Unique Skin Lesions in Suicidal Intravenous Pentobarbital Overdose: A Case Report and Literature Review
Background: Suicide is a significant public health concern, with certain professions such as veterinarians, exhibiting higher suicide rates. Among the common methods of suicide in veterinarians, self-poisoning with the euthanasic product pentobarbital is notably prevalent which can be explained by the accessibility of this drug. Methods: This case report examines the death of a 27-year-old female veterinarian who died from an overdose of intravenously administered pentobarbital. A review of the literature and a search of the database of the Department of Forensic Medicine at UZ Leuven for similar cases was performed. Results: In total, 21 cases of suicidal intoxications with barbiturates, primarily pentobarbital, were included. The 27-year-old veterinarian presented with distinctive skin lesions characterized by marbling, necrosis, and blister formation around the infusion site. These skin manifestations are seen only in cases of intravenous administration of pentobarbital. Common factors in these cases such as anatomical distribution are analyzed and a potential mechanism of origin is proposed. Conclusion: This article discusses the significance of unique skin lesions in forensic investigations, emphasizing their potential role as a pathognomonic sign for intoxications involving barbiturates.
Van Deuren I*¹, Van Brantegem L², Andelhofs D¹, Wuestenbergs J¹ and
Van Den Bogaert W1,3
¹Department of Forensic Medicine, University Hospitals Leuven, Belgium ²Department of Veterinary Medicine, Ghent University ³Department of Imaging and Pathology, Forensic Biomedical Sciences, KU Leuven, Belgium
Key points
- Auto-intoxication with barbiturates is a suicide method commonly used by veterinarians.
- Intravenous administration of pentobarbital can lead to characteristic skin lesions that are not seen when the drug is orally ingested or administered subcutaneously. Therefore they could serve as a pathognomonic sign.
• These specific lesion are thought to result from extravasation of the drug into the surrounding tissues after circulatory failure.
Abbreviations
CPR: Cardiopulmonary Resuscitation
Introduction
According to the World Health Organization, suicide is the third leading cause of death among individuals aged 15 to 29 years [1]. The most common methods of suicide worldwide include hanging, the use of firearms and self-poisoning with pharmaceuticals and pesticides. Occupational access to certain lethal means has been identified as a significant risk factor for suicide, with a particularly higher prevalence in females compared to males [2].
For example, veterinarians and other high-risk professions, such as physicians, exhibit higher suicide rates than the general population. The age-standardized suicide rate among veterinarians is estimated to be three to four times higher than average [3, 4]. Contributing factors to this increased risk include occupational access to lethal medications such as barbiturates, knowledge of their usage, and exposure to job-related stressors, illness, death and euthanasia.
A 2015 Australian study reported that self-poisoning was the most frequently used suicide method among veterinarians, with pentobarbital being involved in 80% of these cases [4]. Although intentional ingestion or injection of pentobarbital is a relatively rare suicide method among the general population, several cases have been documented [5].
The Peacefull Pill Handbook describes pentobarbital (Nembutal) as “the best euthanasia drug” and as “coming closest to the concept of the Peacefull Pill” [6]. Similarly, Final Exit, another book that describes suicide methods, refers to pentobarbital as the “premier drug for self- deliverance” [5].
Pentobarbital is a short-acting barbiturate primarily used in veterinary medicine as an anesthetic and euthanasia agent. Its use in human medicine has become rare due to its narrow therapeutic range and high risk of adverse effects. Current indications for pentobarbital include in-hospital treatment of seizures, status epilepticus, insomnia, high intracranial pressure and its use as a pre-anesthetic agent in surgeries [7].
Table 1 provides an overview of pentobarbital plasma concentrations and their associated effects [7, 8]. The drug is no longer recommended for outpatient use due to the widespread availability of benzodiazepines. However, despite being available only by prescription, pentobarbital is relatively easy to purchase online.
The diagnosis of pentobarbital intoxication, as with all toxicological-related deaths, relies on a combination of autopsy findings with toxicological analysis. To date, no pathognomonic signs have been described for pentobarbital or other barbiturate intoxications.
This report presents a fatal case of self-poisoning following the intentional intravenous injection of pentobarbital and discusses associated characteristic skin lesions that may serve as a potential indicator of such intoxications.
| Effects of pentobarbital | Concentration |
|---|---|
| Sedation | 1-5 µg/mL or 150-200 mg |
| Therapy for high intracranial pressure | 30-40 µg/mL |
| Inducing coma | 20-50 µg/mL |
| Toxic | > 10 µg/mL |
| Lethal | > 15 µg/mL |
Table 1: Therapeutic, Toxic and Lethal Plasma/Serum Concentration of Pentobarbital.
Case Report
Circumstances
A 27-year-old female veterinarian was found dead by her partner in the stable adherent to their home after she failed to show up at the veterinary practice where she was employed.
Emergency services were contacted but no cardiopulmonary resuscitation (CPR) was performed, nor was the body manipulated. She was last seen alive on the morning prior to her discovery. An investigation of her phone revealed that the deceased had recorded a farewell video message at approximately 7:30 p.m. the evening before she was found.
On the ground nearby the body, a box containing multiple gauze pads (clean and used ones), fixation tape and five empty syringes of different sizes (three of which had needles attached) were discovered. Additionally, a half empty bottle of liquor was found nearby. In the bedroom of the adjoining house, there was a pile of clothes with a note reading “Will you let me put these on? xxx”.
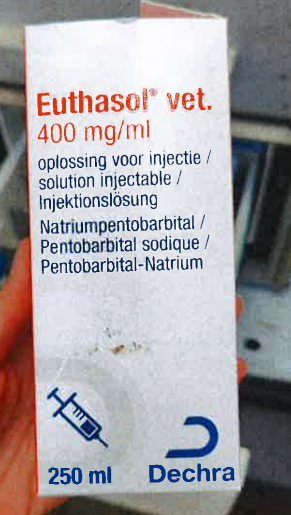
During the death scene investigation, the deceased’s car was searched, revealing multiple veterinary drugs, including a 250 mL bottle of Euthasol® (sodium pentobarbital, 400 mg/mL), an injectable product used to euthanize animals (Figure 1).
External Examination at the Death Scene
An examination of the death scene was conducted by a forensic doctor and a lab technician of the federal police. The deceased woman was found lying on an inflatable camping mat. A catheter was inserted in the radial aspect of the left forearm, connected to a nearly empty infusion bag containing 500 mL of Ringer’s lactate. The infusion bag was hanging from a beam on the wall via a long infusion line, with the drip regulators fully opened.
Distal to the catheter insertion site, the skin showed an irregular linear pink discoloration. The left upper arm exhibited the same type of discoloration, but with a more intense reddish hue and a dark brown discoloration of the skin between some of the red lines, consistent with necrosis (Figure 2). The discoloration patterns appeared to follow the subcutaneous blood vessels. Apart from the puncture wound caused by the catheter, no additional punctures wounds were observed, leading to the conclusion that the product was administered via the infusion bag. The postmortem interval was estimated to be between 13.5 and 22.5 hours based on the temperature-based method of Henssge.

Autopsy Findings
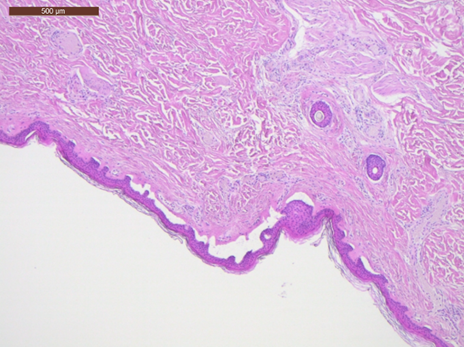
Due to the presumed unnatural cause of death, a forensic autopsy was performed the following day at the ISO- 17020-accredited academic forensic institute of UZ Leuven, accompanied by the lab technician of the federal police [9, 10]. According to the internal guidelines of the institute, a postmortem CT scan was performed prior to the autopsy to exclude air embolism. The medical imaging disclosed no significant findings. The autopsy revealed the body of a young female of normal build (166.5 cm, 64 kg, BMI 23 kg/ m2). The postmortem interval at the time of the autopsy was estimated to be approximately 37 to 46 hours. The vessel markings observed at the death scene were still clearly visible but the necrotic skin now demonstrated noticeable blister formation (Figure 3). The underlying subcutaneous fat and muscle tissue showed no macroscopic abnormalities. Histopathological examination of the skin lesions presented subepidermal blister formation and autolysis of the dermis, but no cellular reaction (Figure 4).

Other relevant autopsy findings included foam in the upper airways, mild cerebral edema with mild cerebellar herniation (brain weight: 1172 g), pulmonary edema (right lung 643 g, left lung 518 g) and congestion of the visceral organs, findings that are consistent with a comatose death. No significant pre-existing diseases were identified.
Toxicological analysis
A comprehensive toxicological analysis was performed on femoral blood (collected in a sodium fluoride tube) and urine samples obtained during the autopsy, using ultra-high- performance liquid chromatography coupled with mass- spectrometry detection. The relevant toxicological findings results are summarized in Table 2. The contents of the infusion bag were not analyzed.
| Product | Femoral blood concentration | Urine concentration |
|---|---|---|
| Pentobarbital | > 10 mg/L | Confirmed but not quantified |
| Midazolam | 32 ng/mL | 113 ng/mL |
| Ketamine | 5950 ng/mL | 95300 ng/mL |
| Trazodone | Trace | 830 ng/mL |
| Alcohol | 0.85 g/L | 1.06 g/L |
Table 2: Results of the Toxicological Analysis.
Summary of Medicolegal Conclusions
The final autopsy report concluded that this 27-year-old veterinarian died as a result of an overdose of intravenously administered pentobarbital, combined with alcohol and (potentially also intravenously administered) ketamine, midazolam, trazodone. Since the stomach content and the contents of the infusion bag were not analyzed, it is not possible to determine which products were ingested and which products were intravenously administered. Based on the circumstances and the death scene investigation the manner of death was determined to be suicide. As a veterinarian, this woman had easy access to the drugs used and had the knowledge regarding the required doses and administration [11].
Literature Review
Methods
A literature review was performed using PubMed for the search of cases describing suicidal pentobarbital intoxication.
The following terms were used: “pentobarbital” AND “autopsy”, “pentobarbital” AND “suicide”, “pentobarbital” AND “injection” AND “suicide”, “pentobarbital” AND “poisoning” and finally “barbiturates” AND “blisters”. Only publications from the last 25 years (1999-May 2024) were included. The eligible publications were reviewed to gather information on demographics, method of administration, external injuries and toxicology results.
Additionally, the database of the Department of Forensic Medicine at UZ Leuven (DaFor) was searched for cases of suicidal intoxication with pentobarbital over the past ten years using the term “pentobarbital”.
Results PubMed
The literature search resulted in 12 eligible articles describing 11 cases of pentobarbital intoxications and 1 phenobarbital intoxication. The most relevant information from these cases is summarized in Table 3.
| Author and year | Sex and age | Profession | Other relevant information | Method of administration | External lesions | Maximum pentobarbital concentration (µg/mL) | Other toxicology results |
|---|---|---|---|---|---|---|---|
| Fink T, et al. [12] | 31y, F | Medicine student | Prior suicide attempt | IV infusion | Blisters and necrosis left arm | 0.32 µg/mL (PB) but higher in blister fluid | thiopental (5.35 µg/mL) |
| Romain N, et al. [13] | 51y, M | Works for the society for the prevention of cruelty to animals | Farewell letters | Abdominal injection | 2 abdominal puncture wounds | 13.5 µg/mL (PB) | / |
| Brandt- Casadevall C, et al. [14] | 65y, M | Cardiologist | / | Oral | No injuries mentioned | 21.4 mg/L (PB) | / |
| Keng M, et al. [10] | 29y, F | Not mentioned | Bipolar disorder and borderline personality disorder | Oral | Bullae on hands, back and right heel | Phenobarbital: 6.1 µg/mL | THC, benzodiazepines |
| Melo P, et al. [15] | 37y, M | Salesperson | / | Oral | No injuries mentioned | 111 µg/mL (CB) | ethanol, diazepam, nordiazepam, oxazepam, temazepam, metoclopramide |
Table 3: Demographics and Other Relevant Patient Information, Method of Administration, External Injuries and Toxicology Results
phenytoin,
- Veterinarian
- Injected in the left antecubital
- Crellin SJ, et al. [16]
- 48y, F
- Not mentioned
- Compartment
- 12.6 µg/mL spouse, suicide note syndrome (PB) fossa
- 4 abdominal
- Former veterinarian’s
- 36 mg/L (PB)
- Hangartner
- S, et al. [17]
- 65y, F
- /
- Injection in the abdominal wall puncture wounds with and 15 mg/L assistant (CB) necrosis
- Druda DF,
- 45y,
- Not mentioned
- Bipolar disorder
- Oral
- No injuries mentioned
- 116 µg/mL (PB)
- / et al. [18]
- M
- Katz KD, et al. [19]
- 94y, F
- Not mentioned
- /
- Oral
- No injuries mentioned
- 9.5 µg/mL secobarbital
- Puncture wound above the umbilicus
- Nakayama
- R, et al. [20]
- 73y,
- M
- Veterinarian
- /
- Injection in the abdominal wall
- 4.93 µg/mL (PB)
- Suffered from ALS, requested euthanasia
- Shintani-
- Ishida K, et
- Gastrostomy
- F,
- ~50s
- Not mentioned
- No injuries mentioned
- 53.8 µg/mL tube (suspected)
- (PB) al. [21]
- Suicidal ideation, borderline personality
- Koizumi Y, et al. [22]
- 21y, F
- Not mentioned
- Oral
- Laceration on left wrist
- 16.6 µg/mL
- / disorder
Table 4: Demographics and Other Relevant Patient Information, Method of Administration, External Injuries and Toxicology
Results DaFor
According to the digital database, the forensic physicians at the Department of Forensic Medicine at UZ Leuven performed 6.400 external postmortem examinations in the past ten years (May 2014-May 2024).
Eight of these cases, excluding the case above, where labeled as suicide by intoxication with pentobarbital. The temporal distribution of cases was as follows: one case each time in 2014, 2015, 2016, 2017, 2019 and 2021 and two cases in 2018.
The age of the deceased ranged from 25 to 74 years. Two were female and six were male. In four cases the profession of the deceased was known: one was an active veterinarian, one was a retired veterinarian, one was a pharmacist, and one was a PhD student in biomedical sciences.
In six cases, the pentobarbital was taken orally. This conclusion was made based on the absence of puncture wounds. In one case, the product was administered through intradermal injection (puncture wound in de the right antecubital fossa).
In another case, concerning a 35-year old female veterinarian, an IV infusion was present in de left arm and both medial ankles. Only in this last case, with evidence for intravenous administration, the characteristic marbling, blisters and dark discoloration of the skin were described around the infusion sites (Figure 5). There are no indications that she had taken or administered any other medications.

In all of the cases the conclusion of suicide was made based on the circumstances. In six cases, farewell letters were found at the scene and in four cases, the deceased had a known history of depression or had previously attempted suicide.
When combining the cases from Table 3 and the Department of Forensic Medicine at UZ Leuven, we can conclude that all 21 cases describe suicidal intoxications with barbiturates, most often pentobarbital. The majority (13 cases or 61,9%) involve oral intake of the drug. In only 3 cases (14,3%) the drug was administered through IV lines. It is striking that in all these cases the skin showed the characteristic lesions. In the remaining 5 cases (23,8%), the barbiturate was injected subcutaneously. In only one of these cases, necrosis around the puncture wound was observed.
Discussion
Publications on barbiturate auto-intoxications are predominantly descriptive case reports, while reviews covering multiple cases are rather scarce. This paper aims to identify common factors within these intoxication cases to explain the observed skin lesions. It is crucial to differentiate these lesions from the well-known coma blisters which are observed in approximately 6% of comatose patients with a barbiturate overdose and exhibit a pathognomonic microscopic finding of sweat gland necrosis [10].
As mentioned, only three of these cases, including that of our 27-year-old veterinarian, exhibited specific skin lesions best described as blister formation combined with necrosis and a reddish marbling effect. Firstly, the only substance identified in each of these cases was a barbiturate. This strongly suggests that this drug is responsible for the observed skin lesions. The other substances found in the 27-year-old veterinarian (e.g. ketamine and midazolam) do not appear to be relevant in this regard. Other articles describing these specific skin lesions as a result of a ketamine or midazolam, were not found.
The second common factor in the three included cases is the observation that the marbling lesions exclusively occur after intravenous administration of the drug. No articles have described these specific lesions following oral ingestion. One case report describes necrosis around a puncture wound in the abdominal wall after subcutaneous administration of pentobarbital, but the typical marbling is absent. Therefore, this external observation could be considered a pathognomonic postmortem sign for intravenous barbiturate administration. In cases where the used product cannot be identified immediately (e.g. no product packaging present) these typical skin lesions can be an important lead for forensic investigators.
Thirdly, the marbling is not limited to the area around the injection site. In all three cases, it spreads throughout almost the entire limb, both proximal and distal to the injection site. The exact origin of these skin lesions remains uncertain. Tissue irritation (caustic effect) and endothelial necrosis are known adverse effects of intravenous administration of pentobarbital, but the observed skin lesions of the three post mortem cases have not been described in living or comatose patients [7], nor have they been documented in animals where pentobarbital is frequently used in high doses. A plausible hypothesis that is proposed is that, postmortem, the cessation of circulation allows the administered product to cause local damage to the vessel wall, resulting in extravasation into the surrounding skin tissue, causing necrosis and blistering. This damage to the vessel wall could also explain the marbling effect. The chemical structure of barbiturates likely contributes to the appearance of the skin lesions. Borodkin et al. described that barbiturates require a high pH-level to remain soluble [11]. In aqueous solutions, the substance crystallizes which may lead to tissue damage.
Fink T, et al. [12] measured pentobarbital concentrations in peripheral blood and in blister fluid finding higher concentrations of pentobarbital in the blister, suggesting extravasation following circulatory failure [12].
While abnormalities in the blood vessel walls would be expected in microscopic examination, the histopathological analysis of skin tissue of the 27-year old veterinarian only showed subepidermal blistering and autolysis with no apparent vascular damage. However, a sampling error must be taken into account. Unfortunately, histopathological examination was only performed in the aforementioned case. As a result of this limitation, no definitive conclusion can be drawn on this matter. In future studies, microscopic examination should be incorporated to help confirm the proposed hypothesis of vascular damage.
Lastly, it is essential to distinguish these lesions from the marbling seen in decomposition. To confirm that these lesions are caused by barbiturates and not decomposition based on external examination, no other signs of decomposition should be present, and the postmortem interval should be relatively short. As decomposition progresses, distinguishing these lesions from decomposition-related marbling can be expected to become increasingly difficult.
A potential notable limitation of this review is the limited number of cases. A larger multi-center study would strengthen future validation of the specificity for pentobarbital intoxications and the suggested hypothesis.
Conclusion
Suicidal auto-intoxications with pentobarbital are rare in the general population but occur more frequently in the field of veterinary medicine. A definitive diagnosis of barbiturate overdose requires autopsy and toxicological analysis. This article provides valuable forensic insights into the characteristic skin lesions associated with intravenous pentobarbital administration, highlighting their potential as a pathognomonic postmortem sign to aid forensic investigations.
Statements and Declarations
The first draft of the manuscript was written by Iris Van Deuren. All authors commented on previous versions of the manuscript and read and approved the final manuscript.
There are no relevant conflicts of interest to disclose. No funds, grants, or other support was received.
This case report is based on a medicolegal autopsy. Written informed consent for publication of the reported clinical details and images was obtained from the mother of the patient and approval by the public prosecutor was granted. A copy of the written consent is available for review by the editor of this journal. All included procedures were performed according to the legal standards of the institution.
Ethical approval was not required for this study.
References
-
World Health Organization (2024) Suicide. WHO, Fact sheets.
-
Milner A, Witt K, Maheen H, LaMontagne AD (2017) Access to means of suicide, occupation and the risk of suicide: A national study over 12 years of coronial data. BMC Psychiatry 17(1): 1-7.
-
Fink-Miller EL, Nestler LM (2018) Suicide in physicians and veterinarians: risk factors and theories. Curr Opin Psychol 22: 23-26.
-
Milner AJ, Niven H, Page K, Lamontagne AD (2015) Suicide in veterinarians and veterinary nurses in Australia: 2001-2012. Aust Vet J 93(9): 308-310.
-
Solbeck P, Snowdon V, Rajagopalan A, Jhirad R (2019) Suicide by Fatal Pentobarbital Intoxication in Ontario, Canada, from 2012 to 2015. J Forensic Sci 64(1): 309- 313.
-
Nitschke P, Stewart F (2019) The Peaceful Pill Handbook. Amazon.
-
Johnson AB, Sadiq NM (2024) Pentobarbital. StatPearls, NCBI Bookshelf.
-
Regenthal R, Krueger M, Koeppel C, Preiss R (1999) Drug levels: Therapeutic and toxic serum/plasma concentrations of common drugs. J Clin Monit Comput 15(7-8): 529-544.
-
Van Den Bogaert W, Wuestenbergs J, Bekaert B, Dequeker E, et al. (2024) Enhancing postmortem diagnostics: over a decade of ISO 17020 accreditation and guidelines implementation in forensic pathology. Forensic Sci Med Pathol.
-
Keng M, Lagos M, Liepman MR, Trever K (2006) Phenobarbital-Induced Bullous Lesions in a Non- Comatose Patient. Psychiatry (Edgmont) 3(12): 65.
-
Borodkin S, Lowell M, Thompson G, Schmits R (1977) No TiStable Nonaqueous Pentobarbital Sodium Solutions for Use in Laboratory Animalstle. J Pharm Sci 66(5): 693- 695.
-
Fink T, Röhrich J (2000) Skin blistering due to local barbiturate effects in the early postmortem phase. Rechtsmedizin 10: 187-190.
-
Romain N, Giroud C, Michaud K, Mangin P (2003) Suicide by injection of a veterinarian barbiturate euthanasia agent: Report of a case and toxicological analysis. Forensic Sci Int 131(2-3): 103-107.
-
Brandt-Casadevall C, Krompecher T, Giroud C, Mangin P (2003) A case of suicide disguised as natural death. Sci Justice J Forensic Sci Soc 43(1): 41-43.
-
Melo P, Costa P, Quintas MJ, Castro A, Tarelho S, et al. (2016) Pentobarbital in the context of possible suicides: Analysis of a Case 274: 109-112.
-
Crellin SJ, Katz KD (2016) Pentobarbital Toxicity after Self-Administration of Euthasol Veterinary Euthanasia Medication. Case Rep Emerg Med, pp: 1-4.
-
Hangartner S, Steiner J, Dussy F, Moeckli R, Gerlach K, et al. (2016) A suicide involving intraperitoneal injection of pentobarbital. Int J Legal Med 130(5): 1217-1222.
-
Druda DF, Gone S, Graudins A (2019) Deliberate Self- poisoning with a Lethal Dose of Pentobarbital with Confirmatory Serum Drug Concentrations: Survival After Cardiac Arrest with Supportive Care. J Med Toxicol 15(1): 45.
-
Katz KD, Koons A, Makar G, Wier A (2021) Old and Cold: A Novel Case of Combined Secobarbital and Pentobarbital Poisoning in an Elderly Woman. Cureus 13(1): e12446.
-
Nakayama R, Sato H, Yama N, Ogura K, Kyan R, et al. (2022) A suicide attempt by intramuscular injection of pentobarbital sodium into rectus abdominis suggested by computed tomography. Forensic Sci Med Pathol 19(2): 198-201.
-
Shintani-Ishida K, Idota N, Tsuboi H, Tsurumi R, Ikegaya H (2022) Pentobarbital overdose: A case of contract killing. Leg Med 59: 102149.
-
Koizumi Y, Higashitani M, Fukui S, Kodama T, Ito H, et al. (2023) A Case of Barbiturate Poisoning From Pentobarbital in a Young Japanese Patient. Cureus 36498.
- Forensic Implications of Adverse Drug Reactions in Schizophrenia A Case Series
- Narcotics and Digital Forensics: Bridging Crimes in the Digital Age
- Ethics in Forensic Psychiatry: Principles, Dilemmas, and Human Rights
- Impact of Acute Stress on Attentional Orienting to Social Cues
- Head Injury and Intracranial Hemorrhage in Western Region of Libya
- A Forensic Study on Handedness: Examination of Handwriting Features in Right and Left Handed Writers