Hepatic Abscess Secondary to Appendiceal Phlegmon an Unusual Complication of Appendiceal Phlegmon
Liver Abscess is a focal supportive process, encapsulated collection filled with pus, infrequent, with moderate mortality of approx. 2-12% according to the literature. The pathogens responsible mainly belong to two groups, bacteria and parasites (Entamoeba Histolytica), and give rise to two types of liver abscesses, pyogenic and amoebic, respectively. The most common causes are abdominal infections, such as acute appendicitis, diverticulitis, inflammatory bowel disease, etc., or systemic infections such as bacterial endocarditis or manipulation of the biliary tract. A pyogenic liver abscess secondary to appendiceal plastron infection is a rare manifestation that has not been well illustrated in the literature. We analyzed a 65-year-old male patient who presented abdominal pain more than 2weeks with a palpable tumor in the right iliac fossa, fever, chills, diarrhea and weight loss and was found to have a pyogenic liver abscess that was suspected to be secondary to an abscessed tumor in the right colon, which turned out to be secondary to Appendicular Plastron. The purpose of this article is to describe a patient who presented notable clinical features and a rare cause of liver abscess, to assist in the diagnosis and treatment of future patients.
Abbreviations
GGT: Gamma-Glutamyl Transferase; AST: Aspartate Aminotransferase; ALT: Alanine Aminotransferase; CT: Computed Tomography; HU: Hounsfield Units.
Introduction
Hepatic abscesses, though rare, present a significant clinical challenge due to their potentially severe complications and variable presentation. These abscesses are typically classified as pyogenic or amoebic, with pyogenic liver abscesses accounting for approximately 0.0023% of all hospital admissions globally. This low incidence rate, however, belies the high morbidity and mortality associated with the condition, particularly when diagnosis or treatment is delayed. Most pyogenic hepatic abscesses arise from biliary tract disease, though in rare cases, they may result from hematogenous spread of infection from other intra- abdominal sources, such as appendicitisegmon is an uncommon complication of untreated acute appendicitis, representing a localized infection where adjacent structures contain the spread of infection around a ruptured appendix. While this formation limits peritonitis, the localized infection can lead to abscess formation or even, in rare cases, systemic spread, resulting in secondary hepatic abscesses. This complication is particularly unusual, with appendicitis accounting for only 1-10% of all cases of pyogenic liver abscess, depending on the study and population assessed.
In Paraguay, logy of hepatic abscesses is limited, though similar patterns to global trends are observed, with a predominant occurrence in older male patients and a significant risk associated with underlying comorbid conditions. Within the regions of Paraguay, no specific regional variations in incidence have been identified, though rural populations may face delays in diagnosis due to limited access to specialized healthcare facilities. The following case presents a unance of a hepatic abscess secondary to appendiceal phlegmon, underscoring the importance of timely diagnosis and appropriate intervention in complex abdominal infections.
Clinical Case
A 65-year-old male patient was referred from another facility with a 17-day history of intermittent, stabbing pain localized in the right iliac fossa, which subsequently radiated to the hypogastrium and left iliac fossa. The pain was moderate in intensity and aggravated intermittently. The patient reported accompanying symptoms of nausea, multiple episodes of vomiting with food content and liquid stools for more than two weeks. The condition was associated with intermittent fever, chills, generalized weakness, and approximately 15 kg of weight loss since the onset of symptoms.
The patient initially sought medical attention at another facility, where he was hospitalized for 16 days and treated with Piperacillin-Tazobactam (4.5 g IV every 8 hours, day 4) and Metronidazole (500 mg IV every 8 hours, day 4).
Upon admission to our service, the patient exhibited mild protein-calorie malnutrition. Vital signs were within normal limits, without systemic compromise. Physical examination of the abdomen revealed distention, with a mildly depressible abdomen and tenderness in the right iliac fossa and hypogastrium. A 10 cm, poorly mobile mass with smooth walls and ill-defined borders was palpable in these regions, exhibiting guarding but without signs of peritoneal irritation [1, 2]. A fluid wave was present, and bowel sounds were preserved. Digital rectal examination revealed a normotonic sphincter, an empty rectal ampulla, a non-bulging and non-tender pouch of Douglas, normal temperature, and yellowish liquid stool on the glove. The remainder of the physical examination was unremarkable.
Initial laboratory results included hemoglobin of 9.5 g/ dL, hematocrit of 28%, white blood cell count of 6,280/mm³ (68% neutrophils), platelets of 444,000/mm³, prothrombin time of 75%, INR of 1.22, creatinine of 1.5 mg/dL, and urea of 51 mg/dL. Electrolytes were within normal limits (Na/K/Cl: 135/3.5/104 mmol/L). Liver function tests revealed elevated gamma-glutamyl transferase (GGT) at 434 U/L and alkaline phosphatase at 578 U/L, while aspartate aminotransferase (AST) and alanine aminotransferase (ALT) were within normal limits (28 U/L and 14 U/L, respectively). Prealbumin was low at 7 mg/dL. Urinalysis was unremarkable.
Procalcitonin level was 1.2 ng/mL, raising suspicion of sepsis likely originating from an abdominal source, with a provisional diagnosis of abscessed cecal neoplasm. Therefore, Amikacin (1 g IV every 24 hours) was added to the initial antibiotic regimen of Piperacillin-Tazobactam (4.5 g IV every 8 hours), while Metronidazole was discontinued.
The patient brought an abdominal ultrasound report indicating hepatomegaly with approximately 800 cc of free, multi-compartmental fluid in the abdominal cavity. A computed tomography (CT) scan with double contrast of the abdomen and pelvis was planned, contingent upon improvement in his renal function.
During hospitalization, the patient developed tachypnea but maintained good oxygen saturation. On auscultation, diminished breath sounds were noted bilaterally at the lung bases. Chest X-ray and pleural ultrasound confirmed the presence of inhomogeneous fluid collections at both lung bases, with volumes of 1,284 cc on the right and 500 cc on the left (Figure 1).
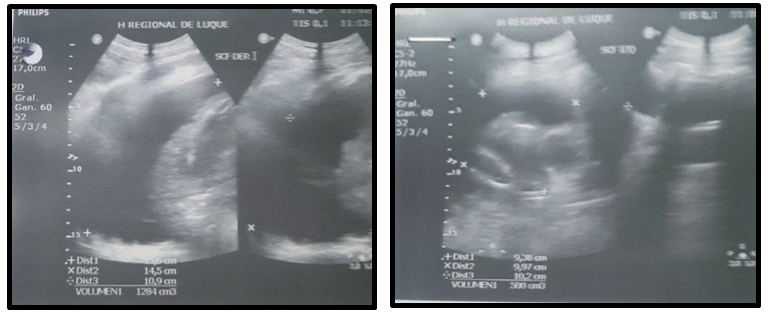
A thoracentesis was performed, yielding an exudate per Light’s criteria, after which the patient experienced improvement in tachypnea.
A contrast-enhanced CT scan of the abdomen and pelvis (Figure 2) revealed a small amount of free fluid in the peritoneal cavity, with minimal fluid seen between jejunal loops, extending to the left hypochondrium and flank. The liver was enlarged with regular contours and contained a large collection occupying segments VI, VII, and VIII of the right lobe. The hypodense area appeared to have a clear fluid density of 16 Hounsfield units (HU) without visible septa. A gas bubble was noted in the uppermost part of the collection. The approximate volume of the collection, which was well-demarcated from healthy liver parenchyma but lacked a distinct capsule or significant pseudocapsule, was estimated at around 1,800 cc. No nodular solid changes or areas of contrast hyper enhancement were observed in the liver. Intrahepatic bile ducts were not dilated. The common bile duct measured 7 mm, with no signs of dilation. The colonic framework was well visualized, with a typical form and positioning, and no signs of inflammation. No diverticula were identified, and the appendix was not visualized. Major blood vessels showed no segmental dilation, and no significant lymphadenopathy was noted.
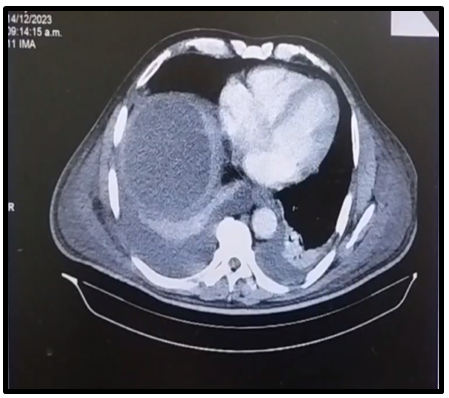
A decision was made to aspirate the collection, and a multipurpose catheter was placed using the Seldinger technique. Approximately 2,000 cc of purulent fluid was drained during catheter placement. A sample was sent for culture and sensitivity testing.
The CT report showed the colonic framework was well-visualized, with typical form and positioning, no signs of inflammation, no diverticula, and the appendix was not visualized. Due to the persistence of the patient’s liquid stools and to further investigate the etiology of the hepatic abscess, a colonoscopy was performed.
The colonoscopy report indicated that the rectum, sigmoid, descending, transverse, and ascending colon had preserved folds, caliber, and distensibility, with no lesions observed. In the cecum, the mucosa appeared normal, and the ileocecal valve was patent. A purulent discharge was noted emanating from an orifice that appeared to be the appendiceal opening (Figure 3).
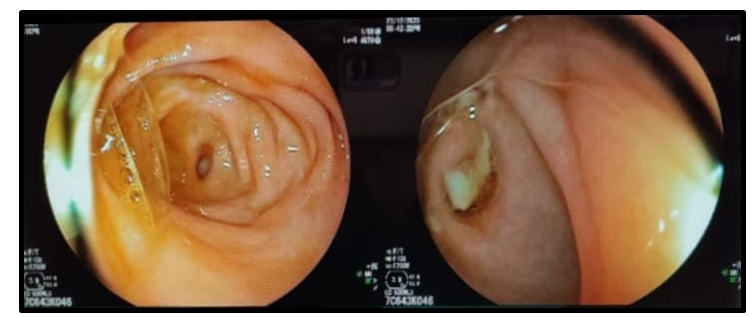
Through a combination of clinical data, imaging studies, and endoscopic examination, we concluded a definitive diagnosis of a hepatic abscess secondary to an appendiceal phlegmon.
Discussion
Hepatic abscesses are an exceedingly rare condition, affecting only about 0.0023% of the population [3]. A pyogenic hepatic abscess caused by a complication of appendicitis, such as an appendiceal phlegmon, is even rarer. Literature reports variable incidence regarding the causes of pyogenic hepatic abscesses. One study found that appendicitis accounts for only about 1% of pyogenic liver abscesses [3], whereas another suggests it may account for up to 10% [4]. Patients developing such abscesses are, on average, 62 years old, with a higher prevalence among men than women (3.3 vs. 1.3 per 100,000) [3].
The clinical presentation of hepatic abscesses varies based on the infection source, but common symptoms include fever, chills, abdominal pain, and may also involve nausea, vomiting, and weight loss.³ In patients presenting with right lower quadrant pain and mass, differential diagnoses should include a wide range of conditions from benign and self-limiting pathologies to malignancies and those necessitating urgent surgical intervention. Given that such patients may exhibit ambiguous clinical presentations, which may mimic neoplasia, as in our case, a thorough and detailed patient history is crucial.
Untreated appendicitis can lead to perforation, resulting in either localized or generalized peritonitis. However, when the body partially controls this infection, an appendiceal phlegmon may form in approximately 10% of cases [5, 6]. An appendiceal phlegmon is a mass formed by surrounding tissues confining the infection near a perforated appendix.
Currently, there is no consensus on the definitive treatment for appendiceal phlegmon, with ongoing controversy regarding the optimal therapeutic approach. On one hand, immediate surgery carries a risk of complications, while conservative treatment is another option [6, 7]. In cases complicated by hepatic abscess, treatment includes targeted antibiotic therapy based on the initial infectious source and typical pathogens, as well as hepatic abscess drainage. Drainage options include percutaneous catheter placement or surgical drainage (open surgery), should percutaneous methods fail. A laparoscopic approach is also an alternative to traditional surgery.
Our patient was treated with antibiotics and abscess drainage via multipurpose catheter placement using the Seldinger technique. A sample of purulent fluid was sent for culture and sensitivity testing.
Culture results revealed:
- Klebsiella pneumoniae: Resistant to all cephalosporins, ciprofloxacin, ertapenem, imipenem, and meropenem; intermediate sensitivity to amikacin; sensitive to tigecycline.
- Escherichia coli (ESBL): Sensitive to imipenem, meropenem, and trimethoprim-sulfamethoxazole.
With a final procalcitonin level of 0.5 ng/mL, antibiotic therapy was discontinued on the fifth day post-drainage placement, and the patient was discharged in good condition with the drain in place. The drain was removed one month later after confirming with an abdominal ultrasound that the liver was of normal size, with regular borders and homogeneous parenchyma, and that no free fluid or collections were observed at the time of evaluation.
Conclusion
This elderly patient presented with right lower quadrant pain and a palpable mass, mimicking an ambiguous clinical picture. Thus, obtaining a comprehensive patient history and considering the possibility of a rare cause of hepatic abscess, in this case as a complication of acute appendicitis, were essential for timely diagnosis and treatment. Sharing this clinical case highlights the importance of recognizing such rare presentations.
References
-
Moreira VF, Garrido E (2014) Gastroenterology Service. Ramón y Cajal University Hospital. Rev Esp Enferm Dig 106(5).
-
Brunicardi F (2006) Capítulo 30: El hígado. Principles of Surgery. In: 8th (Edn.), Schartz.
-
Kaplan GG, Gregson DB, Laupland KB (2004) Population- based study of the epidemiology of and the risk factors for pyogenic liver abscess. Clin Gastroenterol Hepatol 2(11): 1032-1038.
-
Manabe S, Yasuoka T, Endo Y, Usui F, Yamaguchi T, et al. (2017) A case of liver abscess caused by appendicitis which was considered to be drained from hepatobronchial fistula. Nihon Shokakibyo Gakkai Zasshi 114(6): 1015-1022.
-
Humes D, Simpson J (2006) Acute appendicitis. BMJ 333(7567): 530-534.
-
Brainsky A, Salamanca E, Bonilla E, Varón C, Roa J, (2004) Controversies in the management of plastron and appendicular abscess: a case report. Rev Colomb Cir 19(3): 190-194.
-
Wray CJ, Kao LS, Millas SG, Tsao K, Ko TC (2013) Acute apendicitis: Controversies in diagnosis and management. Curr Probl Surg 50(2): 54-86.
- Management of Chronic Insertional Achilles Tendinopathy Using Flexor Hallucis Longus Tendon Transfer in Patients Over 50 Years of Age: A Four-Case Series Following the CARE Guidelines
- Application of Induced Pluripotent Stem Cells in Bone Tissue Engineering: Current Status and Prospects
- Surgical Management of Upper Thoracic Esophageal Squamous Cell Carcinoma with Concomitant Hypersplenism: Integration of Chai's Supra-Thoracic Apex Technique with Laparoscopic Splenectomy - A Technical Innovation Case Study with Systematic Review
- Evaluation of Masticatory Functional Efficiency of Stomatognathic System in Patients Undergoing Open Reduction Internal Fixation for Treatment of Pan-Facial Trauma: A Prospective Study
- Report of Lumboperitoneal (LP) Shunt Procedure in Over Decades Experiences, Systematic Narrative Review
- Encasement of Ventral Hernia Mesh within Small Bowel: A Case Report