Role of Salvia Miltiorrhiza Root Extract (Danshen) in Evaluation of Hibernating/Viable Myocardium: An Evidence Based Study; Utilizing Nuclear Imaging Technique
Background: Complementary and Alternate medicine (CAM) is gaining popularity these days especially in management of chronic illnesses. Salvia Miltiorrhiza Root Extract (Danshen) is one such option for chronic heart diseases. In this study NO3 and SMRE augmented resting scans were compared to see which one was superior in evaluating hibernating myocardium. Methods: Total of 30 patients was included in this hospital based, interventional study. They had ejection fraction 30% or less, with history of myocardial infarction in past. Informed consent was taken. Each underwent 3 studies, 1. Resting scan. 2. NO3 augmented resting scan (using standard protocol). 3. SMRE augmented scan, in which two capsules of SMRE were administered sublingually (in place of NO3). 20 mCi of Tc- 99m sestamibi was injected after 10 min, an hour prior to acquisition. Results: Data interpretation was done by using 17 segments nuclear model. Scan interpretation was done by two independent observers. Out of total 30 patient who underwent NO3 and SMRE resting scans, presence of viable myocardium was indicated in N=15 scans (50%), where N=8 (53.3%) showed improvement with SMRE alone, N=2 (13.3 %) had improvement with NO3 alone and the rest N= 5 (33.3%) demonstrated viability with both SMRE and NO3. Using Chi squared test, at P value < .05, SMRE came out to be better than NO3, for assessment of viable myocardium. Conclusion: SMRE can be utilized for diagnosis as well as management of hibernating Myocardium as it is clinically useful, safe as well as cost effective.
Shagufta Z Qureshi1* and Tabinda Z Qureshi2
Introduction
Any patient with chronic CAD can have hibernating / viable myocardium. This is suggestive of a condition where reduced coronary blood flow results in impaired contractility [1, 2]. Condition is worth studying as LV function in viable myocardium could be partially or completely restored with successful and timely re-vascularization. Radionuclide perfusion imaging (MPI) is a useful diagnostic technique to demonstrate the extent of viability. It has been observed that all the major hemodynamic functions including nutrient and oxygen supply, in response to variations in demand, are conducted in microcirculation [3].
Saliva miltiorrhiza root extract (SMRE) is a natural herb, commonly used in the treatment of cardiovascular disorder. It has tanshinones which can inhibit platelet inhibition. Biological actions of the compounds isolated from SMRE has shown its potential effect of attenuating microcirculatory disturbances, including anti oxidation, inhibition of adhesion molecules, platelet aggregation inhibition, mast cell inhibition, inhibition of apoptosis, and amelioration of the injury of many target organs including heart [4, 5, 6].
Keeping in view these facts, this study was conducted to detect hibernating myocardium in patients with known CAD and we also compared the results of NO3 augmented and SMRE augmented scan in order to find out the better imaging modality for assessment of viable myocardium.
Materials and Methods
It was a hospital based interventional study, conducted in Nuclear Cardiology Department, of Federal Government Polyclinic Hospital (FGPC), Islamabad, Pakistan. Inclusion Criteria for the study subjects were as under:
- Patients between 33-72 years of age, with history of CAD, with/without active cardiac complaints like chest pain or dyspnea.
- Patients with history of myocardial infarction in the past.
- Echocardiography showed EF 30% or less.
Subjects enrolled in the study after formal informed consent. All patients were referred from the Cardiology OPD after thorough history and complete physical examination. They were kept NPO on the day of study. Each underwent 3 studies: a) Resting scan. b) NO3 augmented resting scan (using standard protocol). c) SMRE augmented scan, in which two capsules of SMRE were administered sublingually (replacing nitrate) rest of the protocol was same as in NO3 augmented scan.
BP was recorded before and after NO3 and SMRE administration. 20 mci (740MBq) of Tc-99m sestamibi was injected in each study and all 03 studies, in each case, were conducted on three separate days. Acquisition was done, for 15minutes, in each study, on Siemen’s E.cam dual head Gamma Camera, one hour after isotope injection. A semi- quantitative interpretation was performed, using short axis and vertical long axis myocardial tomograms, utilizing 17 segments Nuclear Model. For each study 0-4 point scale perfusion defect interpretation was used [7] i.e. 0=Normal perfusion, 1=Equivocal, 2=Moderate decrease, 3=Severe decrease in radiotracer uptake, 4=absence of detectable radiotracer in the segment. Statistical inference was drawn using Chi squared test, considering P value as .05.
Results
It was a hospital based interventional study, conducted in Nuclear Cardiology Department of Federal Government Polyclinic Hospital (FGPC), Islamabad, Pakistan. In this 03 months study, a total of 30 patients (22 males, 8 females), age 33-72 years (mean age 52.5 years) were included. All of them had history of myocardial infarction in past, and most of them had some typical cardiac symptoms as shown in Table 1.
| No of Pt. | Age | Gender | Symptoms | Type of Myocardial Infarction |
|---|---|---|---|---|
| 1 | 56 | M | dyspnea | anteroseptal |
| 2 | 53 | M | yspnea | inferolateral |
| 3 | 48 | M | Chest pain | anteroseptal, inferolateral |
| 4 | 70 | F | dyspnea | anteroseptal |
| 5 | 58 | M | dyspnea | anterior wall |
| 6 | 45 | M | Chest pain | anteroseptal |
| 7 | 38 | M | No symptom | inferolateral |
| 8 | 52 | F | dyspnea | Inferior wall |
| 9 | 33 | M | Chest pain | anterior wall |
| 10 | 70 | M | No symptom | antero-apical |
| 11 | 65 | M | dyspnea | anteroseptal |
Table 1: Baseline data of Study Subjects Indicating Symptoms and Type of Infarct.
- 12
- 52
- M dyspnea anteroseptal
- 13
- 76
- M dyspnea inferolateral
- 14
- 58
- M dyspnea anteroseptal, inferolateral
- 15
- 72
- M dyspnea anteroseptal
- 16
- 62
- F
- Chest pain inferolateral
- 17
- 54
- M dyspnea inferolateral
- 18
- 47
- M dyspnea anterior wall
- 19
- 60
- F
- No symptom
- Inferior wall
- 20
- 58
- M
- Chest pain anteroseptal
- 21
- 59
- M
- No symptom inferior wall
- 22
- 67
- M dyspnea inferolateral
- 23
- 64
- F dyspnea anteroseptal
- 24
- 62
- M
- Chest pain anteroseptal
- 25
- 49
- F
- Chest pain anteroseptal, inferolateral
- 26
- 54
- M dyspnea anterior wall
- 27
- 51
- M dyspnea anteroseptal
- 28
- 63
- F
- Chest pain anteroseptal, inferolateral
- 29
- 51
- M dyspnea anterior wall
- 30
- 56
- F dyspnea inferior wall
Table 2: Baseline data of Study Subjects Indicating Symptoms and Type of Infarct.
Visual analysis of scan results was done by two independent observers. Total of 30 patients were studied, in which 15 patients didn’t show any viable myocardium, around the infarcted area. Presence of viable myocardium was noted in rest of the 15 patients.
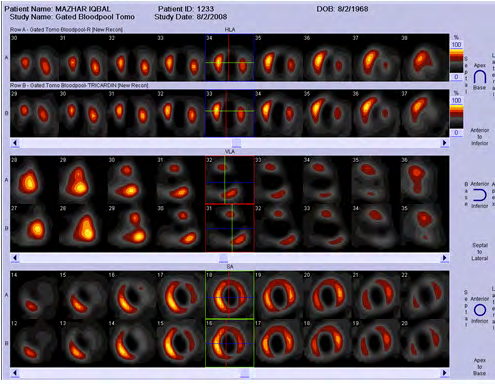
Improvement in myocardial perfusion was declared on the basis of predefined 0-4 point scale. N=8 scans (53.3%) showed improvement (presence of viable myocardium) with SMRE alone. N=2 (13.3%) had improvement with NO3 alone and the rest N= 5 (33.3%) showed improved perfusion with both SMRE and NO3. (Figure 1), shows a case, where SMRE as well as NO3 augmented scan didn’t show any evidence of viable myocardium surrounding the infarcted area, study one in the figure was conducted with NO3 and study 2 was with SMRE, both studies showed no improvement in perfusion.
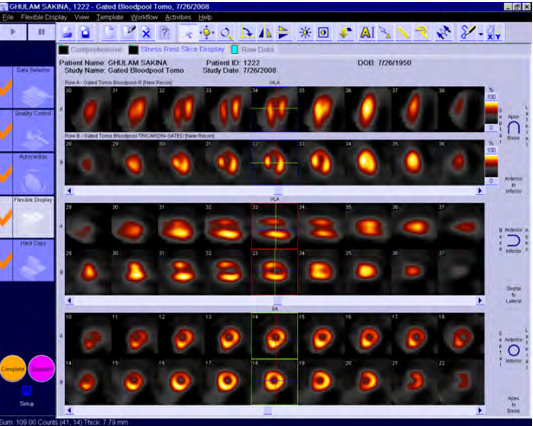
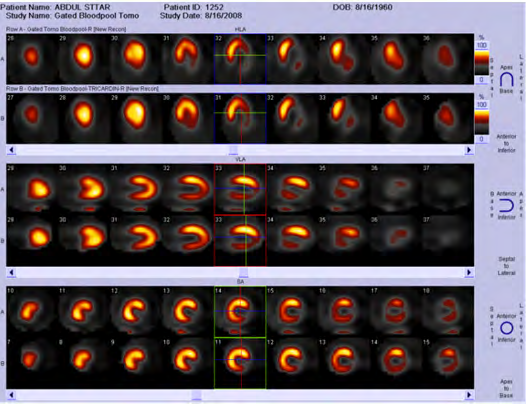
(Figures 2 & 3) demonstrate cases where viable myocardium was demonstrated by SMRE augmented scan, but not with NO3. Study 1 in the figure was conducted with NO3 and study 2 with SMRE.
Our null hypothesis was that “there is no difference between NO3 and SMRE when used in viability study”. The chi-square statistic was 7.2. The p-value came out to be .00729.
So the results were statistically significant at P < .05 and we had to reject our null hypothesis concluding that SMRE was better than NO3, for assessment of viable myocardium. Moreover no fall in systolic BP was noted with SMRE, which were a known side effect and a limitation with NO3 augmented imaging technique.
Discussion
Cardiovascular disease is one of the leading causes of mortality worldwide [8]. It is often accompanied by major risk factors like hypertension, hyperlipidemia, diabetes and obesity that is why usually multi drug regimen is required for management of CAD [9], in addition complementary and alternate medicine is gaining popularity owing to their minimal unwanted side effects [10]. According to an estimate 4–61% in Africa and Asia of cardiac patients, in Africa and Asia, take traditional medicines usually in combination with allopathic medicines [11].
Salvia miltiorrhiza root (Danshen) has been used quite commonly alone or with conventional drugs, by patients with angina pectoris and myocardial infarction, especially in Asia for its cardiovascular benefits as it contains both hydrophilic phenolic acids and lipophilic tanshinones, which are believed to be responsible for its therapeutic efficacy [12]. Around one hundred components are found in SMRE that can cause coronary vasodilatation, suppress thromboxane formation, inhibit platelet adhesion and aggregation, and scavenge free radicals [13, 14, 15].
Keeping in view the known actions of SMRE; in this study we tried to explore the role of SMRE in evaluation of hibernating myocardium and also compared the results of NO3 augmented and SMRE augmented scan to find out which one is the better modality. It was a hospital based interventional study, in which a total of 30 patients, 22 males and 8 females were included. Each one had a history of myocardial infarction, as shown in table 1, with ejection fraction less than 30% on echocardiography. Each patient underwent 03 studies, a resting scan, Nitrate scan and SMRE scan. TC 99m-NO3 augmented resting scan is well known diagnostic entity to evaluate hibernating myocardium.
We for the first time used SMRE for this purpose, keeping in mind, its already documented pharmacological effects. A meta-analysis of sixty randomized clinical trials showed that Danshen oral pill, consisting of S. miltiorrhiza, Dryobalanops camphora and Panax notoginseng showed much better efficacy compared to isosorbide dinitrate [16].
Results showed that out of total 30 patients, 15 didn’t demonstrate any viable/ hibernating myocardium i.e. neither with NO3 nor with SMRE scans, as shown in figure 1, whereas in the remaining 15; 08 patients (53.3%) showed improvement with SMRE alone, i.e. only with SMRE and not with NO3, as shown in figure 2. Only 02 cases (13.3%) showed improvement with NO3 alone, one of those cases is shown in Figure 3, and the remaining 05 patients (33.3%) showed improved perfusion in both SMRE and NO3 augmented scans.
In this new scientific era, everyone is more interested in evidence based medicine that is why utility and positivity of SMRE in nuclear scan shouldn’t be ignored. Moreover when statistical inference was drawn, SMRE augmented resting scan came out to be better diagnostic modality than NO3 scan.
A fact that is worth mentioning here is absence of any significant side effects of this naturally occurring gift. All nitrates are notorious for their blood pressure lowering effect [17, 18], but here; as we observed in the study, this herb didn’t have any of such harm full effects, a fact already document in many previously done studies [19].
Though sample size in this study was not that big, but for future we definitely recommend another study using SMRE as a diagnostic tool for assessing hibernating myocardium. Also SMRE should be considered as therapeutic strategy to manage patient with chronic heart disease, as SMRE not only improves micro vascular circulation [13], but also it didn’t show hypotension like side effects. Studies have shown that hypotension in people with heart failure and chronic heart disease is an indicator of poor prognosis and hinders the therapeutic management [18].
Like every treatment regimen, SMRE did show few side effects e.g. potentiation of anticoagulation of warfarin in three case reports [20, 21, 22] and a clinical study [23], but generally it was found to be quite a safe natural herb, to be utilized in patients with chronic heart disease for diagnostic as well as therapeutic purposes. At the end, one fact that is worth mentioning is that, it is a naturally occurring herb, which is much less costly than many of the allopathic medicines being used for management of chronic heart disease.
As cardiovascular illnesses are one of the most important problems globally and its incidence is increasing rapidly year by year, even in poor and developing countries [8]. The aim of the health professionals should be to find out management regimens which are not only clinically effective but also cost effective and this study supports SMRE to be one of such treatment options. So in view of the results achieved in this study we strongly recommend that more evidence based studies should be conducted with SMRE, with larger sample size, so that this natural gift of nature should be better utilized.
Conclusion
Salvia Miltiorrhiza Root Extract can be utilized in diagnosis as well as management of hibernating Myocardium, being safe and cost effective; it can be of great benefit in poor and developing countries.
References
-
Rahimtoola SH (1993) The hibernating myocardium in ischemia and congestive heart failure. Eur Heart J 14: 22- 26.
-
Braunwald E, Rutherford JD (1986) Reversible ischemic left ventricular dysfunction: evidence for the hibernating myocardium. J Am Coll Cardiol 8(6): 1467-1470.
-
Ye GF, Buerk DG, Jaron D (1995) Arteriolar contribution to microcirculatory CO2/O2 exchange. Microvasc Res 50(3): 338-359.
-
Zhou L, Zuo Z, Chow MSS (2005) Danshen: an overview of its chemistry, pharmacology, pharmacokinetics, and clinical use. J Clin Pharmacol 45(12): 1345-1359.
-
Williamson EM, Lorenc A, Booker A, Robinson N (2013) The rise of traditional Chinese medicine and its materia medica: a comparison of the frequency and safety of materials and species used in Europe and China. J Ethnopharmacol 149(2): 453-462.
-
Tan Y, Kamal MA, Wang ZZ, Xiao W, Seale JP, et al. (2011) Chinese herbal extracts (SK0506) as a potential candidate for the therapy of the metabolic syndrome. Clin Sci 120(7): 297-305.
-
Cabin HS, Roberts WC (1982) Quantitative comparison of extent of coronary narrowing and size of healed myocardial infarct in 33 necropsy patients with clinically recognized and in 28 with clinically unrecognized (“silent”) previous acute myocardial infarction. Am J Cardiol 50(4): 677-681.
-
(2014) Cardiovascular Diseases (CVDs). World Health Organization.
-
Dyakova M, Shantikumar S, Colquitt JL, Drew CM, Sime M, et al. (2016) Systematic versus opportunistic risk assessment for the primary prevention of cardiovascular disease. Cochrane Libr.
-
Peters JU (2013) Polypharmacology-foe or friend?. J Med 56(22): 8955-8971.
-
Hasan SS, Nadeem IA, Bukhari I, Wei Loon WC, et al. (2009) Use of complementary and alternative medicine among patients with chronic diseases at outpatient clinics. Complement Ther Clin Pract 15(3): 152-157.
-
Brantley SJ, Argikar AA, Lin YS, Nagar S, Paine MF (2014) Herb-drug interactions: challenges and opportunities for improved predictions. Drug Metab Dispos 42(3): 301-317.
-
Su CY, Ming Q, Rahman K, Han T, Qin LP (2015) Salvia miltiorrhiza: Traditional medicinal uses, chemistry, and pharmacology. Chin J Nat Med 13(3): 163-182.
-
Grant SJ, Bin YS, Kiat H, Tung Chang DH (2012) The use of complementary and alternative medicine by people with cardiovascular disease: a systematic review. BMC Public Health (12): 299.
-
Ji XY, Tan BKH, Zhu YZ (2000) Salvia miltiorrhiza and ischemic diseases. Acta Pharmacol Sin 21(12): 1089- 1094.
-
Jia Y, Huang F, Zhang S, Wai Leung S (2012) Is danshen (Salvia miltiorrhiza) dripping pill more effective than isosorbide dinitrate in treating angina pectoris? A systematic review of randomized controlled trials. Int J Cardiol 157(3): 330-340.
-
Thadani U, Rodgers T (2006) Side effects of using nitrates to treat angina. Expert Opin Drug Saf 5(5): 667-674.
-
Magny E, Donadio C, Maronnat F, Nghiem D, Berthelot E, et al. (2019) Hypotension in the elderly: Clinical and therapeutic features. Press Med 48(2): 134-142.
-
Poppel PCM, Breedveld P, Abbink JE, Roelofs H, Van Heerde W, et al. (2015) Salvia Miltiorrhiza Root Water-Extract (Danshen) Has No Beneficial Effect on Cardiovascular Risk Factors. A Randomized Double- Blind Cross-Over Trial. PLose One 10(7): e0128695.
-
Tam LS, Chan TY, Leung WK, Critchley JA (1995) Warfarin interactions with Chinese traditional medicines: danshen and methyl salicylate medicated oil. Aust N Z J Med 25(3): 258.
-
Yu CM, Chan JCN, Sanderson JE (1997) Chinese herbs and warfarin potentiation by ‘Danshen’. J Intern Med 241(4): 337-339.
-
Izzat MB, Yim APC, El Zufari MH (1998) A taste of Chinese medicine!. Ann Thorac Surg 66(3): 941-942.
-
Yan Q, Jiang JQ (2008) Effect of Danshen tablet on anticoagulation of warfarin. J Tradit Chin Med 30(1): 19- 21.
- Contribution of 18FDG PET in Atypical HORTON Disease
- Living Conditions, Healthy Practice and State of Households of a Town Rural in Colombia
- Background to the Health and Safety Regulation at Work in Colombia
- Risk Factors Psychology Workers Sena (Center for the Petrochemical Industry) Regional Bolívar, Colombia
- Diffuse Intense Pleural FDG Uptake with Smooth Thickening: A MARKER of Tuberculosis in Isolated Pleural Effusion
- Hypermetabolic Splenomegaly with Infarct in FDG PET/CT: A Clue to Scrub Typhus in PUO