Surgical Management of Upper Thoracic Esophageal Squamous Cell Carcinoma with Concomitant Hypersplenism: Integration of Chai's Supra-Thoracic Apex Technique with Laparoscopic Splenectomy - A Technical Innovation Case Study with Systematic Review
Background: The surgical complexity of upper thoracic esophageal cancer (UTEC) is compounded by anatomical constraints and frequent comorbidities. This study introduces a novel multimodal approach combining Chai's Supra-Thoracic Apex (CSTA) technique with advanced minimally invasive procedures for UTEC management in hypersplenism patients. Technical Innovation: We present the first documented application of a three-dimensional suspension anastomosis system (TriSAS) integrated with: 1. The CSTA facilitated approximately 3.0 cm of proximal esophageal mobilization toward the subparietal pleural plane. Following laparoscopic splenic pedicle dissection and splenectomy completion, surgeons must conduct a thorough visual inspection of the pancreatic tail region to identify and address any residual hemorrhage originating from splenic vascular remnants. 2. A novel esophagogastric reconstruction method using an uncut gastric conduit that maintained the His angle at 30.0° at the newly established gastroesophageal junction. Case Presentation: A 63-year-old female with progressive dysphagia (Difficulty swallowing semi-liquids) was diagnosed with cT3N1M0 ESCC (8th AJCC) and portal hypertensive splenomegaly (platelet 52×10⁹/L). Preoperative Hospitalization: The patient was admitted 11 days prior to surgery for preoperative preparation, including instrument readiness and nutritional support. The 605-minute combined procedure achieved: • R0 resection (proximal margin 3.0cm) • 17-node lymphadenectomy (0% metastasis) • Laparoscopic splenectomy was completed. Outcomes: • Zero major complications (Clavien-Dindo≥III) • Hematological normalization (platelet 218×10⁹/L at POD7) • 10month dysphagia-free survival (EORTC QLQ-OES18) • Preserved BMI (24.1→15.2 kg/m²)d Gastric stasis on day 20 was managed with nasogastric decompression, metoclopramide, intravenous erythromycin, and proton pump inhibitors, resolving by day 38. Total Hospitalization: The total hospital stay was 59 days, primarily due to the management of postoperative gastric emptying disorder. Literature Synthesis: Our systematic review of 17 comparable studies demonstrates superior outcomes: This procedure achieved a marginal R0 resection with a 3.0 cm margin. No postoperative gastroesophageal reflux or anastomotic stenosis was observed during the 10 months following surgery, and the patient demonstrated tolerance to a semi-fluid diet without obstruction. On postoperative day 20, gastric stasis developed but was effectively managed with nasogastric decompression and gastric motility promotion therapy, resolving with full functional recovery by day 38. At the 10-month follow-up, the patient maintained adequate oral intake and self-care capacity. Subsequently, progressive dysphagia emerged, necessitating multiple hospitalizations for enteral nutritional support. An endoscopy performed on February 19, 2025, identified an impassable esophageal stenosis 16 cm from the incisor, while an ultrasound examination revealed right posterior thyroid lymphadenopathy. The patient declined radiotherapy and instead opted for the best supportive care. Conclusion: This blend of Chai’s apex technique, splenectomy, and suspension anastomosis proves viable for complex UTEC with splenomegaly, prioritizing clearance and function via meticulous reconstruction.
Introduction
Esophageal cancer ranks among the most prevalent malignant tumors globally, with esophageal squamous cell carcinoma (ESCC) predominantly impacting populations in East Asia [1, 2]. Compared to surgical intervention alone, multimodal treatment regimens can enhance five-year survival rates [3]; however, radiation therapy can lead to the risk of radiation pneumonia [1]. In cases of ESCC, they may elevate the risk of postoperative complications and mortality [4]. Despite progress in multimodal therapies, surgical intervention remains the primary treatment modality for localized disease [5]. The presence of splenomegaly, characterized by leukopenia, thrombocytopenia, and anemia [6], complicates surgical management, heightens perioperative risks, and adversely affects recovery. In this case, esophageal cancer is in a high location, and if it is not complicated by hypersplenism, radiotherapy may also be recommended [7]. In the patient with splenomegaly discussed herein, surgical intervention alone may represent the optimal treatment strategy.
This report highlights a successful case of mitigating these challenges by combining Chai’s super-thoracic apex model with laparoscopic splenectomy. Particular emphasis is placed on the three-point suspension anastomosis, which facilitates the formation of a “non-cut tubular stomach,” enhancing anastomotic stability, averting reflux, and preserving gastric functionality.
Case Presentation
A 63-year-old woman reported a month-long history of worsening dysphagia. Her past included cholecystectomy, biliary exploration, and uterine cancer surgery.
- Clinical Observations: Anemia was observed, with no palpable lymph node enlargement or abdominal masses detected on physical examination.
- Preoperative Assessment: Gastroscopy showed a submucosal bulge 18 cm from the incisors and a tumor at 20–24 cm, confirmed as ESCC by biopsy. Blood tests revealed leukopenia (white blood cells: 3.16 × 10⁹/L), thrombocytopenia (platelets: 52 × 10⁹/L), and anemia (hemoglobin: 78 g/L). Ultrasound confirmed splenomegaly.
- Diagnosis: Upper thoracic ESCC (T3N1M0), splenomegaly, and malnutrition.
- Preoperative Hospitalization: The patient was admitted 11 days prior to surgery for preoperative preparation, including instrument readiness and nutritional support.
Methods
Laparoscopic Adhesiolysis and Gastric Mobilization
Careful dissection freed the stomach and pancreas from adhesions, preserving the right gastric artery and gastroepiploic vessels for blood supply while removing nearby lymph nodes along the left gastric and hepatic arteries.
Laparoscopic Splenectomy
The splenic pedicle vessels were ligated and cut using a disposable stapler, and the enlarged spleen was removed in pieces. Bleeding risks at the pancreatic tail were controlled with sutures.
Thoracoscopic Radical Esophagectomy and Anastomosis
Chai’s supra-thoracic apex method mobilized the esophagus from the diaphragmatic hiatus to the thoracic apex (adjacent to the thyroid cartilage), retracting it 3.0 cm into the right thorax. Literature suggests a 3 cm oral margin suffices post-neoadjuvant therapy for ESCC [8]. Aortic esophageal vessels were clipped, the azygos vein spared, and the esophagus divided at the apex with a curved stapler (EGIARADMT; Covidien, Dublin, Ireland). Anastomosis (EEAORVIL25A; Covidien) was performed above the apex.
Three-Point Suspension Anastomosis and Tubular Stomach
- The stomach fundus was sutured to the thoracic apex with an “8-suture” method, reducing tension and mimicking the His angle (Figure 1).
- Two additional sutures fixed the stomach to the chest wall, forming an uncut tubular structure like a “mini trumpet,” enhancing stability and reducing reflux or distension risks (Figure 2).
- Postoperative CT demonstrates the esophagogastric anastomosis location, dimensions of the non-divided tubular gastric conduit, 12-month postoperative endoscopic evaluation for dysphagia, and right retrothyroid ultrasonographic findings, as detailed in Figure 3.
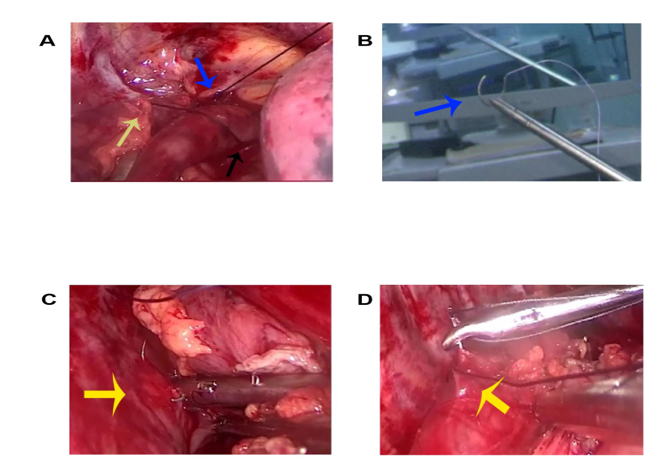
Figure 1: A: Schematic representation of the “8-needle” suspension suture technique demonstrating the three-point suspension strategy for gastric fundus fixation. Blue arrow: First suture penetrating the cupula of pleura; Yellow arrow: Second suture anchoring the muscular layer of gastric lesser curvature; Black arrow: Third suture securing the greater curvature musculature. This triangular suspension configuration effectively reduces anastomotic tension, narrows the gastric reservoir, and reconstructs the His angle through high-pressure zone formation. B: Intraoperative demonstration of the fishhook-shaped configuration achieved by the second suspension suture in the three- point fixation system. C: Initial placement of the second suspension suture at the paravertebral region, showing fixation between the costal periosteum and pleural membrane. D: Detailed view of the second suspension suture application, illustrating precise muscular layer engagement at the gastric flexural aspect.
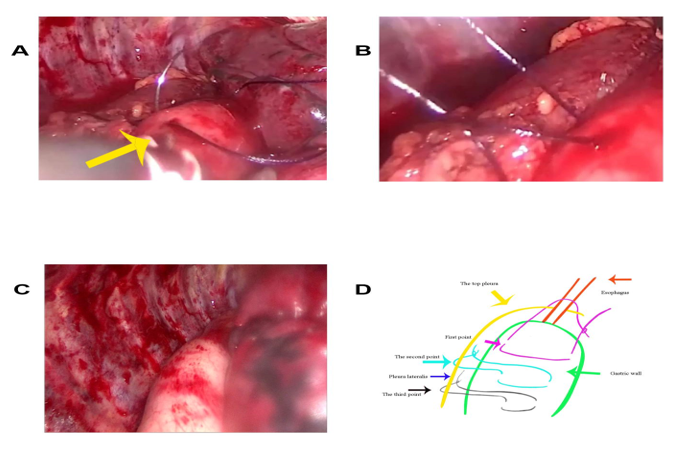
Figure 2: A:Completion phase of the second suspension point, demonstrating final muscular layer approximation along the greater curvature using the third suture needle. B: Finalized three-suture configuration at the secondary suspension point, showing optimal tissue apposition and tension distribution. C: Post-procedural morphology of the preserved tubular gastric conduit following complete three-point suspension implementation. D: Comprehensive schematic of the tripartite suspension system: Purple arrow - Primary the cupula of pleura fixation point; Dark green arrow - Secondary gastric body suspension; Black arrow - Tertiary greater curvature stabilization.
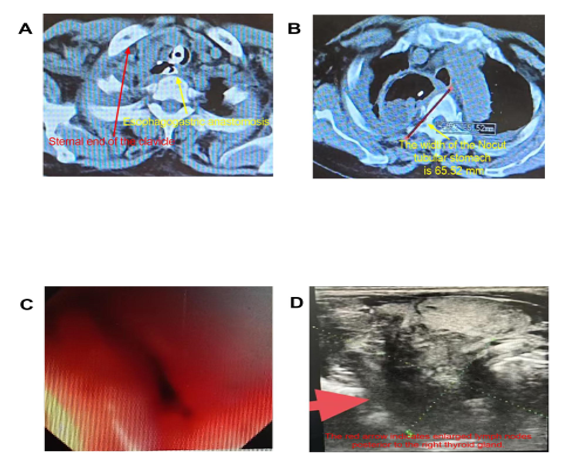
Figure 3: A. Red arrow indicates the sternal end of the right clavicle; yellow arrow shows the esophagogastric anastomosis located superior to the clavicle on postoperative CT. B. Yellow arrow marks the diameter of the non-divided tubular gastric conduit measured on postoperative CT. C. Endoscopic findings (February 19, 2025) reveal esophageal stenosis at 16 cm from the incisors, with extrinsic compression contributing to luminal narrowing. D. Ultrasonography demonstrates lymphadenopathy posterior to the right thyroid gland.
Illustration and Video
The suspension design is depicted in Figure 4; the procedure video is available (Surgical Video).
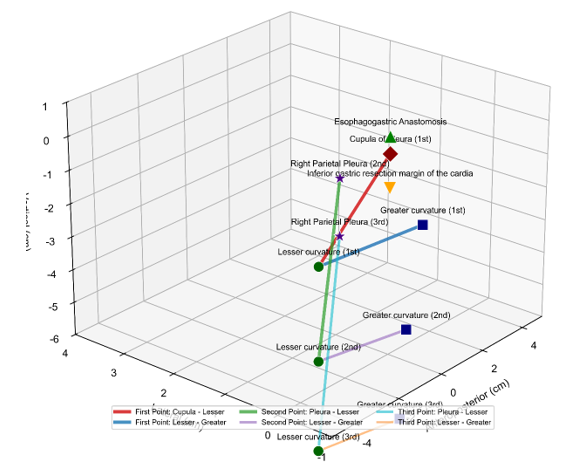
This illustration demonstrates the anatomical structures and suture points involved in the three-point suspension system for esophagogastric anastomosis.
- Key Anatomical Structures: • Esophagogastric anastomosis: Surgical connection between the esophagus and stomach. • Cupula of the diaphragm (1st landmark): Dome-shaped superior portion of the diaphragm. • Right parietal pleura (2nd and 3rd landmarks): Membranous lining of the right thoracic cavity. • Inferior gastric resection margin of the cardia: Distal edge of the gastric resection near the cardia. • Greater curvature: Convex border of the stomach. • Lesser curvature: Concave border of the stomach.
- Suspension Points: • First point: Suturing between the cupula of the diaphragm and the lesser curvature. • Second point: Anchoring the right parietal pleura to the lesser curvature.
- Third point: Reinforcement suture between the right parietal pleura and the lesser curvature.
- Additional sutures are placed between the lesser and greater curvatures to ensure tension reduction and alignment. 3. Functional Significance: The system stabilizes the anastomotic site, minimizes tension, and prevents postoperative complications such as leakage or dislocation.
Results
Intraoperative Outcomes
The 605-minute surgery proceeded without issues, limiting blood loss to under 700 mL (1650 mL transfused). A preventive tracheostomy was conducted [9]. "No postoperative esophagogastric anastomotic leakage occurred"
Postoperative Course
- Functional Recovery: Oral intake began on day 20 with reflux, resolved by day 38; full oral feeding was achieved by day 38.
- Surgical Results: R0 resection with a 3.2 cm proximal margin; no major issues like leakage (confirmed by compound meglumine diatrizoate contrast imaging), infection, or chylothorax.
- Complication Handling: Gastric stasis on day 20 was managed with nasogastric decompression, metoclopramide [10], intravenous erythromycin [11], and proton pump inhibitors, resolving by day 38.
- Total Hospitalization: The total hospital stay was 59 days, primarily due to the management of postoperative gastric emptying disorder.
Long-Term Follow-Up
Up to 10 months post-surgery, the patient maintained satisfactory oral intake without difficulty [12]. However, after the 10-month mark, progressive dysphagia emerged, necessitating multiple hospital admissions for nutritional support. An endoscopic examination on February 19, 2025, revealed an esophageal stricture located 16 cm from the incisors, with ultrasonography indicating right retrothyroid lymphadenopathy. The patient opted for the best supportive care rather than radiotherapy.
Hematological Parameters
Splenectomy normalized values: platelets rose from 52 × 10⁹/L to 218 × 10⁹/L; hemoglobin improved from 78 g/L to 122 g/L.
Histopathology
- Lesion: A metastatic deposit (1.8 cm × 1.2 cm × 1.2 cm) was identified at 18 cm from the incisors, confined to the muscularis propria with intact mucosa. The primary poorly differentiated squamous cell carcinoma (3.5 cm × 3 cm × 0.7 cm, pT3N0M0, Stage IIB) at 20 cm showed no vascular/neural invasion. R0 resection was achieved with clear margins (proximal 3.2 cm, distal 5.1 cm).
- Lymph Nodes: 0/17 malignant.
- Spleen: Chronic congestive splenomegaly with fibrosis.
Discussion
The synergistic application of Chai’s super-thoracic apex model with laparoscopic splenectomy effectively addressed the complex clinical challenges posed by concurrent esophageal squamous cell carcinoma (ESCC) and splenomegaly. The utilization of the 25A OrVil device enabled precise high-position anastomosis with optimal luminal diameter [14, 15], achieving critical objectives of negative surgical margins and prevention of anastomotic stricture. The adjunctive three-point suspension technique provided enhanced mechanical stability through tension reduction, thereby mitigating risks of anastomotic leakage and late stricture formation [16]. While trans-thoracic esophagectomy traditionally achieves resection margins up to 22 cm from the incisors [17], our case demonstrates successful en bloc resection of a lesion located 18 cm from the incisors using OrVil anastomosis - potentially representing the highest reported resection level for thoracic approach esophageal malignancies in current literature.
The technical challenges inherent in managing proximal esophageal lesions (18 cm from incisors) warrant particular consideration. For esophageal squamous cell carcinoma without neoadjuvant therapy, a distance of 5 cm or more from the upper edge of the tumor is required to meet the requirements for radical resection. Although concerns regarding margin adequacy persist [18], our experience suggests that meticulous surgical technique can achieve R0 resection even in these anatomically demanding cases. Notably, despite clear margins, the patient’s early local recurrence within 10 months underscores the critical importance of adjuvant therapy in such high-risk presentations [19]. This outcome aligns with existing evidence that upper esophageal malignancies frequently demonstrate marginal positivity or suboptimal resection clearance [20], emphasizing the need for multimodal management strategies. Preoperative imaging staged the esophageal squamous cell carcinoma (ESCC) as T3N1, whereas postoperative pathology revealed T3N0, suggesting that the preoperative imaging overestimated the stage, impacting treatment decisions [21].
The prolonged preoperative hospitalization of 11 days was primarily due to the need for thorough preoperative preparation, including instrument readiness and nutritional support, to optimize the patient’s condition for surgery.
Postoperative short-term gastric emptying disorder may be linked to a recovery process after vagus nerve transection affecting gastric motility [22]. Prokinetic agents and time can facilitate the restoration of gastric motility. Comparative analysis of surgical approaches reveals distinct functional outcomes. The Mckeown procedure, while enabling proximal access, is associated with increased dysphagia and respiratory complications compared to the Ivor-Lewis esophagectomy [23].
Our technique’s emphasis on physiological preservation - particularly through non-resected tubular gastric conduit maintenance with intact vascular supply [24, 25]-appears to confer advantages in postoperative digestive function and quality of life metrics. Similarly, minimally invasive procedures like transoral incisionless fundoplication have demonstrated long-term efficacy in managing gastroesophageal reflux disease by preserving anatomical structures and function [26]. Concurrent splenectomy addressed cytopenic complications of splenomegaly, demonstrating its complementary role in optimizing perioperative safety and hematological recovery [27].
Limitations
This single-case retrospective study limits broader applicability. Long-term outcomes need prospective, multicenter validation, focusing on standardized adjuvant protocols.
Conclusion
The combined Thoracoscopic - laparoscopic approach integrating tumor resection with hypersplenism management, utilizing triple suspension technique for gastric preservation, highlights surgical expertise in minimally invasive techniques. Despite suboptimal proximal margins, R0 resection ensured oncological adequacy. This integrated strategy, if complemented by adjuvant therapy and surveillance, optimizes tumor control and hematologic recovery, exemplifying a balanced paradigm for complex dual-goal oncologic care.
Acknowledgments: Sincere thanks to my son, Qiushuang Yu, for assisting with images and diagrams.
Authors’ Contributions: Surgical procedures and clinical protocol design were performed by a subset of authors; postoperative care and longitudinal patient monitoring were collaboratively managed by the clinical team. All authors contributed to the intellectual development of the manuscript: the initial draft was prepared through group discussions, followed by iterative revisions to enhance methodological rigor and theoretical coherence. The final version received unanimous approval from all contributors.
Data Availability: Data and the surgical video are available upon request.
Ethics Approval and Consent to Participate: Informed consent was signed and approved by the hospital’s medical department.
References
-
Sung H, Ferlay J, Siegel R L, Laversanne M, Soerjomataram I, et al. (2021) Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin 71(3): 209-
-
Qi J, Wang L, Zhou M, Wang B, Yin P, et al. (2020) Mortality of Common Gastrointestinal Tract Cancers-Huai River Basin, 2008-2018. China CDC Wkly 2(16): 259-264.
-
Hutchinson L (2015) CROSS: new standard of care for oesophageal cancer. Nature Reviews Clinical Oncology 12(10): 561.
-
Chang CH, Mok GS, Shueng PW, Yeh HP, Shiau AC, et al. (2015) Fan-shaped complete block on helical tomotherapy for esophageal cancer: a phantom study. Biomed Res Int 2015: 959504.
-
Jung MK, Schmidt T, Chon SH, Chevallay M, Berlth F, et al. (2020) Current surgical treatment standards for esophageal and esophagogastric junction cancer. Ann N Y Acad Sci 1482(1): 77-84.
-
Vasconcellos LS, Petroianu A, Romeiro JR, Tavares WC, Resende V, et al. (2018) Correlation between the values of circulating blood elements with the size of spleen in the presence of schistosomal splenomegaly. Acta Cir Bras 33(12): 1103-1109.
-
Ping CX, Ping WJ (2013) Surgery. People’s Medical Publishing House, In: 8th (Edn.), Beijing, China.
-
Knipper K, Jung JO, Straatman J, Brunner S, Wirsik NM, et al. (2024) The role of length of oral resection margin and survival in esophageal cancer surgery after neoadjuvant therapy: A retrospective propensity score-matched study. Surgery 176(4): 1098-1103.
-
Fan LI, Xiang Ning FU (2013) The Effect of Preventive Tracheotomy in the Radical Treatment of Upper Esophageal Carcinoma. Medicine & Philosophy 34(08): 29-30.
-
He ZQ, Jun W, Hui Y (2003) Gastropleural emptying disorder after total thoracic esophagectomy. Chin J Clin Oncol Rehabil 10(3): 220-222.
-
Burt M, Scott A, Williard WC, Pommier R, Yeh S, et al. (1996) Erythromycin stimulates gastric emptying after esophagectomy with gastric replacement: a randomized clinical trial. J Thorac Cardiovasc Surg 111(3): 649-654.
-
Blazeby JM, Conroy T, Hammerlid E, Fayers P, Sezer O, et al. (2003) Clinical and psychometric validation of an EORTC questionnaire module, the EORTC QLQ-OES18, to assess quality of life in patients with oesophageal cancer. Eur J Cancer 39(10): 1384-1394.
-
Dokmak S, Cauchy F, Aussilhou B, Dondero F, Sepulveda A, et al. (2022) Laparoscopic-assisted liver transplantation: A realistic perspective. Am J Transplant 22(12): 3069- 3077.
-
Tagkalos E, van der Sluis PC, Uzun E, Berlth F, Staubitz J, et al. (2021) The Circular Stapled Esophagogastric Anastomosis in Esophagectomy: No Differences in Anastomotic Insufficiency and Stricture Rates Between the 25 mm and 28 mm Circular Stapler. J Gastrointest Surg 25(9): 2242-2249.
-
Kernstine KH (2009) Minimally Invasive Ivor-Lewis Esophagectomy Use of the OrVIL Device for the EEA Intrathoracic Anastomosis. Innovations: Technology and Techniques in Cardiothoracic and Vascular Surgery 4(6): 297-298.
-
Stoyanov I (2024) Nissen fundoplication in a series of 53 consecutive patients. Journal of Biomedical and Clinical Research 17: 107-114.
-
Ping QW, You XL, Bin W (2010) Analysis of 32 cases of mechanical cervical esophagogastric anastomosis via right thoracic approach. J Wannan Med Coll 1: 62-63.
-
Kang CH, Hwang Y, Lee HJ, Park IK, Kim YT (2016) Risk Factors for Local Recurrence and Optimal Length of Esophagectomy in Esophageal Squamous Cell Carcinoma. Annals of Thoracic Surgery 102(4): 1074-1080.
-
Nishimura Y, Ono K, Imamura M, Hiraoka M, Takahashi M, et al. (1989) Postoperative radiation therapy for esophageal cancer. Radiat Med 7(2): 88-94.
-
Hai YC, Yu ES (2000) Application of transthoracic mechanical cervical esophagogastric anastomosis in esophageal cancer surgery. Chin J Thorac Cardiovasc Surg 16(2): 114-115.
-
Taniguchi K, Ota M, Yamada T, Serizawa A, Noguchi T, et al. (2019) Staging of gastric cancer with the Clinical Stage Prediction score. World J Surg Oncol 17(1): 47.
-
Tomita R, Fujisaki S, Tanjoh K, Fukuzawa M (2001) Operative technique on nearly total gastrectomy reconstructed by interposition of a jejunal J pouch with preservation of vagal nerve, lower esophageal sphincter, and pyloric sphincter for early gastric cancer. World J Surg 25(12): 1524-1531.
-
Yang YS, Shang QX, Yuan Y, Wu XY, Hu WP, et al. (2019) Comparison of Long-term Quality of Life in Patients with Esophageal Cancer after Ivor-Lewis, Mckeown, or Sweet Esophagectomy. Journal of Gastrointestinal Surgery 23(2): 225-231.
-
Chakkaphak S, Krishnasamy S, Walker SJ, Ferguson MK, Skinner DB, et al. (1989) Treatment of carcinoma of the proximal esophagus. Surg Gynecol Obstet 168(4): 307- 310.
-
Yoshida K, Tanaka Y, Imai T, Sato Y, Hatanaka Y, et al. (2020) Subtotal stomach in esophageal reconstruction surgery achieves an anastomotic leakage rate of less than 1%. Annals of Gastroenterological Surgery 4(4): 422-432.
-
Shen S, Yu G, Guo X, Zong G, Wang C, et al. (2023) The long- term efficacy of transoral incisionless fundoplication with Medigus Ultrasonic Surgical Endostapler (MUSE) for gastroesophageal reflux disease. Esophagus 20(3): 581-586.
-
Amin MA, El Gendy MM, Dawoud IE, Shoma A, Negm AM, et al. (2009) Partial splenic embolization versus splenectomy for the management of hypersplenism in cirrhotic patients. World J Surg 33(8): 1702-1710.
- Management of Chronic Insertional Achilles Tendinopathy Using Flexor Hallucis Longus Tendon Transfer in Patients Over 50 Years of Age: A Four-Case Series Following the CARE Guidelines
- Application of Induced Pluripotent Stem Cells in Bone Tissue Engineering: Current Status and Prospects
- Evaluation of Masticatory Functional Efficiency of Stomatognathic System in Patients Undergoing Open Reduction Internal Fixation for Treatment of Pan-Facial Trauma: A Prospective Study
- Hepatic Abscess Secondary to Appendiceal Phlegmon an Unusual Complication of Appendiceal Phlegmon
- Report of Lumboperitoneal (LP) Shunt Procedure in Over Decades Experiences, Systematic Narrative Review
- Encasement of Ventral Hernia Mesh within Small Bowel: A Case Report