Prognostic Factors for Soft Tissue Sarcomas of the Extremitie
Introduction: Soft tissue sarcomas (STS) are malignant tumors of mesenchymal origin that originate in any connective tissue or body support tissue. They represent 1% of all adult malignancies and are much less common than benign tumors developed in the soft tissue. Objective: The objective of the study is to analyze the factors influencing the prognosis of soft tissue sarcomas. Materiel and Methods: This is a retrospective cohort study of 50 cases of soft tissue sarcomas over a period of 05 years. The average age of the patients is 50 years, with a sex ratio of 01. The average consultation time is 22 months following the auto palpation of a mass gradually increasing in size. The MRI was performed on 37 patients or 74%. Surgical biopsy was performed on 75% of our patients. The predominant histological type was synovialosarcoma in 32% of cases, followed by lympsarcoma which accounted for 28% of cases. High grades (II and III) are the most common and accounted for 50%. Margins of exeresis were R0 in 12% of cases, R1 in 24%, R2 in 8% and unspecified in the rest. 56% of patients underwent conservative surgery, 20% underwent radical surgery and 24% were not operated on due to the stage of the disease. Results: The evolution shows 30% of local recurrences revealed on MRI and 26% of metastases, mainly pulmonary metastases. The adverse prognostic factors for local recidivism were as follows: tumor size >10 cm, the depth of the tumor, the histological grade, margin status, failure to administer adjuvant radiotherapy. Unlike local control, which was affected by many factors, metastatic recurrence was determined by only four independent factors: the depth of the tumor relative to the fascia; the size of the tumor, the grade of the tumor, and the histopathology. Conclusion: The improvement of patients’ quality of life, and therefore their prognosis, depends firstly on treatment from the outset in order to reduce the risk of local recurrence and iterative surgery, and secondly on increasingly functional surgery, hence the importance of multidisciplinary management in a specialised environment.
Introduction
Soft tissue sarcomas (STS) are malignant tumours of mesenchymal origin that originate in any connective or supporting tissue of the body [1]. They present 1% of malignant tumours in adults and are much less frequent than benign tumours developed in soft tissue [2]. The incidence of soft-tissue sarcomas increases with age. Two-thirds of soft- tissue sarcomas are localized to the limbs. In descending order of frequency, they affect the lower limbs and then the upper limbs [2]. No formal etiology is recognised to date, but several intrinsic favorable factors (mutations notably in the genes: NF1RB1, WRN, p53, APC, respectively responsible for neurofibromatosis type I, congenital retinoblastoma and Li-Fraumeni, Gardner and Werner syndromes) or extrinsic (exposure to ionizing radiation, vinyl chloride, dioxin, chlorophenol, certain viruses ...) have been identified [3]. Their diagnosis is said to be difficult.
The essential risk is to initially misunderstand it, leading to inappropriate “drainage on a haematoma diagnosis, liposuction, and enucleation” gestures that may compromise a subsequent conservative treatment. An imaging assessment, in particular an MRI and especially a preoperative biopsy are therefore necessary to adapt the therapeutic approach [2, 3, 4, 5, 6, 7, 8, 9, 10]. The treatment of soft tissue sarcomas (STS) of the limbs is currently based on conservative surgery combined with radiotherapy, the aim being to preserve maximum function while ensuring optimal carcinological safety. Chemotherapy finds its place in locally advanced and/or high-grade malignant tumors with high metastatic potential. The great difficulty of treatment lies in the balance between function and safety, which is defined for each patient by the regional multidisciplinary consultation meetings [11].
Methodology
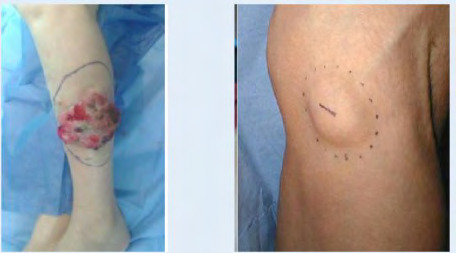
The objective of our work is to identify the factors influencing the prognosis of soft tissue sarcomas of the extremities on the local and remote control plane. This is a retrospective cohort study of 50 patients, treated for soft tissue sarcomas of the extremities at the oncology center of the Hassan II University Hospital of Fez over a 5-year period from 2013 to 2017. The age of our patients ranged from 17 to 86 years old with an average of 50 years old. The peak frequency was between 31 and 45 years of age, with 13 cases (26%). In our series the sex ratio of STS is 1. Patient consultation times ranged from 1 to 60 months (5 years), with an average of 22 months. This tumour is mainly located in the lower limbs with 38 cases (76% of the population studied), including 56% in the thigh. Topography of the upper limb is noted in 12 cases (24% of patients) (Figures 1-4). The discovery by the patient of a mass in his limb, which progressively increases in volume, is the main symptom that leads him to consult. It is found isolated in 54% of patients with STS (27 cases). Other signs were found: Pain in 11 cases, a nodule in 06 cases, functional impotence in 3 cases, alteration of the general state in 02 cases, pathological fracture in 01 case. At the intake clinical examination; the tumour mass ranged in size from 3 to 30 cm. It was noted that 78% of patients (39 cases) presented with bulky swellings, while only 22% (11 cases) consulted for masses of less than 5 cm. Our series of studies shows that in 76% of sarcomas were deep-seated, while only 24% were shallow-seated (Figure 5).





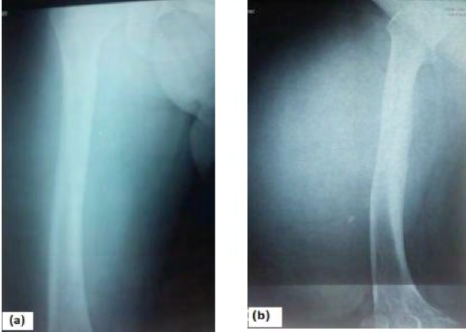
Neurological examination was normal in almost all patients, tingling along the path of the sciatic nerve was found in only one patient. 03 patients had a decreased femoral pulse on the unilateral side. Inguinal lymphadenopathies were also noted in 2 cases. Standard radiography of the affected limb was requested in all patients included who objectified : Intralesional calcifications in 06 cases, rounded images with blurred limits in 15 cases, osteolysis in 03 cases, normal radiography in the remaining patients (Figure 6). In our series, 03 patients benefited from an ultrasound scan of the soft tissues of the affected area, which revealed: hypoechogenic mass, homogeneous of 6.4*4.7 cm of deep localization evoking a lipoma, hypoechogenic formation with a cystic appearance of 03 cm, cloisonne hematoma (Figure 7).
CT scan of the affected limb was performed on 10 patients. It was used to study: the density of the mass, enhancement after injection of the contrast material, vascularization, shape and contours, bone ratios (Figure 8). Magnetic resonance imaging (MRI) was performed on 37 patients, or 74%. On T1 sequences, MRI lesions appear as Hyposignal in 52% of cases, Hypersignal in 15% of cases, isosignal in 20% and variable in the remaining cases. On T1 sequences, lesions appear as Hypersignal in 90% of cases, variable in 10% of cases. In our series, almost all the MRI lesions had intense and heterogeneous enhancement, however, one case was noted as having both sheet and linear enhancement, one case weak enhancement, one case no enhancement (Figures 9-12). The biopsy was performed on all our patients: In 72% of cases, a surgical biopsy was performed, while 04 patients in our series benefited from an image-guided biopsy, i.e. 8%. In 01 patient, the diagnosis was made on percutaneous biopsy. In 7 cases the diagnosis was confirmed on surgical specimen. There was discordance between the biopsy results and the excisional specimen in 03 cases, concerning the histological type (Table 1).
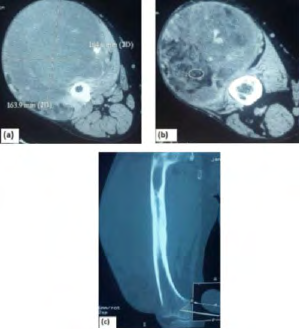
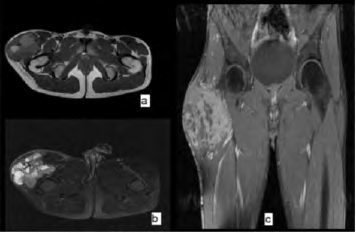
Figure 9: MRI of the right thigh in sections (a) coronal T1 (b) coronal T2 FAT SAT (c) sagittal T1 C+ showing the presence at the vastus lateralis of the right quadricipital muscle of a heterogeneous polylobed mass, containing tissue areas described as discrete hyposignal T1 hypersignal T2 and other haemorrhagic areas as hypersignal T1, hypersignal T2 not disappearing on the FATSAT sequence. It measures: 11x10x10 cm in diameter. Topographically: it infiltrates adjacent muscles in contact with the femoral neck diaphysis, without lysis or bone signal abnormalities.
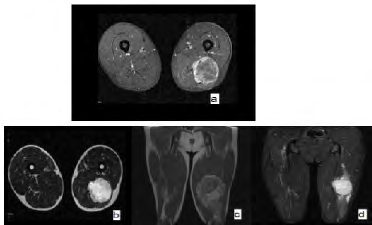
Figure 10: MRI of the left thigh in sections: (a) frontal T1 C+ (b) frontal T2 (c) sagittal T1 (d) T2 FATSAT showing the presence at the left posterior crural compartment at the inter-aponeurotic compartment and in the path of the great sciatic nerve of a tissue formation described as hyposignal T1, hypersignal T2, unmodified in FATSAT sequence, heterogeneously and intensely enhanced after contrast. It is encapsulated, lobulated in contour and maintains clear interfaces with the surrounding muscles.
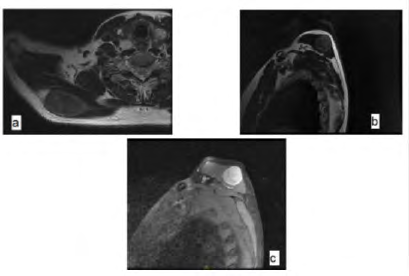
Figure 11: MRI of the right shoulder in sections (a) coronal T1 (b) sagittal T2 (c) sagittal T1C+ showing the presence in the posterior region of the right scapula at the expense of the great dorsal muscle of a rounded, well circumscribed tissue mass measuring 52x32x33mm, described in hypersignal T2 and STIR, iso T1, significantly enhanced after injection of Gadolinium.
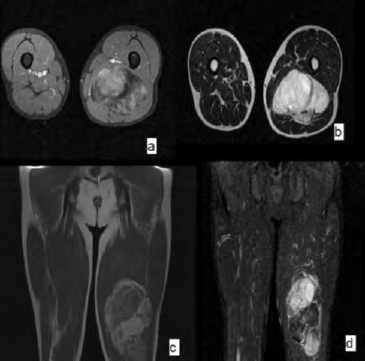
Figure 12: MRI of the left thigh in section (a) coronal T1 C+ (b) coronal T2 (c) sagittal T1 (d) sagittal C+ FATSAT showing the presence of a voluminous mass of the lower half of the posterior compartment of the left thigh appearing to develop intermuscularly at the dependency of the semimembranous muscle and the well limited biceps femoral measuring 165x68x155mm with polylobate partitioned contours. This mass is tissue containing a fat contingent and necrotic areas.
| Preoperative Histology | Post-Operative Diagnosis |
| Myxofibrosarcoma | FERRIER FERAND Dermatosarcoma |
| Chondrosarcoma | Osteoblastic osteosarcoma |
| Swanoma | Liposarcoma |
Table 1: Discordance between pre-and post-operative histology.
As part of the remote extension assessment, a thoraco- abdomino-pelvic CT scan was performed in 40 patients and was objective: pulmonary nodule and micronodule in 13 patients, pleural nodule with pleural effusion in 03 patients, suspicious-looking liver lesions in 04 patients, suspicious-looking bone lesions in 02 patients, spinal lesions in 02 patients, metastatic ADP in 02 patients, metastasis in contralateral limb in 01 patient.
Results
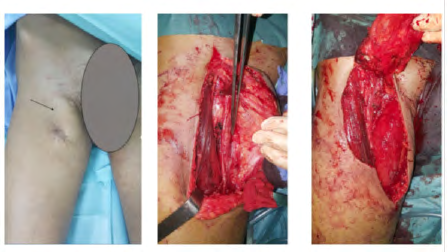
The majority of our patients present with synovialosarcoma. The anatomopathological study made it possible to study the histological grade in 29 patients, i.e. 58% (Table 2). An immuno-histochemical study was performed in 29 patients confirming the histological diagnosis. The technique of molecular biology: fluorescence in situ hybridization [FISH], was used in 13 patients. Surgical specimen removal margins were studied in 22 patients (Table 3). Patients included received conservative or mutilating surgical treatment, depending on the stage, grade and general condition of the patient (Figures 13-16). In our series 28 patients received conservative surgical treatment as shown in Table 4. In addition, 10 patients benefited from radical treatment (Table 5). 12 patients did not benefit from surgical treatment due to the stage of the disease. 09 patients underwent revision surgery: either as part of a recurrence or as part of a tumour bed revision due to the unhealthy R2 margins of the first surgery. 06 of them received conservative treatment (Table 6).
| Grade I | Grade II | Grade III | Unspecified | |
|---|---|---|---|---|
| Number of cases | 4 | 14 | 11 | 21 |
| Margin States | R0 | R1 | R2 | Unspecified |
| Number of cases | 6 | 12 | 4 | 28 |
Table 2: Classification of STS by histological grade.
| Intracapsular excision | Marginal excision | Large excision | Compartimentectomie | |
|---|---|---|---|---|
| Number of cases | 2 | 11 | 11 | 4 |
| percentage | 4% | 22% | 22% | 8% |
Table 3: Data of patients who have undergone revision surgery.
| Amputation | Disarticulation | |
|---|---|---|
| Number of cases | 7 | 3 |
| percentage | 14% | 6% |
Table 4: Data of patients who have undergone revision surgery.
| Primary Surgery | Surgical revision | ||||||
|---|---|---|---|---|---|---|---|
| type | diagnosis | Grade | Margin | type | diagnosis | Grade | Margin |
| Marginal | Myxoid liposarcoma | I | R1 | Compartimentectomie | Myxoid liposarcoma | I | R1 |
| Marginal | synovialosarcoma | II | R1 | large | synovialosarcoma | II | R0 |
| Marginal | Myxoid liposarcoma | II | R1 | large | myxofibrosarcoma | II | R0 |
| Marginal | Dedifferentiated liposarcoma | - | R1 | amputation | Dedifferentiated liposarcoma | II | R0 |
| large | Leimyosarcoma | II | R0 | large | Leimyosarcoma | II | R0 |
| large | Leimyosarcoma | II | R1 | Compartimentectomie | Leimyosarcoma | II | R0 |
| Marginal | Leimyosarcoma | II | R0 | Disarticulation | Leimyosarcoma | II | R0 |
| large | synovialosarcoma | II | R0 | amputation | synovialosarcoma | II | R1 |
| Marginal | Swanoma | - | R0 | large | liposarcoma | - | R1 |
Table 5: Data of patients who have undergone revision surgery.


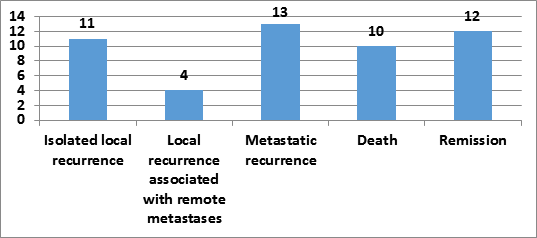
In our series, 12 patients or 24% required additional therapy by external radiotherapy. In all cases, the dose was 66 Grays in 33 fractions with a standard fractionation of 2Gy per fraction one session per day and 5 fractions per week spread over a period of 7 weeks. Chemotherapy was indicated in 26 patients or 52%. Neoadjuvant chemotherapy was given in 07 patients with locally advanced tumors and palliative adjuvant chemotherapy in 19 patients with secondary metastatic localization. Adjuvant and neo- adjuvant chemotherapy were given to 02 patients. The most commonly used therapeutic protocol is 3 courses of adriyamicin+ifosfamide administered with a split-dose regimen and continuous infusion. 02 patients benefited from 6 courses of adriyamicin+ifosfamide. 02 patients benefited from 03 courses of doxorubicin monotherapy and 02 patients benefited from ifosfamide monotherapy. Among the patients who received radiotherapy or chemotherapy, 7 cases or 14% received radiochemotherapy. After a mean decline of 19 months, 11 patients had local recurrences and 04 patients had metastatic recurrences. After an average decline of 19 months, the histogram in figure 16 represents the evolution of our patients.
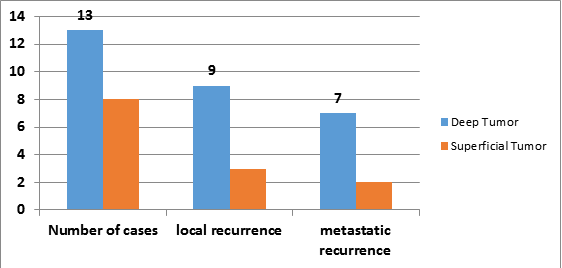
Regarding prognostic factors, the mean age of patients who experienced local recurrence and metastatic recurrence was 27 and 44 years, respectively. 50% of patients who developed a recurrence or metastasis had a tumour located in the lower limb precisely at the thigh. In patients who have developed tumour recurrence or metastasis; the size of the initial tumour ranges from 6cm to 20cm: 35% between 5cm and 10cm and 65% greater than 10 cm. In our study, there were only 21 complete MRI scans available to analyze the depth of the tumour; among 21 cases studied, 13 cases with a deep tumour and 08 cases with a superficial tumour were found, 09 out of 11 patients with a deep tumour developed a recurrence or metastasis, while 03 out of 08 patients with a superficial tumour had a recurrence (Figure 17).
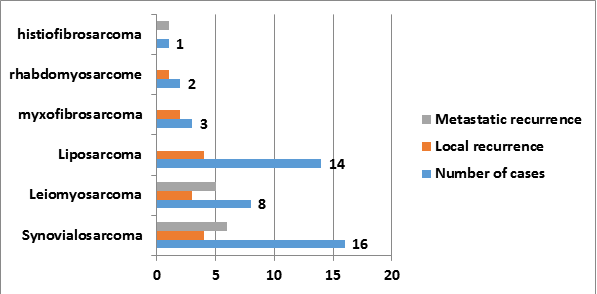
Synovialosarcoma was the histologic type associated with the greatest number of local or metastatic recurrences (Figure 18). Grade III was related to the greatest number of metastatic recurrences (Table 7). In our series; the majority of patients who developed a secondary localization had a typical conservative initial surgery: marginal excision, i.e. 73% (Table 8). Surgical specimen removal margins were studied in 22 patients, 75% of patients whose excision was R1 or R2 developed local recurrence and/or metastasis (Table 9). In our series, almost all patients who developed a secondary localization did not initially benefit from further treatment with either radiotherapy or chemotherapy or radiochemotherapy. 02 cases /22 cases received complementary treatment : 1st patient benefited from a neo-adjuvant CMT + adjuvant RTE, presented a pulmonary metastasis after 01 year, 2nd patient benefited from neo- adjuvant CMT + adjuvant RTE, presented a local recurrence after 06 months.
| Grade I | Grade II | Grade III | |
|---|---|---|---|
| Total number of cases | 4 | 14 | 11 |
| Number of cases with secondary location | 1 | 8 | 10 |
Table 6: Prognostic factors related to histological gr.
| Marginal excision | Large excision | Compartmentectomie | |
|---|---|---|---|
| Number of cases | 11 | 11 | 4 |
| Secondary location | 7 | 6 | 2 |
Table 7: Prognostic factors according to the type of excision.
| Margin States | R0 | R1 | R2 |
|---|---|---|---|
| Number of cases | 6 | 12 | 4 |
| Number of secondary locations | 2 | 9 | 4 |
Table 8: Prognostic factors based on margin status.
Discussion
Soft tissue sarcomas are rare [11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22], presenting 0.5-1% of adult malignancies with an estimated annual incidence of 3-8/100,000 [2]. At Fez University Hospital, STS represent 2.15% of all cancers diagnosed in the anatomopathology department [23]. Soft tissue sarcomas are a very heterogeneous group histologically, as more than 50 different histological types have been described, with some of the subtypes according to the latest WHO classification and frequent molecular heterogeneity [18]. All the studies performed showed a predominance of liposarcoma and a variation in the frequency of other histological types [5, 24, 25]. Our study showed that synovialosarcoma (30%) is the predominant histological type in our series, followed by liposarcoma (28%), leiomyosarcoma (16%), extra-skeletal Ewing’s sarcoma (6%), myxofibrosarcoma (6%), rhabdomyosarcoma (4%), chondrosarcoma (4%), histiofibrosarcoma (2%), pleomorphic cell sarcoma (2%) and Darrier and Ferrand dermatofibrosarcoma (2%) are less frequent (Table 10). The average age is around 50 years, but there are variations in incidence by age depending on histological type [26]. According to Suit et al, the occurrence of soft tissue sarcomas varies with age (approximately 55 years) [2, 27].
| Our series | Kransdorf [27] | Heymann [28] | Glelen [05] | c.elalouani [29] | |
|---|---|---|---|---|---|
| Synovialosarcoma | 30% | 5% | 7.80% | 6.50% | |
| Liposarcoma | 28% | 14% | 39.30% | 15.40% | 22% |
| Leiomyosarcoma | 16% | - | - | - | 7% |
| extra-skeletal Ewing’s sarcoma | 6% | - | - | - | - |
| myxofibrosarcoma | 6% | 5% | 5.60% | 2.40% | - |
| Chondrosarcoma | 4% | - | - | 2.40% | - |
| rhabdomyosarcoma | 4% | 1.90% | 5.60% | 5.60% | 11% |
| pleomorphic cell sarcoma | 2% | 24% | 5.60% | - | - |
| histiofibrosarcoma | 2% | - | - | - | - |
| Darrier and Ferrand dermato-fibrosarcoma | 2% | 6% | - | 3.20% | - |
| Swanoma | 2% | - | - | - | - |
| Unclassified sarcoma | 2% | - | - | - | 20% |
Table 9: Main adult STSs with their respective frequencies.
The results of our series are in line with those in the literature: The age of our patients ranged from 17 to 86 years with an average of 50 years. According to Chang and Sandak, nearly 60% of soft tissue sarcomas are located at the extremities, in order of decreasing frequency, they are of interest: the lower limbs “50%”, the deep regions of the trunk “mediastinum, retroperitoneum 20%”, the upper limbs “15%”, the trunk wall “10%” and head and neck “5%” [2]. Thus in our series of studies, the location of STS was in 84% at the level of the lower limbs (Table 11). The study of tumour location in relation to the superficial fascia shows that the frequency of deep tumours is higher than that of superficial tumours (96% versus only 4%) [28]. Our study is in line with the literature and objectively 76% of the deep tumors.
| Year of Study | Effective | Upper limb | Lower limb | |
|---|---|---|---|---|
| Heymann [2] | 1990-2003 | 89 | 15.70% | 58.50% |
| Milbéo [32] | 1996-2000 | 84 | 16% | 84% |
| Our series | 2012-2017 | 50 | 16% | 84% |
Table 10: Representation of STS locations in the different study series.
Biau, et al. [29] reported that age was significantly associated with local recurrence, while Gronchi, et al. [30] reported no association with local recurrence. Zagars GK, et al. [31] showed that the patient’s age (≤ 64 years vs> 64 years) had a relative risk of 1.8 (95% CI, 1.3-2.5, P < 0.001). Pisters PW, et al. [32] reported that age greater than 50 years is a poor prognostic factor for local recidivism. Bonvalot S, et al. [2] did not report the prognostic value of age in local recurrence. In our study: 40% of the patients with an age >50 years developed a local recurrence VS 30.7% of the patients <50 years. Comparing the percentages with a KHI2 test; age has no prognostic value in this study. Zagars GK, et al. [31] showed that the location of the tumour has a prognostic value on local recurrence, in decreasing order of significance: deep regions of the trunk, head and neck, upper extremities, superficial wall of the trunk, lower extremities, with a relative risk of 2.6 (95% CI 1.8-3.6; P < 0.001). In our series, the location of the STS was in 84% at the level of the lower limbs, 80% of which were at the level of the thigh; of these, half developed recurrence.
The value of the seat in local recurrence cannot be determined since only soft tissue sarcomas of the extremities have been treated. Zagars GK, et al. [31] found that tumour size had a relative risk of 1.7 (95% CI 1.2-2.4, P = 0.002). The 5- and 10-year control rates were as follows: ≤ 2 cm, 84% and 83% at 5 years and 10 years, respectively, 2 cm and ≤ 5 cm, 84% and 82% at 5 years and 10 years, respectively, 5 cm and ≤ 10 cm, 83% and 79% at 5 and 10 years, respectively, 10 cm, 77% and 73% at 5 years and 10 years, respectively. Pisters PW, et al. [32] showed that tumour size was one of the prognostic factors in distant recurrence. Coindre JM, et al. [12] and Andres Rydholm did not demonstrate the prognostic value of size in local recurrence. In our study patients who developed tumor recurrence, the size of the initial tumor ranged from 6cm to 20cm: 35% between 5cm and 10cm, 65% greater than 10cm. Therefore, our study is in line with the literature: a height greater than 10 cm is a prognostic value for local recurrence.
In our series of studies there were only 21 complete MRI reports available to analyze the depth of the tumor. Among 21 cases studied, 13 cases with a deep tumour and 08 cases with a superficial tumour were found. 9 patients/13 patients with deep tumours developed a recurrence, while 03 patients/08 patients with superficial tumours had a recurrence. Comparing the results by the KHI2 test we find that the depth of the tumour is significant as a prognostic factor. The histological type has a prognostic value according to: Gunar K, et al. [31] who considered histyofibrosarcomas, neurogenic sarcomas, and epitheloid sarcomas as a poor prognostic factor compared to other histological types. The
local control rates at 5 and 15 years were respectively: For neurogenic sarcoma: 76% and 71%, for epithelioid sarcoma: 65% and 65%, for leiomyosarcoma: 90% and 90%, for synovial sarcoma 88% and 84%; for liposarcoma 85% and 78%; for fibrosarcoma: 83% and 79%; for rhabdomyosarcoma: 80% and 80%; and for unclassified sarcoma, the corresponding rates were 83% and 83%. Pisters PW, et al. [32] also consider neurogenic sarcomas to be one of the significant adverse prognostic factors for local recurrence.
All studies show that histological grade has a very significant prognostic value on local recurrence. According to Zagars GK, et al. [31] the grade of the tumour had a relative risk of 1.5 (95% CI 1.1-2.2, P = 0.013). Coindre JM, et al. [12] consider histological grade as a prognostic factor for tumour recurrence (95% CI, P < 0.01). Our study is in line with the literature and shows that grade III has a significant risk of recurrence compared to other histological grades. The quality of surgical excision during initial treatment was the only factor consistently and significantly found in all studies involving multivariate analysis. Wide excision (local relapse rate of 5 to 15%) should be preferred over marginal excision which is always inadequate (50 to 90% local relapse), and a fortiori intracapsular excision which is nothing more than simple surgical biopsies. Current adjuvant treatments do not make up for poor quality surgery, and systematic resection of the tumour bed must be offered if the tumour was opened during the operation, if the surgeon did not consider that it could be a sarcoma prior to the operation, and if the removal is incomplete or marginal. Zagars GK, et al. [31] confirmed that the resection margin is a significant prognostic factor for local recurrence with a relative risk of 2.5 (95% CI, 1.9-3.3, P < 0.001). Pisters PW, et al. [32] cited the microscopically positive surgical margins as significant adverse prognostic factors for local recurrence in their studies of sarcomas. Coindre JM, et al. [12] found that among the causes of the development of local recurrence, poor surgery (local excision) had a very significant value (P<0.001). Anders Rydholm reported that the strongest predictor of local recurrence is the surgical margin reached.
In our study, 75% of the patients whose excision was R1 or R2 developed a local recurrence. According to Anders RYDHOLM adjuvant therapy reduces local recurrence which is the reason for surgery combined with radiotherapy. According to Coindre JM, et al. [12], the development of local recurrence depends on whether or not adjuvant radiotherapy is carried out (P = 3.6 x 10-6). Gunar K, et al. [31] compared radiotherapy and chemotherapy in the management of soft tissue sarcomas and their impact on local recurrence by demonstrating local control rates at 5 years and 15 years for 99 patients. Those who received simultaneous radiotherapy and chemotherapy had a control rate at 5 and 15 years of age (82% and 82% respectively). Patients who did not receive concomitant chemotherapy had a control rate (83% and 79% respectively, P = 0.993). Therefore, chemotherapy has no prognostic value in local recurrence.
Unlike local control, which was affected by many factors, metastatic recurrence was determined by only four independent factors: the depth of the tumor relative to the fascia; the size of the tumor, the grade of the tumor, and the histopathology. In most studies, size appears to be the relevant factor. Gustafson, & Peabody, et al. 1994, Coindre JM, et al. [12] and Pisters PW, et al. [32, 33]. It is considered an important determinant of metastatic outcomes in patients with intermediate- and high-grade STS. Although the traditional size threshold is 5 cm, very small tumours (≤ 2 cm) have a significantly lower metastatic potential than intermediate-sized tumours (> 2 cm and ≤ 5 cm). Intermediate-grade tumours (> 10 cm) had a metastasis rate of only 26% over 15 years, whereas high-grade tumours (> 10 cm) had a metastasis rate of 62% over 15 years (Tables 12,13). In our study the tumours ranged in size from 3 to 30 cm. 78% of patients (39 cases) presented with bulky swellings, while only 22% (11 cases) consulted for masses of less than 5 cm.
| 5-years MFSR | |||
|---|---|---|---|
| Size(cm) | 5-Jan | 0.8 | |
| 10-Jun | 0.6 | ||
| 15-Nov | 0.5 | ||
| >15 | 0.4 | ||
| Grade | І | 1 | |
| ІІ | 0.9 | ||
| ІІІ | 0.7 | ||
| ІV | 0.5 | ||
| Tumor Size | 5- Year metalistic control (%) | 15- Year metalistic control (%) | p value |
| ≤5 | 85 | 79 | <0.001 |
| >5 cm | 65 | 55 | |
| Immediate grade and size | |||
| ≤5 | 96 | 88 | 0.002 |
| >5 cm | 82 | 74 | |
| High grade and size | |||
| ≤5 | 82 | 75 | <0.001 |
| >5 cm | 57 | 45 |
Table 11: Prognostic factors for patients with localized soft-tissue sarcoma.
In patients who have developed metastasis; the size of the initial tumour varies between 6cm and 20cm: 35% between 5cm and 10cm, 65% greater than 10cm. There is a close correlation between tumour size and depth. According to Coindre JM, et al. [12], Pisters PW, et al. [32] the deep location is one of the unfavourable characteristics for the development of remote metastasis with a (P = 0.0013). Our study is in line with the literature, 60% of patients with a deep tumor have developed metastasis. Histopathology (unfavorable vs. favorable) had a relative risk of 1.4 (95% CI, 1.1-1.7, P = 0.006) which correlated independently with metastatic recurrence. The study by Gunar K, et al. [31] was based on univariate analysis, and allowed the selection of five unfavourable, highly metastatic histotypes: leiomyosarcoma, synovial sarcoma, neurogenic sarcoma, rhabdomyosarcoma, epithelioid sarcoma. For patients with leiomyosarcoma, the metastasis rates at 5 and 15 years were 64% and 57% respectively. For patients with synovial sarcoma, the respective rates were 62% and 53%. For patients with neurogenic sarcoma, the respective rates were 63% and 59%.
For patients with epithelioid sarcoma, the respective rates were 64%. For patients with rhabdomyosarcoma, the respective rates were 59% and 55%. According to JM Coindre, among the unfavourable characteristics for the development of remote metastasis grade 3 had a value (P = 4 x 10-12). S. Bonvalot et al. identified histological grade as the most important prognostic factor with 5-year survival rates of 90%, 60% and 35% for grades 1, 2 and 3, respectively. Gunar K, et al. [31] showed that the intermediate grade had a relative risk of 8.9 (95% CI: 1.2-64.1; P <0.001) and that high-grade tumours had a relative risk of 22.5 (95% CI, 3.2- 160.1; P <0.001). Tumour necrosis has often been reported as an important prognostic factor according to (Costa, et al. 1984, Mandard, et al. 1989, Lack, et al. 1989, Becker, et al. 1991, van Unnik, et al. 1993, Oda, et al. 1993, Gustafson 1994. Vascular invasion is another strong prognostic factor (Mandard, et al. 1981, Gustafson, 1994). Our study is in line with the literature and shows that grade III has a significant risk of metastasis compared to other histological grades.
Conclusion
STS are malignant tumours that are rare and whose prognosis may be worsened by inadequate management. The improvement of patients’ quality of life, and therefore their prognosis, depends firstly on treatment from the outset in order to reduce the risk of local recurrence and iterative surgery, and secondly on increasingly functional surgery, hence the importance of multidisciplinary management in a specialized environment.
Conflicts of Interest
The authors do not declare any conflict of interest.
Contribution of Our Study to Knowledge
As far as we know, no elaborate study on this subject is available in the Fez region.
References
-
Société canadienne de cancer (2012) Vue d’ensemble du sarcome des tissus mous Encyclopédie canadienne du cancer.
-
Bonvalot S, Vanel D, Terrier P, Pechoux CL, A Le (2004) Cesne Principles for the treatment of soft tissue sarcoma in adults.
-
Honoré C, Méeus P, Stoeckle E, Bonvalot S (2015) Soft tissue sarcoma in France in 2015: Epidemiology, classification and organization of clinical care. J Visc Surg 152(4): 223-230.
-
Coindre JM (2016) Comment classer un sarcome des tissus mous en 2006. Ann pathol 26(Suppl 1): 98-100.
-
Taieb S, Ceugnart L, Gauthier H, Penel N, Vanseymortier L (2006) Soft tissue sarcoma: role of imaging for initial diagnosis and treatment. Cancer Radiother 10(1-2): 22- 33.
-
Tzeng CW, Smith JK, Heslin MJ (2007) Soft tissue sarcoma: preoperative and postoperative imaging for staging. Surg Oncol Clin N Am 16(2): 389-402.
-
Holzapfel K, Regler J, Baum T, Rechl H, Specht K, et al. (2015) Local Staging of Soft-Tissue Sarcoma: Emphasis on Assessment of Neurovascular Encasement-Value of MR Imaging in 174 Confirmed Cases. Radiology 275(2): 501-509.
-
Collin F, Marty MG, Binh MBN, Coindre JM (2006) Soft tissue sarcomas: current data in the field of pathology. Cancer Radiother 10(1-2): 7-14.
-
Siebenrock KA, Hertel R, Ganz R (2000) Unexpected resection of soft-tissue sarcoma. More mutilating surgery, higher local recurrence rates, and obscure prognosis as consequences of improper surgery. Arch Orthop Trauma Surg 120(1-2): 65-69.
-
Davis AM, Kandel RA, Wunder JS, Unger R, Meer J, et al. (1997) The impact of residual disease on local recurrence in patients treated by initial unplanned resection for soft tissue sarcoma of the extremity. 66(2): 81-87.
-
Lintz F, Moreau A, Cassagneau E, Maillard O, Waast D, et al. (2008) Study of the margins after resection of soft- tissue sarcomas JUIN.
-
Coindre JM, Terrier P, Bui NB, Bonichon F, Collin F, et al. (1996) Prognostic factors in adult patients with locally controlled soft tissue sarcoma. A study of 546 patients from the French Federation of Cancer Centers Sarcoma Group. J Clin Oncol 14(3): 869-877.
-
Gosling JA, Harris PF, Whitmore I, PLT Willan Anatomie humaine: Atlas en couleurs, pp: 2-3.
-
https://www.slideshare.net/mandiradahal1/skin- anatomy
-
http://www.superetscelette.net/page/p19/
-
Robinson E, Bleakney RR, Ferguson PC, O’Sullivan B (2008) Oncodiagnosis Panel: Multidisciplinary Management of Soft- Tissue Sarcoma. Radio Graphics 28(7): 2069-2086.
-
Fletcher CDM, Unni KK, Mertens F (2002) World Health Organization Classification of tumours. Pathology and genetics of tumours of soft tissue and bone. Lyon: IARC Press.
-
Coindre JM (2003) Immunohistochemistry in the diagnosis of soft tissue tumours. Histopathology 43(1): 1-16.
-
Sorensen PH, Liu XF, Delattre O, Rowland JM, Biggs CA, et al. (1993) Reverse transcriptase PCR amplification of EWS FLI-1 fusion transcripts as a diagnostic test for peripheral primitive neuroectodermal tumors of childhood. Diagn Mol Pathol 2(3): 147-157.
-
Nagao K, Ito H, Yoshida H, Minimizaki T, Furuse K, et al. (1997) Chromosomal rearrangement t(11:22) in extra skeletal Ewing’s sarcoma and primitive neuroectodermal tumour analysed by fluorescent in siti hybridization using paraffin-embedded tissue. J Pathol 181(1): 62-66.
-
Trojani M, Contesso G, Coindre JM, Rouesse J, Bui NB, et al. (1984) Soft tissue sarcoma of adults, study of pathological variables and definition of histopathological grading system. Int J Cancer 33(1): 37-42.
-
Stoeckle E, Michota A, Henriques B, Sargos P, Honorée C, et al. (2016) Surgery for soft-tissue sarcomas of the limbs and trunk wall. Cancer Radiother 20(6-7): 657- 665.
-
Hafid I (2012) Registre Hospitalier Des Cancers Resultats Preliminaires Du Service D’anatomie Pathologiquechu Hassan Ii Fes (A propos de 5532 cas).
-
Heymann S, Jung GM, Simon P, Bergerat JP, Borel C, et al. (2007) Résultants à long terme d’une série de 89 patients suivis pour un sarcome des tissus mous traits par chirurgie conservatrice et 3 modalités d’irradiation post-opératoire Cancer/Radiotherapie 11(8): 443-451.
-
Elalouani C, Khouchani M, Sadek H, Rida H, Elkholti Y, et al. (2009) Profil épidémioclinique et évolutif des sarcomes des tissus mous dans le service d’oncologie radiothérapie du centre hospitalier universitaire Mohammed-VI Marrakech. Cancer/Radiothérapie 13(6- 7): 695.
-
Holzapfel K, Regler J, Baum T, Rechl H, Specht K (2015) Local Staging of Soft-Tissue Sarcoma: Emphasis on Assessment of Neurovascular Encasement-Value of MR Imaging in 174 Confirmed Cases. Radiology 275(2): 501- 509.
-
Suit HD, Russell WO, Martin RG (1975) Sarcoma of soft tissue: clinical and histopathologic parameters and response to treatment. Cancer 35(5): 1478-1483.
-
Clark MA, Fisher C, Judson I, Thomas JM (2005) Soft- tissue sarcomas in adults. N Engl J Med.
-
Biau DJ, Ferguson PC, Turcotte RE, Chung P, Isler MH, et al. (2011) Adverse effect of older age on the recurrence of soft tissue sarcoma of the extremities and trunk. J Clin Oncol 29(30): 4029-4035.
-
Gronchi A, Casali PG, Mariani L, Miceli R, Fiore M, et al. (2005) Status of surgical margins and prognosis in adult soft tissue sarcomas of the extremities: A series of patients treated at a single institution. J Clin Oncol 23(1): 96-104.
-
Zagars GK, Ballo MT, Pisters PW, Pollock RE, Patel SR, et al. (2003) Prognostic factors for patients with localized soft‐tissue sarcoma treated with conservation surgery and radiation therapyAn analysis of 1225 patients. Cancer 97(10): 2530-2543.
-
Pisters PW, Leung DH, Woodruff J, Shi W, Brennan MF (1996) Analysis of prognostic factors in 1,041 patients with localized soft tissue sarcomas of the extremities. J Clin Oncol 14(5): 1679-1689.
-
Coquard IR, Thiesse P, Vince DR, Chauvin F, Bobin JY, et al. (2004) Conformity to clinical practice guidelines, multidisciplinary management and outcome of treatment for soft tissue sarcomas. Ann Oncol 15(2): 307-315.
- Contribution of 18FDG PET in Atypical HORTON Disease
- Living Conditions, Healthy Practice and State of Households of a Town Rural in Colombia
- Background to the Health and Safety Regulation at Work in Colombia
- Risk Factors Psychology Workers Sena (Center for the Petrochemical Industry) Regional Bolívar, Colombia
- Diffuse Intense Pleural FDG Uptake with Smooth Thickening: A MARKER of Tuberculosis in Isolated Pleural Effusion
- Hypermetabolic Splenomegaly with Infarct in FDG PET/CT: A Clue to Scrub Typhus in PUO