Evaluation of Masticatory Functional Efficiency of Stomatognathic System in Patients Undergoing Open Reduction Internal Fixation for Treatment of Pan-Facial Trauma: A Prospective Study
There is limited literary knowledge about masticatory functional efficiency post-intervention in patients with panfacial trauma. The aim was to evaluate the masticatory functional efficiency of the stomatognathic system in patients with panfacial fractures preoperatively and postoperatively. This prospective study had two groups. Group 1 (n=20) consisted of patients with panfacial fractures. Group 2 (n=20) consisted of healthy volunteers. Mean Maximum Voluntary Bite Force (MVBF) of the Group 1 was recorded. Preoperative MVBF of Group 2 subjects was recorded. Postoperatively the MVBF was recorded in Group 2 subjects at 1 week, 1 month, 3 months and 6 months. Group 2 subjects were asked to answer a pre-validated, modification of OHIP-14 questionnaire 6 months postoperatively. It was concluded that patients regained masticatory functional efficiency comparable to that of normal healthy volunteers by 6 th postoperative month with significant improvement in quality of life. Intraoperative factors such as amount of periosteal bone stripping and number of muscle attachments released can have a negative impact on the patients’ masticatory efficiency in the long run.
Abbreviations
ORIF: Open Reduction Internal Fixation; MVBF: Maximum Voluntary Bite Force; OHIP: Oral Health Impact Profile; SPSS: Statistical Product and Service Solutions.
Introduction
The craniofacial skeleton has an important role in the functions of chewing, speech, sight, smell, breathing, and aesthetics. Various factors affect chewing efficiency, such as bite force, dental occlusion, mandibular movements and tongue and saliva activity [1]. Masticatory function is the ability of a person to masticate or chew without pain or interference. Determinants of masticatory function are the range of mandibular motion, occlusion, maximum occlusal forces, and the activity of masticatory muscles. This function is affected in dentofacial abnormalities and in traumatic and pathological injuries to the jaws [2].
Panfacial craniofacial fractures are defined as: Fractures that coexist in cranio-orbital area (upper third) and orbito- zygomatic-maxillary area (middle third) of the face and in the mandibular (lower third) areas of the craniofacial unit [3]. Markowitz and Manson had defined them as fractures that involve all three subunits of the face. Some of the authors include patients with fractures at only two levels also to be called as panfacial injury [4]. They occur when there is a high impact injury to the facial skeleton like high-speed collisions of motor vehices [5].
Historically, the panfacial fractures were mainly treated conservatively. This led to various postoperative problems, like gross malocclusion, considerable increase in facial width, decreased facial projection, alteration in facial height and so on. Improper occlusion should not be underestimated because the way the teeth come together can be detected by the patient far more easily and it is very disturbing for the patient.
Such a malocclusion can have deleterious effects on the temporomandibular joint and not only reduces the masticatory efficiency of the stomatognathic system leading to malnutrition but also depreciates the patient’s overall quality of life. In the present times surgical intervention and open reduction of these complex fractures are commonly performed. Approach to the facial skeleton in cases with panfacial fractures should be based on wide exposure, adequate visualisation and adequate reduction. The type of surgical approach depends on the location of the fracture, severity of the facial injury, extent of the exposure required and amount of comminution present in the region [6]. Anatomic reduction is essential for precise three-dimensional reestablishment of facial height, width and projection. This restoration of anatomy also leads to restoration of function by means of normal masticatory efficiency [7].
During surgical treatment, soft tissue injury in the form of stripping of masticatory muscles and iatrogenic neurovascular injury can further affect the masticatory apparatus. All facets of form and function are important and the surgeon must try to preserve them. The restoration of the patient’s occlusion is considered one of the keys of determining correct reduction. Despite occlusal position being restored surgically, it is unknown whether the patient might be able to produce occlusal loads similar to that of normal individuals, due to the fractures and/or its surgical treatment [8].
Maximum occlusal forces are an important parameter of masticatory function and also are relatively easy to measure and analyse. Thus, in patients treated surgically for facial skeletal fractures, records of maximum occlusal forces act as a very effective objective assessment criteria for restoration of skeletal architecture of the bony buttresses and repair and healing of masticatory soft tissues [9].
The influence of pan-facial trauma and the treatment of injury on a patient’s quality of life should be assessed by the surgeon to determine the overall outcome of the treatment [10]. By determining the time period that is required for patients to attain normal maximum occlusal forces we can also establish the duration that would be required for the patient to achieve normal masticatory efficiency and by extention we can ascertain the exact duration for which the patient would suffer from poor oral intake in the postoperative phase. It is an important factor for the operating trauma surgeon to be aware of the duration of the postoperative convalescence period in which the nutritional intake of the patient would be below optimum levels in order to correct the nutritional deficits.
In the existing literature there are mainly studies that evaluated the bite force of patients who have sustained mandibular fractures and were treated for the same. There is a paucity of research evaluating the effect of panfacial fractures on bite forces. The aim of this study was to determine the masticatory functional efficiency of patients treated surgically for panfacial trauma and to evaluate the long-term quality of life of such cases.
Materials and Methods
Ethical approval had been given by the Institutional Ethical Committee to carry out this research and the ethical approval number assigned to the study was IEC/03/21. This was a prospective analytical study in which 20 randomly selected patients with panfacial fractures (Group 1) were scrutinized and 20 randomly selected healthy volunteers with normal occlusion (Group 2) between the ages of 18 years to 40 years were selected as a comparative group. The sample for Group 1 were selected considering the following points in mind;
- all individuals were patients reporting with panfacial trauma,
- not having dentoalveolar fractures,
- were fit to undergo ORIF under necessary anesthesia and
- were of age 18 years and above. Patients with osteoarthritis and connective tissue disorder of temporomandibular joint, systemic illness or immunocompromised conditions were excluded from the study. Patients who were partially or completely edentulous patients or undergoing orthodontic treatment were excluded from the study. Patients with traumatic brain injury were also excluded. All the patients reported to our ‘Out Patient Department’ within one week after sustaining their trauma and none of the patients had concurrent thoracic, abdominal, cervical spine or long bone injuries. Demographic data and the description of the pattern of facial fractures of the subjects in Group 1 are outlined in Table 1.
| Sr. No. | Age/ Sex | Fractures Sustained |
|---|---|---|
| 1 | 24yr/M | B/L Le Fort III #. |
| 2 | 30yr/M | B/L ZMC #, Rt. Parasymphysis #. |
| 3 | 26yr/M | Rt. ZMC #, Lt. Le Fort I #, Lt. Parasymphysis #. |
| 4 | 34yr/M | Lt. ZMC #, Rt. Le Fort II #, Symphysis #, Lt. Condyle #. |
| 5 | 27yr/F | NOE complex #, Frontal bone #, Lt. Condyle #. |
| 6 | 22yr/M | Frontal bone #, Left ZMC #, Rt. Le Fort I #. |
| 7 | 40yr/M | B/L Angle #, Rt. ZMC #, Lt. Le Fort II #. |
| 8 | 36yr/M | Rt. ZMC #, Lt. Le Fort I #, Lt. Parasymphysis #. |
| 9 | 22yr/M | B/L ZMC #, B/L Condyle #, Symphysis #. |
| 10 | 31yr/M | B/L Angle #, Lt. ZMC #, Rt. Le Fort I #. |
| 11 | 29yr/M | Rt. Angle #, Lt. Ramus #, Rt. ZMC #, Lt. Le Fort I #. |
| 12 | 32yr/M | B/L Le Fort III #. |
| 13 | 33yr/M | B/L Le Fort III #, Rt. Angle #. |
| 14 | 21yr/M | Rt. Condyle #, Lt. Angle #, Rt. ZMC #, Lt. Le Fort I #. |
| 15 | 34yr/F | B/L ZMC #, Lt. Parasymphysis #. |
| 16 | 28yr/M | B/L Angle #, Rt. ZMC #, Lt. Le Fort II #. |
| 17 | 34yr/M | B/L ZMC #, Lt. Condyle #, Rt. Angle #, Symphysis #. |
| 18 | 26yr/M | Rt. ZMC #, Lt. Le Fort I #, Lt. Parasymphysis #. |
| 19 | 19yr/M | Lt. ZMC #, Rt. Le Fort II #, Symphysis # , Lt. Condyle #. |
| 20 | 27yr/M | Frontal bone #, Rt. ZMC #. |
Table 1: Details of panfacial trauma patients.
Thorough preoperative assessment of the panfacial trauma patients was performed and detailed case history was recorded describing the etiopathogenesis and date of the trauma sustained, along with details of and concurrent injuries sustained.
3DCT face imaging was obtained for all the patients on presentation after ruling out any other life-threatening injuries and if any, after instituting primary care. Preanesthetic check-up was done for all patients to undergo surgery under necessary anaesthesia and then the patients were planned for surgery.
The preoperative Maximum Voluntary Bite Force (MVBF) was recorded. In patients with restricted mouth opening the MVBF was considered as nil. The bite force sensor was first placed in the right molar region and the patient was asked to occlude for a period of 30 seconds. This was followed by the left molar region and incisor region. The MVBF of molar and incisor regions was averaged. The patients were asked to answer a modified, pre-validated translation of the OHIP-14 questionnaire preoperatively. Maximum Voluntary Bite Force (MVBF) in incisor and molar region was recorded of the 20 healthy volunteers. The bite force sensor was first placed in the right molar region and the patient was asked to bite down as hard as possible for a period of 30 seconds. This was followed by the left molar region and incisor region. The MVBF of molar and incisor regions was averaged. The mean of average MVBF of the healthy volunteer group was obtained.
Panfacial trauma patients underwent ORIF under necessary anaesthesia. Under necessary anaesthesia, with proper asepsis the patients were prepared and wide surgical exposure with the necessary approaches was achieved for adequate anatomic reduction. Sequences such as “Bottom Up and Inside Out” or “Top Down and Outside In” were used as deemed necessary for each individual case [8].
ORIF of the fractures was performed using titanium miniplates, titanium miniscrews and titanium meshs of the appropriate dimensions as required based on the individualized treatment planning of each case.
The variables such as stability of occlusion achieved, the number of individual bones with periosteal stripping and the number of muscle attachments (primarily masticatory muscles) released intraoperatively were recorded. MVBF of the patients was recorded then at the postoperative 1 week, 1 month, 3 months and 6 months.
The patients were asked to answer a modified, pre- validated translation of the OHIP-14 questionnaire again at the 6 month postoperative follow up appointment.
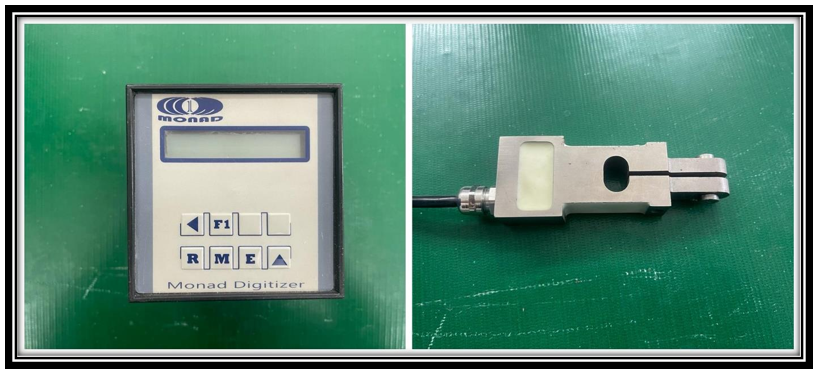
The armamentarium used to measure MVBF was a digital gnathodynamometer with a 1500 Newton capacity manufactured and supplied by Texon Corporation. The bite force sensor works on the principle of strain gauge technology.
Strain gauge transducers are devices that consist of aluminium alloy plates. These plates are attached with strain gauges and the assembly is connected to a wheaston bridge circuit. On loading these metal plates undergo deformation, due to which its resistance changes, which results in a change in electric potential or voltage.
This change in voltage can be calibrated with a known weight to indicate the applied load. The controller receives electric signals in mv/v from the sensor. The device consists of two main components, the sensor and the digital display unit which are depicted in Figure 1.
The sensor is hand held and is connected via a cable to the digital display unit. It is 12 mm in height and 150 mm long. This makes it easy for the patient to hold it in their hand, insert it in the mouth and apply pressure when instructed.
The digital display indicates the digital value of the pressure applied in Newtons unit. The appliance has a button for ‘set zero’ and a selector switch for the ‘peak’ option. The ‘set zero’ option allows the values obtained to be accurately controlled. The position peak records the greatest force applied during the test.When the patient bites on the bite points at the centre of the metal plates of the sensor, the maximum occlusal bite force of that chewing cycle is automatically recorded irrespective of the dynamic force shifts by the subject during biting.
To measure the postoperative quality of life a modified (for trauma patients), pre-validated version of the OHIP- 14 questionnaire was utilized which is shown in Figure 2. The Oral Health Impact Profile (OHIP-14) is a 14- items questionnaire designed to measure self-reported functional limitation, discomfort and disability attributed to oral conditions. The OHIP-14 is a self-filled questionnaire that focuses on seven dimensions of impact (functional limitation, pain, psychological discomfort, physical disability, psychological disability, social disability and handicap) with participants being asked to respond according to frequency of impact on a 5-point Likert scale coded never (score 0), hardly ever (score1), occasionally (score2), fairly often (score 3) and very often (score 4) [11].
![Figure 2: The Oral Health Impact Profile (OHIP-14) is a 14- items questionnaire designed to measure self-reported functional limitation, discomfort and disability attributed to oral conditions. The OHIP-14 is a self-filled questionnaire that focuses on seven dimensions of impact (functional limitation, pain, psychological discomfort, physical disability, psychological disability, social disability and handicap) with participants being asked to respond according to frequency of impact on a 5-point Likert scale coded never (score 0), hardly ever (score1), occasionally (score2), fairly often (score 3) and very often (score 4) [11].](/fulltextimages/13819/fig_2.png)
Results
All the data was recorded and statistical analysis was performed using Statistical Product and Service Solutions (SPSS) version 21 for Windows (Armonk,NY:IBM corp). Intragroup comparisons of maximum occlusal bite force measurements in patients of panfacial trauma at different time intervals was done using Repeated ANOVA test followed by Tukey’s post hoc test for multiple pair wise comparison. Unpaired ‘t’ test was used for intergroup comparison between study group and control group in relation to MVBF measurements.
MVBF
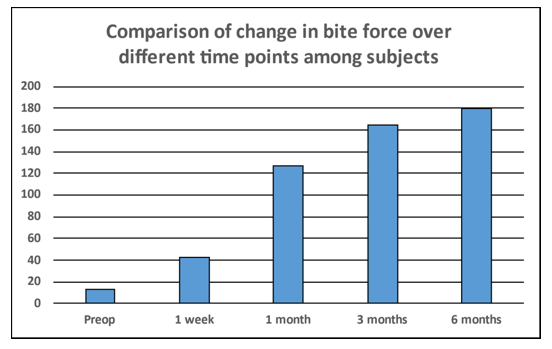
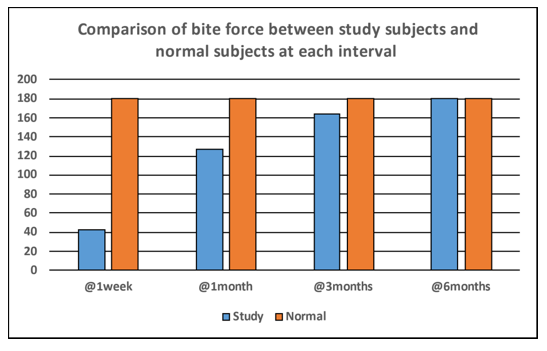
Comparison of change in MVBF over different time points among panfacial trauma patients was analysed using repeated measures of ANOVA test. A p≤0.05 was considered to indicate significant difference. The Comparison of change in MVBF over different time points which is depicted diagrammatically in Figure 3 shows that there was a significant increase in MVBF from preoperative interval to 6 months post-operative time interval. Multiple comparisons for change in MVBF over different time points among panfacial trauma patients was assessed using adjustments for multiple comparisons using Bonferroni test. A p≤0.05 was considered to indicate statistically significant difference. The comparison showed that there was a significant increase in MVBF from preoperative phase till 1 week postoperative interval, 1 month postoperative interval, 3 months postoperative interval and 6 months postoperative time interval. Also, increase in MVBF from 1 week postoperative interval to 1 month postoperative interval, and subsequently 3 months postoperative interval and 6 months postoperative time interval was significant. Comparison of MVBF between panfacial trauma patients and healthy volunteers was done at each interval using Independent t test considering that a p≤0.05 indicates statistically significant difference. This is represented diagrammatically in Figure 4. The comparison showed that after 1 week postoperative interval and 1 month postoperative interval, MVBF was significantly lesser in panfacial trauma patients as compared to healthy volunteers. After 3 months postoperative time interval, MVBF was lesser in panfacial trauma patients as compared to healthy volunteers; however, difference in MVBF among two groups was non-significant. After 6 months post-op interval, MVBF among two groups was almost similar (p=0.998).
OHIP- 14 Score
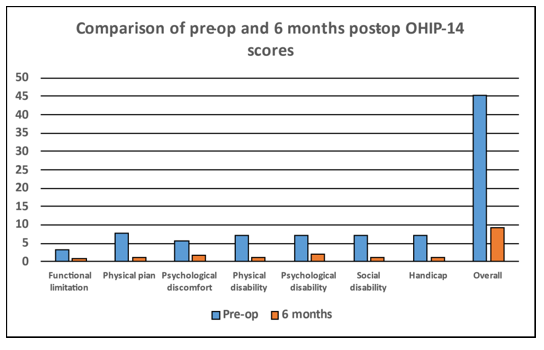
Comparison of Preoperative and postoperative OHIP- 14 scores was done using Paired t test and a p≤0.05 was considered to be a statistically significant difference. The comparison showed that there was a significant difference in OHIP-14 scores of all the domains and in the overall OHIP score which is represented graphically in Figure 5 and in tabular form in Table 2.
| Interval | Mean | SD | p value | |
|---|---|---|---|---|
| Functional limitation | Pre-op | 3.25 | 1.07 | <0.001* |
| Functional limitation | 6 months post-op | 0.95 | 0.22 | <0.001* |
| Physical plan | Pre-op | 7.8 | 0.41 | <0.001* |
| Physical plan | 6 months post-op | 1.15 | 0.67 | <0.001* |
| Psychological discomfort | Pre-op | 5.75 | 1.12 | <0.001* |
| Psychological discomfort | 6 months post-op | 1.8 | 0.62 | <0.001* |
| Physical disability | Pre-op | 7.25 | 0.44 | <0.001* |
| Physical disability | 6 months post-op | 1.1 | 0.31 | <0.001* |
| Psychological disability | Pre-op | 7.25 | 0.44 | <0.001* |
| Psychological disability | 6 months post-op | 2.05 | 0.39 | <0.001* |
| Social disability | Pre-op | 7.2 | 0.41 | <0.001* |
| Social disability | 6 months post-op | 1.1 | 0.31 | <0.001* |
| Handicap | Pre-op | 7.15 | 0.49 | <0.001* |
| Handicap | 6 months post-op | 1.05 | 0.22 | <0.001* |
| Overall | Pre-op | 45.3 | 2.54 | <0.001* |
| Overall | 6 months post-op | 9.2 | 1.8 | <0.001* |
Table 2: Comparison of pre-operative and 6 months post-operative OHIP-14 scores of panfacial trauma patients.
Paired t test; * indicates significant difference at p≤0.05 Table 2: Comparison of pre-operative and 6 months post-operative OHIP-14 scores of panfacial trauma patients.
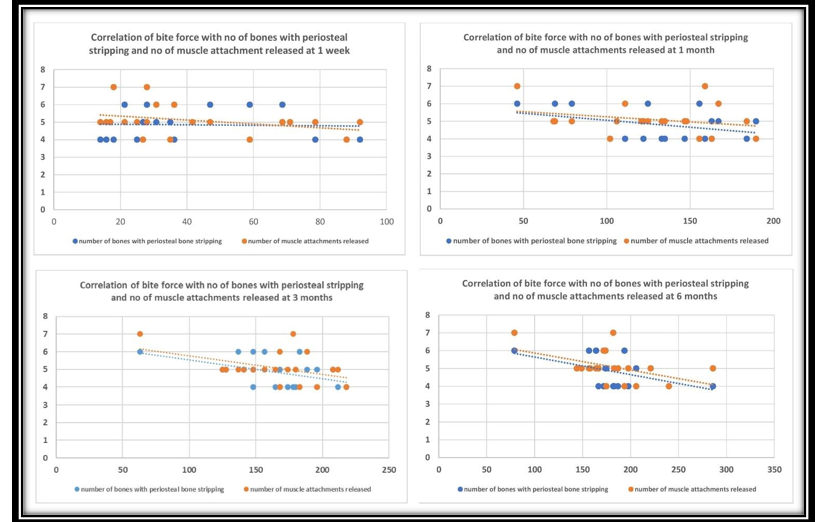
Periosteal stripping of number of bones and number of muscle attachments released
Descriptive details of the same are mentioned in Table 3. Correlation of MVBF with number of bones with periosteal stripping and number of muscle attachments released was analyzed using Pearson correlation test. A p≤0.05 was considered as a statistically significant correlation. This analysis is depicted in Table 4 and is graphically represented in Figure 6. There was no correlation between MVBF and number of bones with periosteal stripping and number of muscle attachments released after 1 week and 1month post-op interval. However, number of bones with periosteal stripping showed significant negative moderate correlation with MVBF after 3 months and 6 months i.e. increase in number of bones with periosteal stripping significantly reduced the MVBF after 3 months and 6 months. Similarly, increase in number of muscle attachments released significantly reduced the MVBF after 6 months.
| N | Minimum | Maximum | Mean | SD | |
|---|---|---|---|---|---|
| No of bones with periosteal stripping | 20 | 4 | 6 | 4.85 | 0.81 |
| No of muscle attachments released | 20 | 4 | 7 | 5.1 | 0.85 |
Table 3: Descriptive details of number of bones with periosteal stripping and number of muscle attachments released.
| No of Bones with Periosteal Stripping | No of Muscle Attachments Released | |
|---|---|---|
| 1 week | -0.045 | -0.328 |
| 1 month | -0.39 | -0.272 |
| 3 months | -0.472* | -0.437 |
| 6 months | -0.500* | -0.461* |
Table 4: Correlation of MVBF with number of bones with periosteal stripping and number of muscle attachments released.
Pearson correlation test; * indicates significant correlation at p≤0.05 Table 4: Correlation of MVBF with number of bones with periosteal stripping and number of muscle attachments released.
Discussion
In our study the mean MVBF of the healthy volunteer group was found to be 180N. Bite force results from the action of the jaw elevator muscles which is determined by the central nervous system and feedback from muscle spindles, mechanoreceptors and nociceptors modified by the craniomandibular biomechanics [12]. Shushma G, et. al. [13] stated that the functional state of the masticatory system is best assessed by evaluating the bite force. Raustia AM, et. al. [14] in their study found that in patients with upper and middle third facial fractures, a return to preoperative parameters was observed after 1 year of observation and chewing improved following bilateral condylar fracture for up to 6 months after treatment, although changes were observed for up to 3 years. Varga S, et. al. [15] state that large variations in human bite force have been recorded in the first molar area, some of which can be explained by the fact that the studies have been performed on different populations, or by the difference in measuring instruments and techniques. Due to this high amount of variability in MVBF in even normal population it was deemed necessary to determine our own set parameters for ‘normal MVBF’ by using our own gnathodynamometer in a group of healthy volunteers rather than using a reference range of normal MVBF from the existing data pool, in order to minimize bias. In our study the mean preoperative MVBF was found to be 13.05 N with a Standard Deviation (SD) of 10.58 N. There are no studies in the literature which state what the MVBF would be in an untreated panfacial trauma patient. It can and should be logically assumed although, that the masticatory efficiency of a patient with multiple facial fractures including especially the maxilla and the mandible would be negligible.
The same has been objectively proven in our study. At 1 week postoperatively we recorded a mean MVBF of 42.09 N with a SD 25.17 N and at 1 month, 3 months and 6 months, the mean MVBFs’ were recorded at 126.47 N with SD 39.68 N, 164.23 N with SD 35.96 N and 179.95 N with SD 41.07 N respectively. This shows a steady significant rise in bite forces and therefore masticatory efficiency at each time interval as compared to the preoperative values. There was also a significant increase in MVBF at the 6 month follow up as compared to the early postoperative values, the 6 monthly mean MVBF being closely similar to that of the healthy volunteer group. As there is no literature published in the existing data pool which have evaluated the postoperative masticatory functional efficiency of panfacial trauma patients, our work is quite distinctive. There are some studies where bite force was measured in isolated mandibular fractures. Kshirsagar R, et. al. [2] conducted a study where they measured the amount of bite force generated by patients treated for parasymphyseal fractures of the mandible by open reduction and internal fixation at various predetermined time intervals. In their study restoration of functional bite forces was evident by 6 to 8 weeks. However, the restoration of maximum bite forces may require up to 12 weeks in parasymphyseal fractures [2].
Sybil D, et. al. [5] found that maximum bite forces in patients with mandibular fractures were significantly less than in controls for several weeks after surgery. After the ninth postoperative week, the maximum bite force measured < 65% the normal in patients with isolated angle fractures and > 80% the normal in patients with isolated parasymphysis fractures. The same values reduced to < 60% in patients with fractures of angle and parasymphysis and < 70% in patients with fractures of parasymphysis and condylar complex. An inverse relationship was found between the bite force values and the number of fractures of the mandible in their study. The authors also found lower bite forces and longer period for normalization in patients who had fractures in those regions of the mandible which are more significantly associated with the masticatory apparatus for example angle or condyle of the mandible [5]. In our study by the 6th postoperative month the patients with panfacial fractures could generate MVBF values similar to that of healthy volunteers. The MVBF values at the 3rd postoperative month were significantly higher than those at the postoperative 1 month and much more so than the values achieved at just 1 week postoperatively.
This indicates a steady rise in the masticatory efficiency in the convalescence period all the way until the 6th postoperative month. Upon examining the findings in our study, it can be unequivocally stated that a time duration of about 6 months is required for panfacial trauma patients to regain normal masticatory functional efficiency. This observation in our study adds empirical evidence to the existing knowledge in this particular field of research. Moreover, this observation is very clinically relevant because it gives operating trauma surgeons an estimate of the duration of their patients’ recouperation period. This adds to the knowledge and understanding of operating surgeons and also gives them relevant data that they can share with their patients to give them a clearer picture of their postoperative prognosis. We get a more realistic understanding of the postoperative trauma patients’ nutritional status from this, as this too depends on the patients’ masticatory efficiency. The nutritional status of the patient is integral to the holistic care of the patient and the trauma team must be cognizant of the effects of compromised nutritional status during the healing phase and measures to correct these deficits must be undertaken [16].
The duration for which special attention must be paid to the monitoring of nutritional status can be estimated from the findings of this study. All of these findings are very pertinent and shed light on extremely relevant clinical scenarios. Finally, as is the dynamic and evolving nature of the surgical field we can endeavour to improve upon the current surgical trends to try to change the current reality into a more favourable one, where possibly masticatory efficiency can be achieved even sooner. This opens a new door into auditing contemporary surgical methods and also for objectively measuring the effectiveness and benefits of any future innovations or modifications to the management of panfacial trauma patients. The authors believe that the scope for further research along this path is limitless. The effect of periosteal stripping on the overall functioning of the masticatory apparatus is an unexplored arena of research. With no studies of this nature being found in human subjects there only exist in vivo animal based studies on the topic of the effect of periosteal stripping on bone. These studies also mainly focus in the outcome of vascularity of the bony cortices [17]. It is indeed a fascinating approach to study the effect it could have on human subjects particularly in patients with panfacial trauma. No studies evaluating the effect of facial fracture treatment on the muscles of mastication could be found in the literature. However, there is research that has analysed the muscles of mastication in other clinical situations, such as studies related to orthognathic surgery after mandibular advancement.
In these studies, a return to preoperative parameters was observed after 1 year of observation, and chewing improved following bilateral condylar fracture for up to 6 months after treatment, although changes were observed for up to 3 years [6, 18, 19, 20]. The authors observed that the assessment of the corelation between number of bones with periosteal stripping and release of muscle attachments with MVBF does not seem to hold much significance in the initial postoperative phase. It is only by the 3 month and especially the 6 month postoperative phase that this relation becomes apparent that the increase in the amount of periosteal stripping and increase in number of muscle attachments released leads to a lowering of the MVBF. From this one can infer that it would be prudent to rely on minimally invasive techniques to perform the ORIF. Patients who sustain facial trauma suffer significant long-term health-related quality of life consequences stemming from their injuries [21].
Quality of life is currently considered an important marker for assessment in oral health studies. Quality of life is defined as an individual’s perception of their position in life in the context of the culture and value systems in which they live and in relation to their goals, expectations, standards and concerns [22]. There is no dearth of questionnaires for assessing quality of life in the literature with various of them having been used in studies and a classification of these questionnaire tools has also been mentioned in a study by Tan PG, et. al [23] which is based on the specific quality of life aspect assessed. In the existing literature there are only studies that evaluated the quality of life in patients who have sustained mandibular fractures, or midface fractures and their goals have also been of a comparative nature to analyse either conservative management against surgical intervention or to pitch two treatment modalities against each other.
There are no studies in the literature which have evaluated the effect of panfacial fractures and its treatment on the quality of life. The Oral Health Impact Profile (OHIP) questionnaire is one of the most commonly used instruments to assess quality of life; it has been used in various studies across different cultures. and socio- demographic profiles. The OHIP was developed in order to provide a comprehensive measurement of the dysfunction, discomfort, and disability associated with oral conditions as reported by the individual. OHIP analyses the different dimensions of functional patterns. These dimensions are functional limitation (e.g., difficulty chewing), pain (e.g., sensitivity of teeth), psychological discomfort (e.g., personal embarrassment), physical disability (e.g., changes in diet), psychological disability (e.g., reduced concentration), social disability (e.g., avoiding social contact), and incapacitation (e.g., being unable to work productively).
However, very few studies have investigated this issue in patients with facial trauma [24]. Conforte JJ, et. al. [25] developed a validated version of the OHIP-14 questionnaire specifically for facial trauma patients wherein the original OHIP-14 questions underwent minor adaptation: the words ‘‘their teeth and dentures’’ were replaced with the words ‘‘after suffering facial trauma’’ and ‘‘after surgical treatment’’. A translation of the same questionnaire was used in our study. OHIP-14 can be considered one of the best detectors of the psychosocial impact in a population. The scores of the OHIP-14 index range from 0 to 56 with 0 indicating the highest quality of life and 56 indicating the inverse. In our study the preoperative mean OHIP-score of the panfacial trauma patient group was 45.30 with a SD of 2.54 and mean 6 month postoperative score was 9.20 with an SD of 1.80 showing a significant improvement in the overall quality of life of all subjects.
On closer inspection there was a similar improvement in scores postoperatively in all domains of the questionnaire such as functional limitation, physical pain, psychological discomfort, physical disability, psychological disability, social disability and handicap. The most significant improvement was in the mean functional limitation domain, it being 3.25 with a SD of 1.07 preoperatively and only valuing at 0.95 with a SD of 0.22 6 months postoperatively. The domains of psychological discomfort and psychological disability similarly showed drastic improvements. The social disability scores also showed great improvements which is notable. The 2015 study by Conforte JJ, et. al. [25] corroborates this as they too found that facial trauma caused the greatest impact on the quality of life of surgical patients in the post-trauma, preoperative phase but that the surgical treatment of the same significantly improved quality of life for patients with mandibular and multiple facial fractures. Lewandowski B, et. al. [26] found in their study during the period of 8 months after lower facial injury, there was a significant improvement in the quality of life assessed with OHIP-14. Sahni V, et. al. [27] conducted a literature review which showed that patients suffering from orofacial trauma had significantly increased levels of mental state disorders such as post-traumatic stress disorder (PTSD) and generalized anxiety disorder, more so in victims of assault. Their results point toward an increased prevalence of mental state disorders in patients suffering from facial trauma, which warrants for early intervention in this regard to improve the quality of life of these patients. Several studies on patients with mandibular fractures noted that patients treated with MMF have better quality of life post treatment while higher pain scores were recorded in patients undergoing ORIF [28, 29]. This can be attributed to milder injuries which do not necessitate open reduction and internal fixation compared to panfacial trauma patients who obviously require more extensive treatment. This aspect of postoperative discomfort can be easily combatted by the surgical team being more mindful of patient’s pain score and by prescribing the appropriate analgesics to reduce the effect of pain being the causative factor that deteriorates the patients immediate postoperative quality of life [30]. Bearing all the evidence in mind, we can unequivocally state that management by ORIF of panfacial trauma patients if performed systematically and by a skilled operator can provide the sufferer with a good quality of life and that has been objectively proved in our study.
Conclusion
20 patients with panfacial fractures who underwent ORIF of their fractures were thoroughly analysed preoperatively and postoperatively to determine if they achieve masticatory functional efficiency of their stomatognathic system. This was done by measuring the patients preoperative MVBF and their postoperative MVBF’s at I week, 1 month, 3 months and 6 months post surgically and by comparing all these bite force readings with that of a healthy group of 20 volunteers. In addition we have tried to determine the postoperative quality of life of the patients by using the OHIP-14 Questionnaire as a tool wherein each trauma patient filled out the questionnaire by preoperatively and then 6 months postoperatively and the scores were then compared.
The following conclusions were drawn from our study:
- There was a significant steady improvement in masticatory efficiency postoperatively at 1 week, 1 month, 3 months and 6 months as compared to the preoperative phase.
- There was a significant improvement in masticatory efficiency 6 months postoperatively as compared to the immediate postoperative phase.
- A duration of 6 months was required for the patients to regain normal masticatory functional efficiency which was comparable to that of normal healthy volunteers.
- Intraoperative factors such as amount of periosteal bone stripping and number of muscle attachments released can have a negative impact on the patients’ masticatory efficiency in the long run.
- There was a significant improvement in the quality of life of the panfacial trauma patients 6 months postoperatively as compared to that preoperatively.
- It can be concluded that a duration of 6 months is required for the patients to return to normal life wherein they had complete regain of masticatory functional efficiency and also subjectively experienced a significant improvement in their quality of life.
References
-
Spagnol G, Palinkas M, Regalo SCH, de Vasconcelos PB, Sverzut CE, et al. (2016) Impact of midface and upper face fracture on bite force, mandibular mobility, and electromyographic activity. International Journal of Oral and Maxillofacial Surgery 45(11): 1424-1429.
-
Kshirsagar R, Jaggi N, Halli R (2011) Bite force measurement in mandibular parasymphyseal fractures: a preliminary clinical study. Craniomaxillofacial Trauma & Reconstruction 4(4): 241-244.
-
Peterson LJ (2012) Peterson’s Principles of oral and maxillofacial surgery. PMPH, USA.
-
Perry M, Holmes S (2014) Atlas of operative maxillofacial trauma surgery: primary repair of facial injuries. Springer.
-
Sybil D, Gopalkrishnan K (2013) Assessment of masticatory function using bite force measurements in patients treated for mandibular fractures. Craniomaxillofacial Trauma & Reconstruction 6(4): 247- 250.
-
Ribeiro MC, Regalo SCH, Pepato AO, Siéssere S, de Souza LG, et al. (2011) Bite force, electromyography, and mandible mobility during the 6-month period after surgical treatment for isolated fractures of the zygomatico-orbital complex. Oral Surgery, Oral Medicine, Oral Pathology Oral Radiology and Endodontology 111(4): e1-e7.
-
Kumar ST, Saraf S, Devi SP (2013) Evaluation of bite force after open reduction and internal fixation using microplates. Journal of Dentistry (Tehran, Iran) 10(5): 466.
-
Ellis E, Throckmorton GS (2001) Bite forces after open or closed treatment of mandibular condylar process fractures. Journal of Oral and Maxillofacial Surgery 59(4): 389-395.
-
Singh S, Fry RR, Joshi A, Sharma G, Singh S (2012) Fractures of angle of mandible–A retrospective study. Journal of Oral Biology and Craniofacial Research 2(3): 154-158.
-
Kumar S, Gattumeedhi SR, Sankhla B, Garg A, Ingle E, et al. (2014) Comparative evaluation of bite forces in patients after treatment of mandibular fractures with miniplate osteosynthesis and internal locking miniplate osteosynthesis. Journal of International Society of Preventive and Community Dentistry 4(S1): S26-S31.
-
Deshpande NC, Nawathe AA (2015) Translation and validation of Hindi version of oral health impact profile-14. Journal of Indian Society of Periodontology 19(2): 208-210.
-
Sathyanarayana HP, Premkumar S, Manjula WS (2012) Assessment of maximum voluntary bite force in adults with normal occlusion and different types of malocclusions. J Contemp Dent Pract 13(4): 534-538.
-
Shushma G, Kantly R (2016) Gnathodynamometer--a reliable device for assessing jaw bite force. Journal of Evolution of Medical and Dental Sciences 5(102): 7488- 7491.
-
Raustia AM, Oikarinen KS, Pernu H (1997) Changes in electrical activity of masseter and temporal muscles after temporomandibular joint surgery: A one-year follow up. International Journal of Oral and Maxillofacial Surgery 26(4): 253-257.
-
Varga S, Spalj S, Lapter Varga M, Anic Milosevic S, Mestrovic S, et al. (2011) Maximum voluntary molar bite force in subjects with normal occlusion. The European Journal of Orthodontics 33(4): 427-433.
-
Badwal RS, Bennett J (2003) Nutritional considerations in the surgical patient. Dental Clinics 47(2): 373-393.
-
Mercurio AD, Motta T, Green E, Noble G, Hart RT, et al. (2012) Effects of extensive circumferential periosteal stripping on the microstructure and mechanical properties of the murine femoral cortex. Journal of Orthopaedic Research 30(4): 561-568.
-
Throckmorton GS, Talwar RM, Ellis E (1999) Changes in masticatory patterns after bilateral fracture of the mandibular condylar process. Journal of Oral and Maxillofacial Surgery 57(5): 500-508.
-
van den Braber W, van der Glas H, van der Bilt A, Bosman F (2004) Masticatory function in retrognathic patients, before and after mandibular advancement surgery. Journal of Oral and Maxillofacial Surgery 62(5): 549-554.
-
Galil KA, Loukota R (2010) Fractures of the mandibular condyle: evidence base and current concepts of management. British Journal of Oral and Maxillofacial Surgery 48(7): 520-526.
-
McCarty JC, Herrera Escobar JP, Gadkaree SK, El Moheb M, Kaafarani HM, et al. (2021) Long-term functional outcomes of trauma patients with facial injuries. Journal of Craniofacial Surgery 32(8): 2584-2587.
-
Felce D, Perry J (1995) Quality of life: Its definition and measurement. Research in Developmental Disabilities 16(1): 51-74.
-
Tan PG, Soh CL (2020) Quality of life assessments in maxillofacial trauma patients-A systematic review. Journal of Oral and Maxillofacial Surgery Medicine and Pathology 32(2): 87-92.
-
Campos LA, Peltomäki T, Marôco J, Campos JADB (2021) Use of oral health impact profile-14 (OHIP-14) in different contexts. What is being measured?. International Journal of Environmental Research and Public Health 18(24): 13412.
-
Conforte JJ, Alves CP, Ponzoni D (2016) Impact of trauma and surgical treatment on the quality of life of patients with facial fractures. International journal of Oral and Maxillofacial Surgery 45(5): 575-581.
-
Lewandowski B, Szeliga E, Lewandowska EC, Ozga D, Kontek A, et al. (2018) Comparison of oral-health- related quality of life in patients in the short-and long- term period following lower-facial injury and fractures- preliminary report. Dental and Medical Problems 55(1): 57-62.
-
Sahni V (2018) Psychological impact of facial trauma. Craniomaxillofacial Trauma & Reconstruction 11(1): 015-020.
-
Omeje KU, Adebola AR, Efunkoya AA, Osunde OD, Bamgbose BO, et al. (2015) Prospective study of the quality of life after treatment of mandibular fractures. British Journal of Oral and Maxillofacial Surgery 53(4): 342-346.
-
Omeje KU, Rana M, Adebola AR, Efunkoya AA, Olasoji HO, et al. (2014) Quality of life in treatment of mandibular fractures using closed reduction and maxillomandibular fixation in comparison with open reduction and internal fixation-A randomized prospective study. Journal of Cranio-Maxillofacial Surgery 42(8): 1821-1826.
-
Sharma G, Kaur A (2017) Quality of life after orbito-facial trauma. Orbit 36(6): 407-410.
- Management of Chronic Insertional Achilles Tendinopathy Using Flexor Hallucis Longus Tendon Transfer in Patients Over 50 Years of Age: A Four-Case Series Following the CARE Guidelines
- Application of Induced Pluripotent Stem Cells in Bone Tissue Engineering: Current Status and Prospects
- Surgical Management of Upper Thoracic Esophageal Squamous Cell Carcinoma with Concomitant Hypersplenism: Integration of Chai's Supra-Thoracic Apex Technique with Laparoscopic Splenectomy - A Technical Innovation Case Study with Systematic Review
- Hepatic Abscess Secondary to Appendiceal Phlegmon an Unusual Complication of Appendiceal Phlegmon
- Report of Lumboperitoneal (LP) Shunt Procedure in Over Decades Experiences, Systematic Narrative Review
- Encasement of Ventral Hernia Mesh within Small Bowel: A Case Report