Undescended Testis Cancer Detected on FDG PET-CT Imaging in a Pediatric Patient
Cryptorchidism is one of the major risk factors for increased risk of testicle cancer. The differential diagnosis at the inguinal region is very important for hypermetabolic foci because of the possibility of metastasis at this level in cancer patients ongoing PET imaging for detection of metastases. In this case report, the findings of a pediatric patient with inguinal testis cancer identified as primary malignity region on FDG-PET/CT imaging, is presented.
Introduction
Positron emission tomography-Computed Tomography (PET-CT) with fluorine-18 fluorodeoxyglucose (F18-FDG) has evolved as a useful imaging modality in the assessment of a variety of cancers, especially for tumor screening, staging, restaging and post treatment monitoring. In this case report, the findings of a pediatric patient with inguinal testis cancer identified as primary malignity region on FDG-PET/CT imaging, is presented. CT imaging provided by PET/CT has been useful in showing increased FDG uptake seen on PET imaging in inguinal region belonging to testis.
Case Report
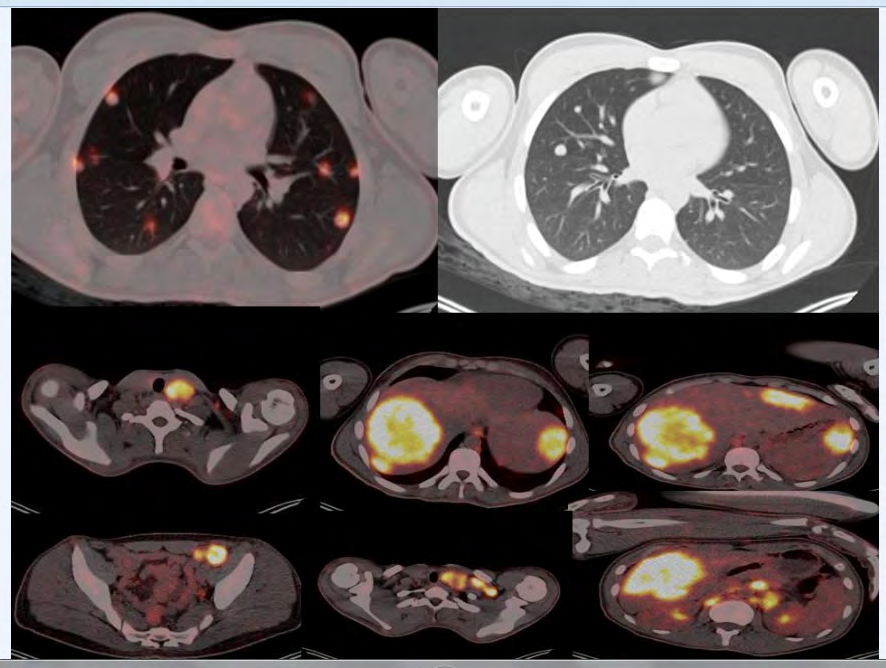
A 16-year-old male pediatric patient with inguinal mass was referred for FDG-PET/CT examination for metabolic characterization and searching for primary malignity region. Total body PET/CT images from the top of the skull to the thighs were acquired 60 min. after the intravenous injection of 8.2 mCi (303 MBq) of FDG per standard protocol. On FDG-PET/CT imaging, increased FDG uptake was detected at left cervical, supraclavicular, (SUVmax: 18.89), anterior mediastinal, prevascular, left paratracheal, right paraosephageal, paracardiac (SUVmax: 19.74), retroperitoneal, hilus of spleen, bilateral paraaortic, aortacaval, parailiac, mesenteric, left pelvic and left inguinal (SUVmax: 22-27) conglomere lymphadenopathies. Metastatic nodules and masses fewer than 10 with increased FDG uptake at left and right liver paranchime (SUVmax: 23) and metastatic subplevral and paranchimal nodules more than 20 with increased FDG uptake (SUVmax: 24.88) were seen (Figure 1).
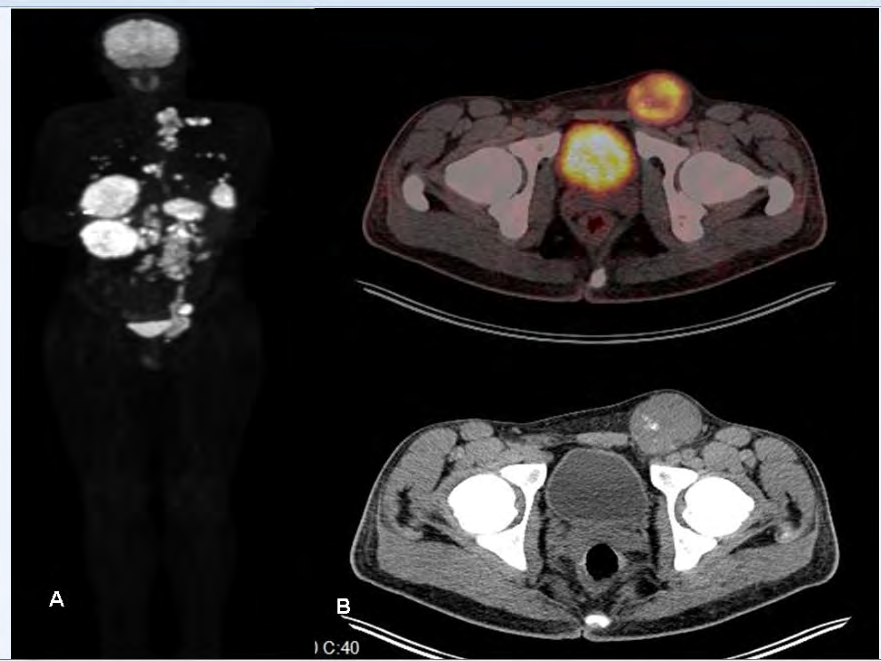
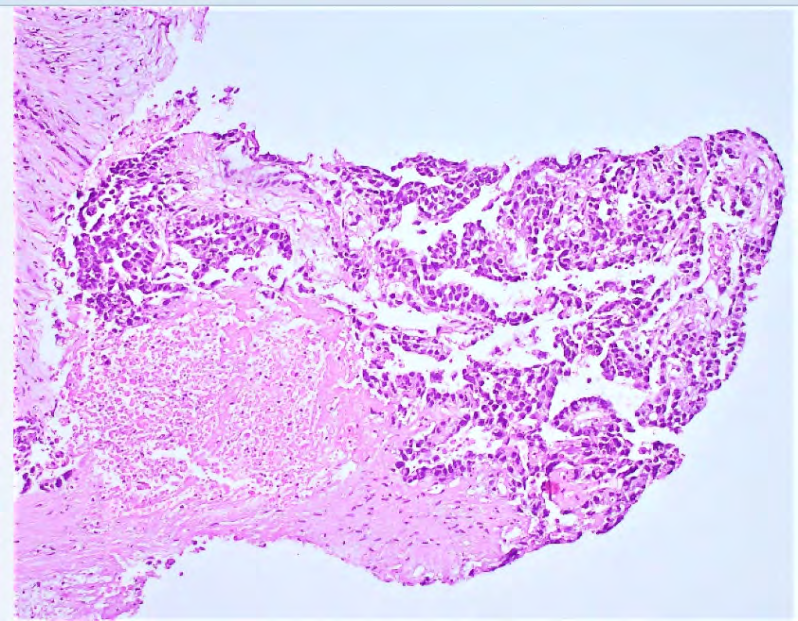
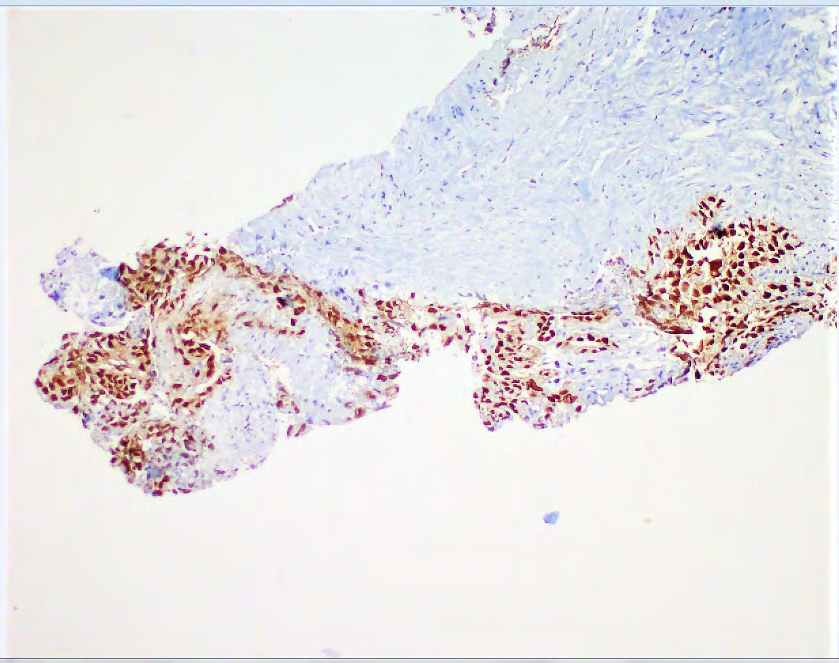
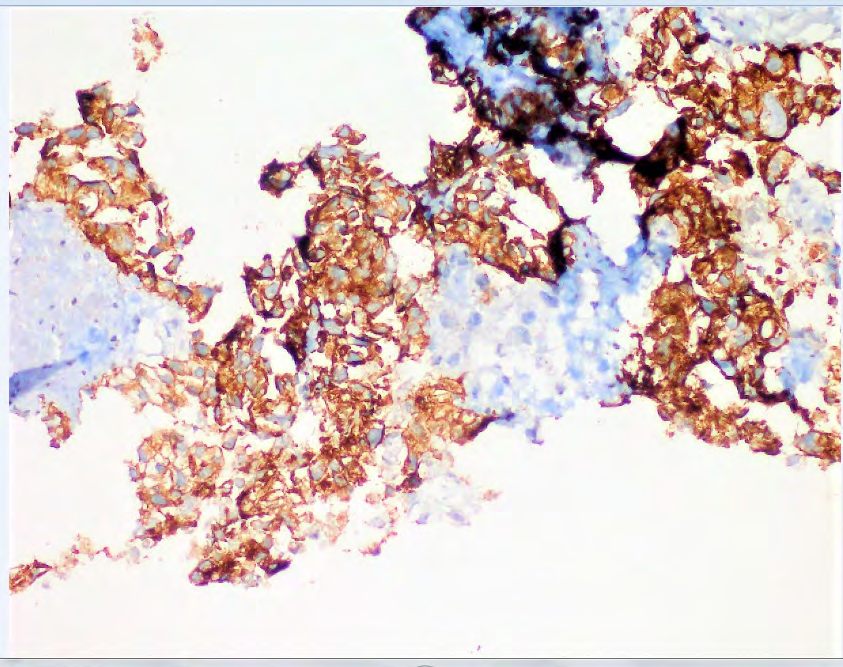
Additionally, left inguinal 5 X 5.5 cm mass with central necrosis and calcification belonging to undescended testis (SUVmax: 19.47) that appears separated from the inguinal lymphadenopaties was detected (Figure 2). PET/CT fusion image has confirmed that this activity was belonging to an undescended testicle activity. Biyopsy confirmed germ cell embrional carcinoma (Figures 3-5).
Discussion
Testicular cancer is a disease which mainly affects men between 15 and 35 years [1]. It has a share of 1% of all solid tumors in the western world with an increasing incidence of 3–10/100,000 [2]. Cryptorchidism or the failure of testicular descent is the most common defect in newborn boys. Cryptorchidism is an established risk factor for both infertility and testicular germ cell tumors. Cryptorchidism is one of the major risk factors for increased risk of testicle cancer. The differential diagnosis at the inguinal region is very important for hypermetabolic foci because of the possibility of metastasis at this level in cancer patients ongoing PET imaging for detection of metastases. It is important to differentiate the activity in the groin from lymph node activity, testicular cancer, metastatic disease activity, inflamation and urine skin contamination artefact [3]. Also, on pelvic imaging urinary bladder activity can easily be confused with the activities of scrotum, intestine and rectum.
F-FDG PET/CT showed statistically significant measurements for differentiation between malignant and benign lesions with a sensitivity of 90.6% and a specificity of 80.9% [4]. In this case, CT component of the PET/CT provided an advantage in the differential diagnosis of the inguinal region. CT imaging findings has been useful in showing increased FDG uptake seen on PET imaging at left inguinal region belonging to an undescended testis activity.
Disclosures
All authors assert that there are no conflicts of interest (both personnel and institutional) regarding specific financial interests that are relevant to the work conducted or reported in this manuscript.
References
-
Boccellino M, Vanacore D, Zappavigna S, Cavaliere C, Rossetti S, et al. (2017) Testicular cancer from diagnosis to epigenetic factors. Oncotarget 8(61): 104654-104663.
-
Rosen A, Jayram G, Drazer M, Eggener SE (2011) Global trends in testicular cancer incidence and mortality. Eur Urol 60(2): 374-379.
-
Hinojosab D, Josepha UA, Wana DQ, Barona BJ (2008) Inguinal herniation of a bladder diverticulum on PET/ CT and associated complications. Clinical Imaging 32(6): 483-486.
-
Shao D, Gao Q, Tian XW, Wang SY, Liang CH, et al. (2017) Differentiation and diagnosis of benign and malignant testicular lesions using 18F-FDG PET/CT. Eur J Radiol 93: 114-120.
- Contribution of 18FDG PET in Atypical HORTON Disease
- Living Conditions, Healthy Practice and State of Households of a Town Rural in Colombia
- Background to the Health and Safety Regulation at Work in Colombia
- Risk Factors Psychology Workers Sena (Center for the Petrochemical Industry) Regional Bolívar, Colombia
- Diffuse Intense Pleural FDG Uptake with Smooth Thickening: A MARKER of Tuberculosis in Isolated Pleural Effusion
- Hypermetabolic Splenomegaly with Infarct in FDG PET/CT: A Clue to Scrub Typhus in PUO