Skattor T, Stray-Pedersen A, Romundstad L, Antal EA, et al. (2021) Vaccine-induced immune thrombotic thrombocytopenia causing a severe form of cerebral venous thrombosis with high fatality rate: a case series. Front Neurol 12: 721146.
-
Sessa F, Salerno M, Esposito M, Di Nunno N, Zamboni P, et al. (2021) Autopsy findings and causality relationship between death and COVID-19 vaccination: a systematic review. J Clin Med 10(24): 5876.
-
Saluja P, Amisha F, Gautam N, Goraya H (2022) A systematic review of reported cases of immune thrombocytopenia after COVID-19 vaccination. Vaccines (Basel) 10(9): 1444.
-
Cari L, Alhosseini MN, Fiore P, Pierno S, Pacor S, et al. (2021) Cardiovascular, neurological, and pulmonary events following vaccination with the BNT162b2, ChAdOx1 nCoV-19, and Ad26.COV2.S vaccines: an analysis of European data. J Autoimmun 125: 102742.
-
Lee DS, Kim JW, Lee KL, Jung YJ, Kang HW (2022) Adverse events following COVID-19 vaccination in South Korea between February 28 and August 21, 2021: a nationwide observational study. Int J Infect Dis 118: 173-182.
- Forensic Implications of Adverse Drug Reactions in Schizophrenia A Case Series
- Narcotics and Digital Forensics: Bridging Crimes in the Digital Age
- Ethics in Forensic Psychiatry: Principles, Dilemmas, and Human Rights
- Impact of Acute Stress on Attentional Orienting to Social Cues
- Head Injury and Intracranial Hemorrhage in Western Region of Libya
- A Forensic Study on Handedness: Examination of Handwriting Features in Right and Left Handed Writers