Contribution of a Three-Phase 99m Tc-HMDP Bone Scintigraphy Protocol Completed by SPECT-CT Scan in the Diagnosis and Management of Langerhans Cell Histiocytosis of Bones in an Adolescent
Langerhans Cell Histiocytosis (LCH) or Histiocytosis X is a rare disorder of the reticuloendothelial system due to the accumulation of Langerhans cells in the tissues, most often organized into granulomas. The bone is the most affected organ. It can be a single osteolytic lesion or a multi-systemic form with organ dysfunction. We report herein the case of a 15-yearold adolescent male with bone pain in the hip evolving for two months in whom the diagnosis of unifocal bone langerhansian Histiocytosis was confirmed by a triple phase bone scintigraphy supplemented by SPECT CT objectifying a single focus of the disease at the greater left trochanter of the femoral bone without any other pathological bone fixation clearly identifiable on the other parts of the skeleton. This clinical case allows us to clarify the key role of a triple phase bone scan supplemented by SPECT CT in the diagnosis and management of Langerhans Cell Histiocytosis of bone in our context.
Fokoué F*, El Mselmi S, Abaouz N and Ismaili Alaoui N
Introduction
Langerhansian Cell Histiocytosis (LCH) or X Histiocytosis is a rare disorder of the reticuloendothelial system due to an abnormal accumulation of Langerhans cells in the tissues, most often organized into a granuloma. This condition mainly occurs in children or young adults. The clinical presentation varies according to the affected tissues. It may be a single osteolytic lesion or a multisystem form with organ dysfunction. Bone remains the most affected tissue, followed by skin and pituitary gland. We report herein the case of a 15-year-old adolescent boy presenting with a bone pain in the left hip progressing for two months in whom diagnostic imaging supplemented by a bone biopsy was in favor of a Langerhans Cell Histiocytosis of bone confirmed by the histological and immunohistochemical study. A bone scan was subsequently ordered confirming unifocale bone involvement. The aim of this work is to show the place of three-phase bone scintigraphy supplemented by SPECT CT in the initial management of Langerhans Cell Histiocytosis of bone.
Patient and Method
This is a 15-year-old boy, with no particular medical history admitted to the pediatric service for management of a bone pain in the left hip predominantly at night, with a partial response to the usual analgesics, evolving for 02 months after a notion of neglected trauma to the pelvis during a football game. The clinical examination highlighted a weight of 64 kg, a normal height for age with a normal dermatological and neurological examination, an absence of polyuropolydipsic syndrome. The rest of the clinical examination was unremarkable apart from the osteoarticular examination which revealed a slight localized pain in the left hip during palpation, with limitation of the flexion movement of the thigh on the torso and a slight lameness in the left hip. The initial biological assessment was normal with normal fasting blood glucose at the level of 5.2 mmol/L (3.89-6.2 mmol/L), SR, renal function and blood ionogram at a normal value. An MRI of the hip was performed after an initial pelvic X-ray showing a bone lesion in the left greater trochanter measuring 25 mm x 23 mm x 21 mm associated with a hypo intense intra osseous edema in T1 with a T2 hyper signal which was intensely and evenly enhanced afterwards contrast injection. A bone biopsy was then performed on the bone lesion objectified by pelvic X-ray and MRI. Histological and immunohistochemical studies concluded to a Langerhans Cell Histiocytosis of bone. Standard x-rays of the pelvis, knees and skull taken as part of an initial extension workup returned with normal findings apart from the already known bone lesion in the left greater trochanter. The patient was subsequently referred to the nuclear medicine department for a bone scan to look for other sites of bone damage.
Results
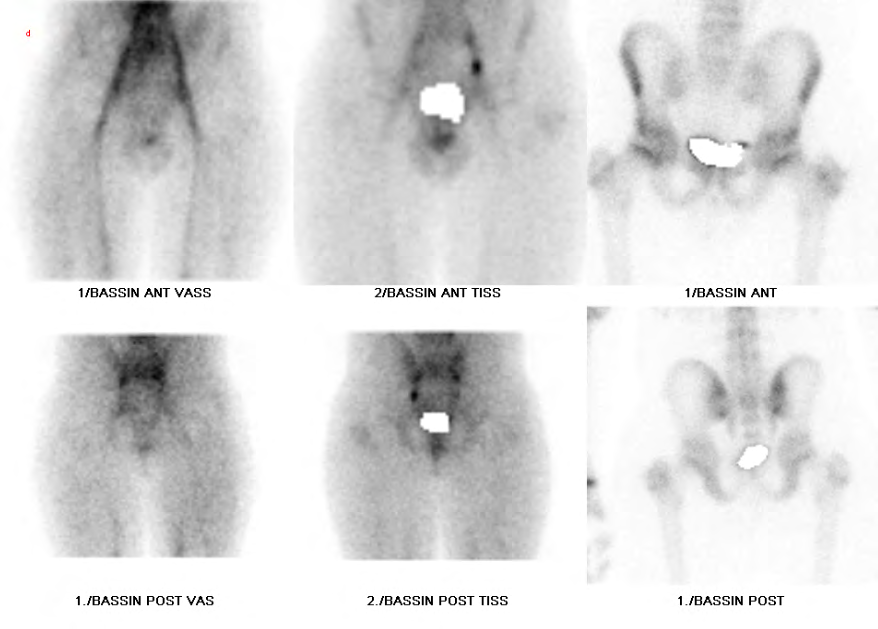
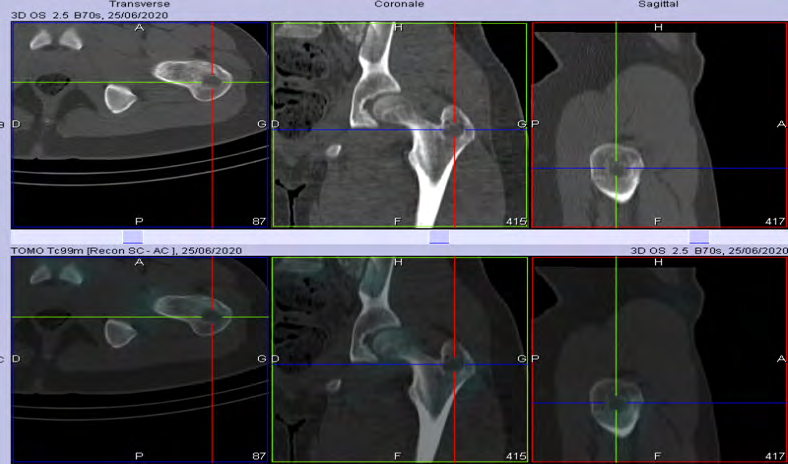
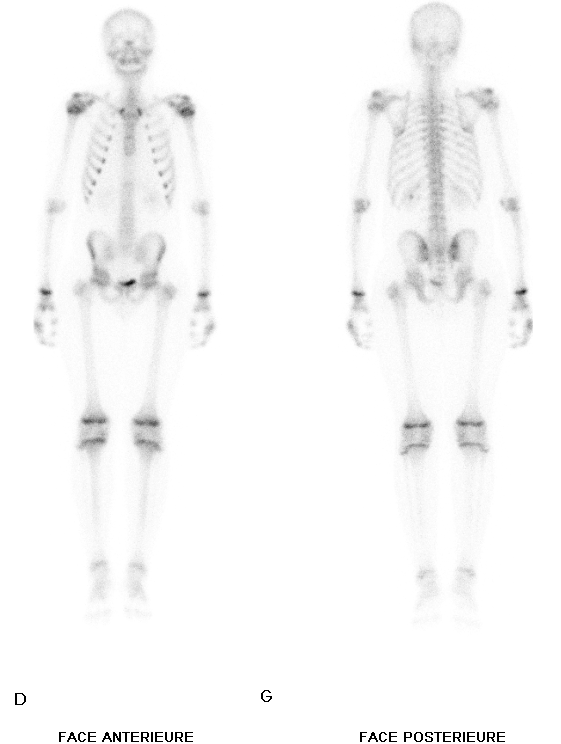
We performed early static images centered on the pelvis between 0-10 min, then a full body scan examination and late static images supplemented by a SPECT CT focused on the pelvis 2 hours after an intravenous injection of 481 MBq (13 mCi) of Methylene Diphosphonate labeled with metastable Technetium 99 (MDP-99mTc). The early and late images were acquired with a Siemens dual head Gamma Camera, Symbia T6 2010 model. Bone scintigraphy carried out in 03 phases showed a moderate hyperemia of the left hip at the early stage and moderately intense bone hyperfixation of the left greater trochanter at the late stage. The complement by SPECT CT revealed the lacunar bone lesion previously described on to the left greater trochanter both on standard radiographs and MRI without any other fixation or bone structure anomaly clearly identifiable on the entire skeleton thus making it possible to conclude to an unifocal presentation of the Langerhans Cell Histiocytosis of bone presented by the patient (Figures 1-5).

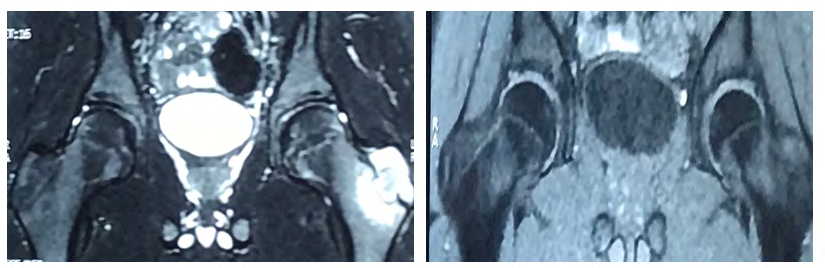
Figure 2: MRI of the hip showing a bone lesion in the left greater trochanter with T2 discreet hypersignal, well limited T1 hypersignal and regular contours, surrounded by a border with T1 and T2 hypointense without enhancement after injection of contrast. It measures 25mm x 23mm x 21mm and is accompanied by intraosseous edema in hypointense T1, Hypersignal T2, which is intensely and evenly enhanced after injection of contrast.
Discussion
Langerhans Cell Histiocytosis is a rare disease which belongs to a group of conditions called Histiocytosis. In the general population the estimated annual incidence of LCH ranges from 0.5-5.4 cases per million of persons per year. LCH more frequently affects young adults, but it can also be seen in very young children. The incidence of LCH in children is determined as 2–9 per million of persons per year and is slightly predominant in males (M/F = 1.2–1.4). In our observation, the child was 15 years old adolescent male. Actually the pathogenesis of this condition is becoming more and more precise. Osteolytic bone involvement is the most common circumstance of discovery [1, 2].
LCH of bone can manifest as bone pain, broken bones or swelling. The clinical examination should always look for skin lesions because they have an important diagnostic value. The rapid spread of the disease to other organs is an actor of poor prognosis [2]. In our observation, the disease was revealed by bone pain localized in the left hip with no skin lesions and no involvement of other organs.
With regard to the pathogenesis of LCH, the cells involved are abnormal by their presence in many organs and tissues and by their oligoclonal proliferation. These cells initially described by Paul Langerhans in 1868 belong to the reticulo- endothelial system. Initially, three forms of expression of the same disease were described:
- Letterrer-Siwe’s disease, an acute form of infants, characterized by multi-visceral involvement including hepato-splenomegaly and a very poor prognosis.
- Hand-Schüller-Christian disease, which combines exophthalmia, diabetes insipidus and cranial deficiencies. The coexistence of the three elements of this triad is however inconstant, found in only 10% of cases.
- Eosinophilic granuloma, mainly in older children, which is more frequently single than multiple and generally has a favorable outcome, affecting 60% of cases of LCH of bone in pediatric age.
In 1953, Lichtenstein highlighted histopathological similarities allowing these distinct clinical manifestations to be grouped under a single nosological entity, Histiocytosis X.
In 1973, Nizelof et al established that the pathophysiological link between these syndromes is the dysfunction of Langerhans cells. The disease is now called Langerhans Cell Histiocytosis [3]. Subsequently it was classified into 03 groups:
- Group 1 including Langerhans Cell Histiocytosis (all forms included);
- Group 2 comprising Non-Langerhans Cell Histiocytosis and Benign Histiocytosis (juvenile xanthogranuloma, Rosai-Dorfmann-Destombes disease, Erdheim Chester disease, Lymphohistiocytosis, Hemophagocytic);
- Group 3 including Malignant Histiocytic diseases (malignant Histiocytosis and Histiocytic sarcoma).
In 2016, significant progress in cellular and molecular biology led to rapid changes in the diagnostic and therapeutic modalities of Histiocytosis and to a revision of their classification by Emile JF, et al. [3] in which Histiocytosis are listed in five main groups (Tables 1 & 2).
- Group L comprising Langerhans cell Histiocytosis and Erdheim-Chester disease which are now considered as inflammatory myeloid neoplasms with the discovery of mutations in the BRAFV600E and MAP2K genes in two thirds of patients;
- Group C including non-Langerhans skin diseases such as Multicentric Reticulohistiocytosis and Xanthoma Disseminatum;
- Group R including Rosai-Dorfman-Destombes disease;
- Group M (malignant histiocytosis) and group H (hemophagocytosis).
The osteoarticular manifestations of Histiocytosis are found in groups L, C and R.
| Group L (Langerhans) | Langerhans Cell Histiocytosis (LCH)Indeterminate Cell HistiocytosisErdheim-Chester disease (ECD) |
| Group C (Cutaneous) | Non-Langerhansian Histiocytosis Cutaneous or mucocutaneous:* Xanthogranuloma family* “Juvenile non-xanthogranuloma” familyCutaneous non-Langerhansian Histiocytosis with component major systemic:* Xanthogranuloma family: disseminated xanthoma* “Non-xanthogranuloma” family: multicentric reticulohistiocytosis (MRH) |
| Group R (Rosai) | Familial Rosai-Dorfman-Destombes disease (FRDD): classic lymph node, extra lymph node, associated with tumors or autoimmune disease, unclassifiable |
| Group M (Malignant) | * Primary Malignant Histiocytosis: Histolytic sarcomas, Sarcomas with interdigital dendritic cells, Langerhans cell sarcomas.* Secondary malignant histiocytosis: Associated with or following lymphoma or leukemia. |
| Group H (Hemophagocytosis) | Primary Hemophagocytic Lymphohistiocytosis and Secondary Hemophagocytic Lymphohistiocytosis |
Table 1: Classification of Histiocytosis according to Emile JF, et al. [3].
| Frequencies (in percentage) | |
|---|---|
| Bone | 70-80% |
| Skin | 10-50% |
| ENT | >15% |
| Hypophysis | 5-50% |
| Orbital | <20% |
| Mouth | 6% |
| Gastrointestinal tract | 2-13% |
| Lung | 5% |
| Liver | 4% |
| Ganglia | <10% |
Table 2: Frequency and locations of mono-tissue forms of Langerhansian Histiocytosis in children [3].
The diagnostic criteria defined by the Histiocytic Society are as follows: Presumed diagnosis: by light microscopy findings; Probable diagnosis: by optical microscopy findings and 2 of the following markers: adenosine triphosphatase, D-mannosidase, peanut agglutinin104; Definitive Diagnosis: including optical microscopy findings and 1 of the following criteria.
Birbeck granules (electron microscopy, a long and expensive technique) or labeling of pathological cells with the CD1a antigen. The S100 protein is present in LCH but is not specific since it is also demonstrated in Rosai Dorfmann Destombes disease. In our patient, histology and immunohistochemistry made it possible to make the definitive diagnosis of LCH, in particular by the demonstration within several tumor cells of an expression marked by the CD1a antigen, and an intense expression of the S 100 protein. After establishing the definitive diagnosis, in addition to a meticulous ENT and stomatologic clinical examination and a biological workup including FBC, ionogram, CRP and liver workup, certain imaging examinations are generally requested. These are skeletal x-rays or even cross-sectional examinations; in particular CT or MRI centered according to clinical or biological call points [4, 5].
In our case study, a standard x-ray on the pelvis was initially carried out followed by a focused MRI both showing the bone lesion and thus allowed to perform of a biopsy and curettage allowing the diagnosis to be made after a histological and immunohistochemical confirmation, and also to treat the patient.
With regard to the morphological imaging means generally used in first intention, standard radiographs are often oriented by the painful bone site and can show osteolysis with a geode image. CT can confirm the presence of osteolysis with a better analysis of the corticoperiosteal reaction and the extent of bone lesions, especially at the base of the skull. MRI can better identify the involvement of soft tissues adjacent to the bone [5, 6].
The role of bone scintigraphy has long been debated, because while it allows whole body examination with high sensitivity for detection, it has low specificity for precise anatomical analysis of bone lesions. Whole-body bone scintigraphy provides an initial mapping of bone lesions, but is less sensitive than radiography in the diagnosis of eosinophilic granuloma [6].
In LCH of bone, the whole body bone scintigraphy can show foci of hypofixation, but most often hyperfixation. Hyperfixation in this case corresponds to osteocondensing lesions and hypofixation to pure osteolytic lesions without edematous reaction. The edematous reaction corresponding to a hyperemia observed during vascular and / or tissue phase if a three-phase scintigraphy is performed. Normal fixation corresponds to small lesions or lesions where the tumor is still confined to the medullar canal.
The sensitivity of bone scintigraphy increases significantly for the detection of active and multiple lesions. Whole-body MRI has been shown to have better sensitivity than bone scans and whole skeletal x-rays, but all of these imaging modalities have comparable accuracy in the initial risk stratification in patients [7, 8].
The advent of SPECT CT hybrid imaging has made it possible to increasingly upgrade bone scintigraphy because it allows for a better initial extension assessment or a mapping of the disease by a complete functional imaging of the skeleton with anatomical location thus increasing the specificity and sensitivity of bone scintigraphy in detecting bone lesions, thus allowing a more adequate initial therapeutic decision. It may also have a role in the follow-up of treated patients who already have known bone lesions [7, 8].
A recent retrospective study on the additional value of PET CT scan has shown that an initial PET CT scan with 18FDG would better characterize the extent and specificity of certain locations compared to CT or MRI exams alone for all forms of Histiocytosis. In addition, 18FDG PET CT scan would be very useful for the evaluation of the metabolic response to immunomodulatory treatments when these are used [9, 10]. It has also been shown that 18FDG PET CT scans can provide information that bone scintigraphy might omit and is therefore superior to it. In addition to bone analysis it makes it possible to highlight, on the one hand, tissue and organ lesions, in particular ganglionic, splenic and hepatic damage, which may be omitted by other means of imaging and, on the other hand possibly to identify the possible sites bone biopsy, finally the PET CT scan could therefore be good exam for the follow-up of treated patients who already have known organ lesions [10, 11, 12].
In our case study, a three-phase bone scintigraphy centered on the pelvis was performed followed by a whole body bone scan, and SPECT CT imaging focused on the area of bone hyperfixation. This protocol allowed to ‘’ establish a precise map of the bone damage by a panoramic analysis of the entire skeleton, and to confirm the unifocal nature of the bone damage by characterizing the unique bone lesion of the left greater trochanter objectified on standard radiographs and MRI centered on the painful area.
Regarding the therapeutic management of LCH of the bone, single or few bone lesions in number generally do not require any treatment, other than the biopsy or fine needle aspiration necessary to confirm the diagnosis and to reduce de pain. Surgical treatment by curettage or osteosynthesis to reduce the risk of fracture may be prescribed. Multifocal forms of LCH can be an indication of chemotherapy alone or combined with corticosteroid therapy and / or external radiotherapy. The first line chemotherapy is Vinblastine or Etoposide if indicated [1, 3, 8].
External radiotherapy remains very delicate because of the risk of secondary cancer in the irradiation field. At moderate doses, between 10 and 15 grays, it can be useful in the event of a very extensive and / or extensive lesion.
Conclusion
Although 18-FDG PET CT seems to be the Gold standard in the initial extension workup and follow-up for Langerhans Cell Histiocytosis, our case study demonstrates the key role of HMDP-99mTc bone scintigraphy supplemented by SPECT CT in the management of LCH of the bone, thus making it possible to establish an initial lesion mapping of the bone sites affected, by an accurate analysis of the entire skeleton. It thus allows easier subsequent monitoring with better diagnostic value and better value for money compared to other imaging methods with acceptable overall dosimetry.
References
-
Donadieu J, Héritier S (2017) Histiocytose Langerhansienne de l’enfant. The Medical Press 46(1): 85-95.
-
Abbott GF, Christenson MLR, Franks TJ, Frazier AA, Galvin JR (2004) From the archives of the AFIP: pulmonary Langerhans cell histiocytosis. Radiographics 24(3): 821- 841.
-
Emile JF, Abla O, Fraitag S, Horne A, Haroche J, et al. (2016) Revised classification of histiocytoses and neoplasms of the macrophage-dendritic cell lineages. Blood 127(22): 2672-2681.
-
Geevasinga N, Jeremy R, Crombie CM, N Manolios (2005) Histiocytose and bone: Experience from one major Sydney teaching hospital. Intern Med J 35(10): 622-625.
-
Chalès G, Guggenbuhl P, Rousseau BC, Cathelineau C, Guillin R (2020) Manifestations ostéoarticulaires des histiocytoses de l’adulte. EMC - Appareil locomoteur 34(1): 1-15.
-
Ghir I, Amrani M, Ouboukdir R, Mhamdi F, Bellaoui W, et al. (2012) Intérêt de l’imagerie hybride TEMP-TDM dans l’histiocytose langerhansienne osseuse. À propos d’un cas. Médecine Nucléaire 36(10): 644-647.
-
Micheline R, Georges C, Anne D, Carrier P, Darcourt J (2008) Intérêt de la scintigraphie osseuse dans l’Histiocytose Langerhansienne. À propos d’un cas. Médecine Nucléaire 32(9): 495-499.
-
Jeong RK, Hee MY, Ah YJ, Cho YA, Seo JJ, et al. (2019) Comparison of whole-body MRI, bone scan and radiographic skeletal survey for lesion detection and risk stratification of Langerhans Cell Histiocytosis. Sci Rep 9: 317.
-
Phillips M, Allen C, Gerson P, McClain K (2009) Comparison of FDG-PET scan to conventional radiography and bone scans in the management of Langerhans cell Histiocytosis. Pediatr Blood Cancer 52(1): 97-101.
-
Zehra P, Selcuk S, Saadet A, Balci TA, Onur MR, et al. (2015) Insufficiency of Bone Scintigraphy in vertebral lesion of Langerhans Cell Histiocytosis Compared to F-18 Fluodeoxyglucose Positon Emission Tomography/ Computed Tomography and Diagnostic Computed Tomography. Mol Imaging Radionucl Ther 24(1): 21-24.
-
Sager S, Yilma S, Sager G, Halac M (2010) TC 99m bone scan and fluoroxydeosyglucose positron emission tomography in evaluation of disseminated Langerhans cell histiocytosis. Indian J Nucl Med 25(4): 164-167.
-
Vija LM, Bera G, Haroche J, Cohen F, Riffaud PC, et al. (2015) Rôle de la TEP/TDM au 18FDG dans la caractérisation et le suivi thérapeutique des histiocytoses. Médecine Nucléaire 39(4): 357-370.
- Contribution of 18FDG PET in Atypical HORTON Disease
- Living Conditions, Healthy Practice and State of Households of a Town Rural in Colombia
- Background to the Health and Safety Regulation at Work in Colombia
- Risk Factors Psychology Workers Sena (Center for the Petrochemical Industry) Regional Bolívar, Colombia
- Diffuse Intense Pleural FDG Uptake with Smooth Thickening: A MARKER of Tuberculosis in Isolated Pleural Effusion
- Hypermetabolic Splenomegaly with Infarct in FDG PET/CT: A Clue to Scrub Typhus in PUO