Management of Chronic Insertional Achilles Tendinopathy Using Flexor Hallucis Longus Tendon Transfer in Patients Over 50 Years of Age: A Four-Case Series Following the CARE Guidelines
Introduction: Chronic insertional Achilles tendinopathy is a debilitating condition, particularly in patients over 50 years of age, due to progressive degenerative changes. When conservative management fails, transfer of the flexor hallucis longus (FHL) tendon has emerged as a reliable surgical option. This study aimed to describe the surgical technique and present clinical outcomes in four patients, in accordance with the CARE guidelines. Results: Four female patients (51-71 years) with chronic insertional Achilles tendinopathy unresponsive to conservative treatment underwent calcification resection, distal Achilles tendon reinsertion, and FHL transfer. At 12 months, all patients showed marked clinical improvement, with pain resolution, restored plantarflexion, and significant gains in AOFAS (American Orthopaedic Foot and Ankle Society) scores. Conclusion: FHL tendon transfer for chronic insertional Achilles tendinopathy in patients over 50 provides excellent functional recovery, substantial pain relief, and demonstrates a favourable safety profile with no major complications.
Introduction
Chronic insertional Achilles tendinopathy causes significant pain and functional impairment, associated with weakness of the posterior muscle group [1]. In patients over 50 years of age, the Achilles tendon shows increased degenerative and inflammatory changes [2]. Flexor hallucis longus (FHL) tendon transfer, combined with Achilles tendon debridement and partial calcaneal tuberosity osteotomy, improves plantarflexion strength [3], effectively fills tendon substance loss [4], and provides well-vascularized tissue to the critical avascular zone located 2-6 cm proximal to the calcaneal insertion, promoting graft integration [5]. Some studies report significant functional improvement following FHL augmentation [2, 6], while others show comparable outcomes without augmentation [3]. In this case series, we focused on the FHL augmentation technique in patients over 50 years, with a 12-month follow-up. Informed consent was obtained, and reporting adhered to SCARE guidelines [7].
Case reports
Case 1
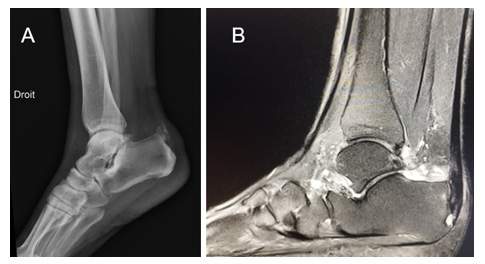
A 71-year-old female presented with a two-year history of chronic right heel pain, associated with persistent gait impairment. Radiographs and MRI performed two years prior revealed a calcific insertional Achilles tendinopathy of the right tendon (Figure 1). Clinical examination demonstrated tenderness at the Achilles tendon insertion, posterior swelling, and plantarflexion deficit. The preoperative AOFAS score was 45.
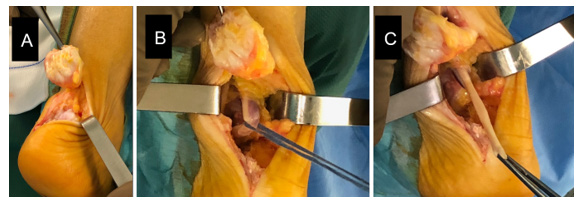
Following failure of conservative management, the patient underwent calcification excision with distal Achilles tendon reinsertion combined with the FHL tendon transfer under general anesthesia, in the prone position with a thigh tourniquet. Via a medial para-Achilles approach, the tendon sheath was opened, the Achilles tendon detached, and the calcific lesion excised. The FHL tendon was identified, looped, and sectioned distally with the ankle in equinus (Figure 2). A 6-mm blind tunnel was drilled anterior to the native Achilles insertion, and the graft was fixed using an interference screw. The Achilles tendon was reinserted posterior to the graft on four anchors using a double-row speed-bridge construct. Postoperatively, the limb was immobilized in a non–weight-bearing equinus cast for three weeks, followed by a removable boot with weight-bearing. Physical therapy focusing on ankle mobilization was initiated at six weeks. At six months, plantarflexion was restored, gait was pain-free, and AOFAS scores were 82 and 99 at six and twelve months, respectively (Figure 3).

Case 2
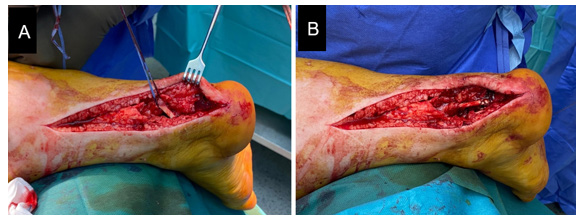
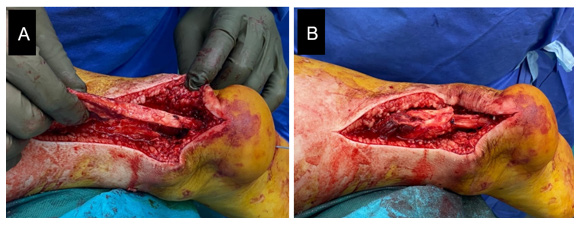
A 56-year-old female presented with chronic right hindfoot pain. The preoperative AOFAS score was 35. Initial imaging revealed a large calcification of the distal Achilles tendon, including its insertion. Surgical management consisted of calcification excision with distal Achilles tendon reinsertion combined with the FHL tendon transfer, performed by the same surgical team. Through a medial para-Achilles approach, the tendon sheath was opened, the Achilles tendon detached, and the calcification excised (4 cm longitudinal × 2.5 cm transverse; (Figure 4). The deep aponeurosis was opened, the FHL tendon identified, looped, and sectioned distally with the ankle in equinus. The distal portion was prepared with whipstitching, and a 6-mm blind tunnel was drilled. The graft was passed and fixed with an interference screw (Figure 5). Due to substantial tendon loss following excision, a quadriceps tendon graft was harvested. A second tunnel was drilled at the calcaneal tuberosity, and the quadriceps graft was sutured proximally to the remaining Achilles tendon stump and reinserted distally on four anchors using a double-row speed-bridge construct (Figure 6). Postoperative management was identical to case 1. At three weeks, the surgical wound was fully healed. At twelve months, the patient was pain-free, and AOFAS scores were 84 and 95 at six and twelve months, respectively.

Case 3
A 51-year-old female presented with chronic left hindfoot pain, localized to the Achilles tendon insertion. The preoperative AOFAS score was 61. Initial imaging revealed a posterior calcaneal tuberosity exostosis consistent with Haglund’s deformity, along with calcifications at the Achilles tendon insertion. Surgical management consisted of excision of the calcaneal tuberosity and calcifications, distal Achilles tendon reinsertion, and FHL tendon transfer. The procedure was performed using the standardized technique described for previous cases, including Achilles tendon brushing. Postoperative recovery was uneventful, with no complications. AOFAS scores at six and twelve months were 95 and 97, respectively.
Case 4
A 57-year-old female presented with chronic left hindfoot pain. She had previously undergone surgery 11 months earlier for Haglund’s deformity, including resection of the calcaneal tuberosity and Achilles tendon brushing. Clinical evolution was marked by persistent pain (preoperative AOFAS score 65), and imaging revealed distal tendon calcifications associated with a large calcaneal spur. Revision surgery was performed, consisting of excision of the calcaneal spur and tendon calcifications, distal Achilles tendon reinsertion, and FHL tendon transfer, using the standardized technique applied in the other cases. Postoperative recovery was uneventful. AOFAS scores at six and twelve months were 97 and 99, respectively The chronological sequence of events is summarized in Table 1.
| Period or context | Event | Details |
|---|---|---|
| • Chronic pain in the right hindfoot • Failure of conservative treatment | Clinical examination | • Severe right heel pain with persistent gait impairment • Tenderness at the Achilles tendon insertion + posterior swelling + plantarflexion deficit • AOFAS score: 45(P1), 35(P2), 61(P3), 65(P4) |
| Lateral radiograph + ankle sagittal DP Fat Sat MRI) | • Opacity in the posterosuperior aspect of the calcaneal tuberosity (P1, P2, P3, P4) and within the tendon (P2) • Hyperintensity within the tendon at its insertion site | |
| Diagnosis | Insertional Achilles tendinopathy | |
| Surgery | Calcification excision with distal Achilles tendon reinsertion combined with the FHL tendon transfer | • General anesthesia, prone position, thigh tourniquet • Medial para-Achilles approach. • Opening of the tendon sheath, detachment of the Achilles tendon and excision of the calcification. Distal section of the FHL tendon with the ankle in equinus position • Fixation of the graft with an interference screw, placed anterior to the tendon, into a 6-mm blind tunnel located anterior to the Achilles tendon. • Reinsertion of the Achilles tendon using four anchors with a double-row SpeedBridge-type construct • Specificity of P2: given the loss of tendon substance after resection of the large calcification, the quadriceps tendon was harvested, sutured proximally to the remaining Achilles tendon stump, and distally reinserted using four anchors mounted with sutures in a double-row SpeedBridge-type configuration • Specificity of P3 and P4: Achilles tendon combing (longitudinal tenotomy), in addition to the standard procedure, due to Haglund’s disease |
| Postoperative period | Rehabilitation | • Below-knee cast in equinus position without weight- bearing (3 weeks) • Then a removable boot with weight-bearing (3 weeks). • Physiotherapy starting from the 6th week |
| At six months | Follow-up | • Normal plantar flexion • Painless gait |
| At six and twelve months | Scores AOFAS at 6-12 months | • 82-99(P1), 84-95 (P2), 95-97(P3), 97-99(P4) |
Table 1: Timeline of clinical events.
P1: first patient P2 : second patient P3 : third patient P4: fourth patient FHL : Flexor hallucis longus Table 1: Timeline of clinical events.
Discussion
The Achilles tendon is composed of fibers from the gastrocnemius and soleus muscles and serves as the primary ankle plantar flexor [8]. Its vascularization relies on the paratenon, but in cases of overuse, blood flow to the critical zone located 2–6 cm proximal to its insertion may be compromised, leading to tendon injury and fibrosis [2, 9]. Chronic insertional Achilles tendinopathy is associated with irreversible fibrous degeneration [10, 11]. FHL tendon transfer is frequently performed to reinforce tendon structure, enhance mechanical strength, and improve vascular supply [12]. Its neuromuscular activation is synchronized with the triceps surae, providing optimal support for normal gait mechanics [13, 14]. This procedure is indicated in cases of tendon substance loss greater than 50% and in patients over 50 years of age [15, 16, 17]. The FHL tendon is preferred over other grafts due to its length, durability, relative motor unit strength compared with other tendons (e.g., flexor digitorum longus), and anatomical proximity to the Achilles tendon [15]. The FHL has greater muscle mass and strength than the flexor digitorum longus and peroneal tendons, which are also used in the treatment of chronic Achilles tendinopathy [18]. Some authors perform a secondary medial approach at the forefoot, at the dorsal–plantar skin junction near the first metatarsal, to control the distal section of the tendon [2]. Proper graft tension is achieved with the ankle in dorsiflexion to place the Achilles tendon under maximal stretch. Once correctly tensioned, any excess length of the FHL is trimmed to ensure optimal pull of the transferred tendon.
The transfer of the FHL tendon is a minimally invasive procedure that generally yields favorable outcomes [19]. The comparison between FHL transfer combined with Achilles tendon debridement and debridement alone remains controversial: while some authors report no significant difference [5], others note improved functional outcomes and reduced pain in patients over 50 years of age [2]. Den Hartog et al. [20] observed a higher healing rate and marked improvement in AOFAS scores in 18 of 26 patients over 50 years old.
Conclusion
FHL tendon transfer combined with Achilles tendon debridement provides significant functional improvement and substantial pain relief in patients over 50 years with chronic insertional Achilles tendinopathy.
Authors contributions
Bizolé Balepna DY wrote the first draft and updated the article in accordance with the CARE guidelines. Nanema H and Baleng PN critically reviewed. Baroan C and Nieto H critically reviewed and contributed to the edition of the final version.
References
-
Howell MA, McConn TP, Saltrick KR, Catanzariti AR (2019) Calcific insertional Achilles tendinopathy- Achilles repair with flexor hallucis longus tendon transfer: case series and surgical technique. J Foot Ankle Surg 58(2): 236-242.
-
Sabaghzadeh A, Ghanbari N, Gholamshahi H, Zakeri AM, Shakeri Jousheghan S, et al. (2024) Does FHL Tendon Transfer Alter the Outcome of Haglund Deformity Treatment by Using Debridement and Ostectomy in Patients Older Than 50 Years? A Single-Blinded Randomized Controlled Trial. Foot Ankle Orthop 9(3): 1-7.
-
Hunt KJ, Cohen BE, Davis WH, Anderson RB, Jones CP (2015) Surgical treatment of insertional Achilles tendinopathy with or without flexor hallucis longus tendon transfer: a prospective, randomized study. Foot Ankle Int 36(9): 998-1005.
-
Tashjian RZ, Hur J, Sullivan RJ, Campbell JT, DiGiovanni CW (2003) Flexor hallucis longus transfer for repair of chronic achilles tendinopathy. Foot Ankle Int 24(9): 673- 676.
-
Thermann H, Hüfner T, Tscherne H (2000) Achilles tendon rupture. Der Orthopäde 29: 235-250.
-
Lui TH (2007) Endoscopic assisted flexor hallucis tendon transfer in the management of chronic rupture of Achilles tendon. Knee Surg Sports Traumatol Arthrosc 15(9): 1163-1166.
-
Kerwan A, Al Jabir A, Mathew G, Sohrabi C, Rashid R, et al. (2025) Revised surgical Case Report (SCARE) guideline: an update for the age of artificial intelligence. Premier J Sci 10: 100079.
-
Chimenti RL, Cychosz CC, Hall MM, Phisitkul P (2017) Current concepts review update: insertional Achilles tendinopathy. Foot Ankle Int 38(10): 1160-1169.
-
Wang J, Zeng X, Ma X (2020) Advance of diagnosis and treatment of Haglund syndrome. Chin J Repar Reconstr Surg 34(4): 518-523.
-
Benca E, Willegger M, Wenzel F, Hirtler L, Zandieh S, et al. (2018) Biomechanical evaluation of two methods of fixation of a flexor hallucis longus tendon graft. Bone Jt J 100(9): 1175-1181.
-
Vaishya R, Agarwal AK, Azizi AT, Vijay V (2016) Haglund’s syndrome: a commonly seen mysterious condition. Cureus 8(10): e820.
-
Maffulli N, Gougoulias N, Christidis P, Maffulli GD, Oliva F (2023) Primary augmentation of percutaneous repair with flexor hallucis longus tendon for Achilles tendon ruptures reduces tendon elongation and may improve functional outcome. Knee Surg Sports Traumatol Arthrosc 31(1): 94-101.
-
Perry J (1992) Ankle Foot Complex. In: Perry J, Burnfield JM (Eds.), dir. Gait Analysis: Normal and Pathological Function. Slack Inc, Thorofare, USA, pp: 51-87.
-
Hahn F, Meyer P, Maiwald C, Zanetti M, Vienne P (2008) Treatment of chronic Achilles tendinopathy and ruptures with flexor hallucis tendon transfer: clinical outcome and MRI findings. Foot Ankle Int 29(8): 794-802.
-
Schon LC, Shores JL, Faro FD, Vora AM, Camire LM, et al. (2013) Flexor hallucis longus tendon transfer in treatment of Achilles tendinosis. J Bone Jt Surg 95(1): 54-60.
-
El Tantawy A, Azzam W(2015) Flexor hallucis longus tendon transfer in the reconstruction of extensive insertional Achilles tendinopathy in elderly: an improved technique. Eur J Orthop Surg Traumatol 25(3): 583-590.
-
Maffulli N, Saxena A, Wagner E, Torre G (2019) Achilles insertional tendinopathy: state of the art. J Int Soc Arthrosc Knee Surg Orthop Sports Med 4(1): 48-57.
-
Alhaug OK, Berdal G, Husebye EE, Hvaal K (2019) Flexor hallucis longus tendon transfer for chronic Achilles tendon rupture. A retrospective study. Foot Ankle Surg 25(5): 630-635.
-
Maffulli N, Del Buono A, Loppini M, Denaro V (2014) Ipsilateral free semi-tendinosus tendon graft with interference screw fixation for minimally invasive reconstruction of chronic tears of the Achilles tendon. Oper Orthop Traumatol 26(5): 513-519.
-
Den Hartog BD (2009) Insertional Achilles tendinosis: pathogenesis and treatment. Foot Ankle Clin 14(4): 639- 650.
- Application of Induced Pluripotent Stem Cells in Bone Tissue Engineering: Current Status and Prospects
- Surgical Management of Upper Thoracic Esophageal Squamous Cell Carcinoma with Concomitant Hypersplenism: Integration of Chai's Supra-Thoracic Apex Technique with Laparoscopic Splenectomy - A Technical Innovation Case Study with Systematic Review
- Evaluation of Masticatory Functional Efficiency of Stomatognathic System in Patients Undergoing Open Reduction Internal Fixation for Treatment of Pan-Facial Trauma: A Prospective Study
- Hepatic Abscess Secondary to Appendiceal Phlegmon an Unusual Complication of Appendiceal Phlegmon
- Report of Lumboperitoneal (LP) Shunt Procedure in Over Decades Experiences, Systematic Narrative Review
- Encasement of Ventral Hernia Mesh within Small Bowel: A Case Report