Remission of Post Liver Transplant FSGS after Conversion to Ciclosporin-A from FK506 -- 3 Case Reports
<p>Background: FK506 (FK) is the key immunosuppressive drug for orthotropic de novo liver transplantation recipients. It has been shown to be superior to Ciclosporin-A (CsA) in terms of graft survival and toxicity. However, we report of three cases, who developed FSGS in the native kidneys that remitted when FK506 was switched to CsA. Methods: We changed FK506 to CsA in 2 patients keeping the third patient continue FK as before. At timed interval we evaluated renal remission and liver graft status over a long period of 6 years. Both short-term and long-term outcomes in terms of renal and liver were compared. Achievement of 50% reduction of proteinuria (TUP) was the endpoint. Results: Patient characteristics were similar except for the incidence of HCV in the non-converted case. Stable remission of proteinuria and stable renal function were attained in the converted cases, while the 3rd case had increase in proteinuria from 1.44 g/d to 2.25 g/d with deterioration of RFT. There was no episode of AR in the OLTX post conversion as proven by biopsy. Conclusions: CsA may induce remission in FSGS precipitated by FK506 for OLTX without compromising liver graft.</p>
Introduction
Fk506 monotherapy or in combination with steroid in orthotropic Liver transplantation (OLTX) is the standard practice. It has proven superior to Ciclosporin-A (CsA) in preventing Acute Rejection (AR) and in prolonging patient and graft survival [1, 2, 3]. In addition, incidence of side effects like hirsutism, hypertension and hyperlipidemia are less common in FK506 [4, 5, 6]. Although FK is more diabetogenic in long-term use because of pancreatic islet cell dysfunction, this can be well controlled by conventional hypoglycemic agents [4]. However, as a calcineurin inhibitor (CNI), it has enjoyed a relative safety profile over CsA. Recently, Evorilimus (EVR) has been in use for OLTX with good results in a pursuit of avoiding FK [7]. Various studies have addressed the impact of OLTX and the associated CNI immunosuppression on renal function and chronic kidney disease [8, 9, 10]. In addition, impacts of different CNI on renal status post renal transplantation have been discussed in abundance [11, 12, 13, 14, 15, 16]. However, there is paucity of reports of recurrent FSGS in native kidney after OLTX due to CNI, and in renal allograft post- transplant, after conversion to FK506 from CsA. This lack of evidence in transplant literature makes it difficult to validate the cause and effect relationship between FK and FSGS in native kidney after OLTX, and in renal allograft because of issues of recurrent diseases in the grafted kidney. Nevertheless, the objective facts presented in this case report cannot be ignored. Moreover HCV, which is a frequent cause of Chronic Liver Disease (CLD), also causes FSGS [17, 18]. For these reasons it is difficult to conclude the causal relationship between de-novo FSGS in native kidney because of FK use in OLTX. It would be of paramount interest to observe the impact on de-novo renal pathology of immuno-conversion of FK to CsA in OLTX.
Case Report
We diagnosed FSGS by renal biopsy in 3 cases of OLTX when they developed de-novo proteinuria 6 to 10 years after liver transplant. Initially, we became aware of significant proteinuria (TUP>1 gm/day) in one case of OLTX. That led us to monitor TUP routinely in other liver transplant cases. The liver transplant surgery and time to develop proteinuria with subsequent performance of renal biopsy to get the diagnosis of FSGS were at different occasions in these three cases. All of these 3 cases were on FK506 after OLTX. We did not use Mycophenolate Mofetil (MMF) in our liver transplant cases including the three case of this series. The other immunosuppressive medicine was prednisolone. It’s dosage pattern followed the standard protocol for liver transplant. In view of the observation of biopsy proven FSGS in these 3 cases of OLTX who were on FK, we decided to evaluate the effect of conversion to CsA in 2 cases keeping the 3rd case as control with continuation of FK.
Patients’ demographics are given in table 1. The background parameters of the cases at the time of conversion to CsA, were recorded and are shown in table 2.We mentioned the Serum creatinine level at the time of renal biopsy that showed FSGS. We followed up all cases with measurement of RFT and TUP until the achievement of endpoint of having partial remission of FSGS, as defined by us as 50% reduction of proteinuria. This endpoint was achieved in two cases. The earliest case (the 3rd case) did not undergo remission as even at 1 year and renal function continues to deteriorate subsequently.
| Y | Age | s | HB | s | Time to FSGS | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| P | atient | s | HCVAb | Drug | |||||||||||||
| ear | Ag | (Months) | |||||||||||||||
| Case 1 | 47 | + | - | 124 | CsA 163 ng/ml | ||||||||||||
| Case 2 | 42 | + | + | 82 | CsA 133 ng/ml | ||||||||||||
| Control Case | 64 | - | + | 72 | FK506 7.4 ng/ml |
Table 1: Patients’ demographics.
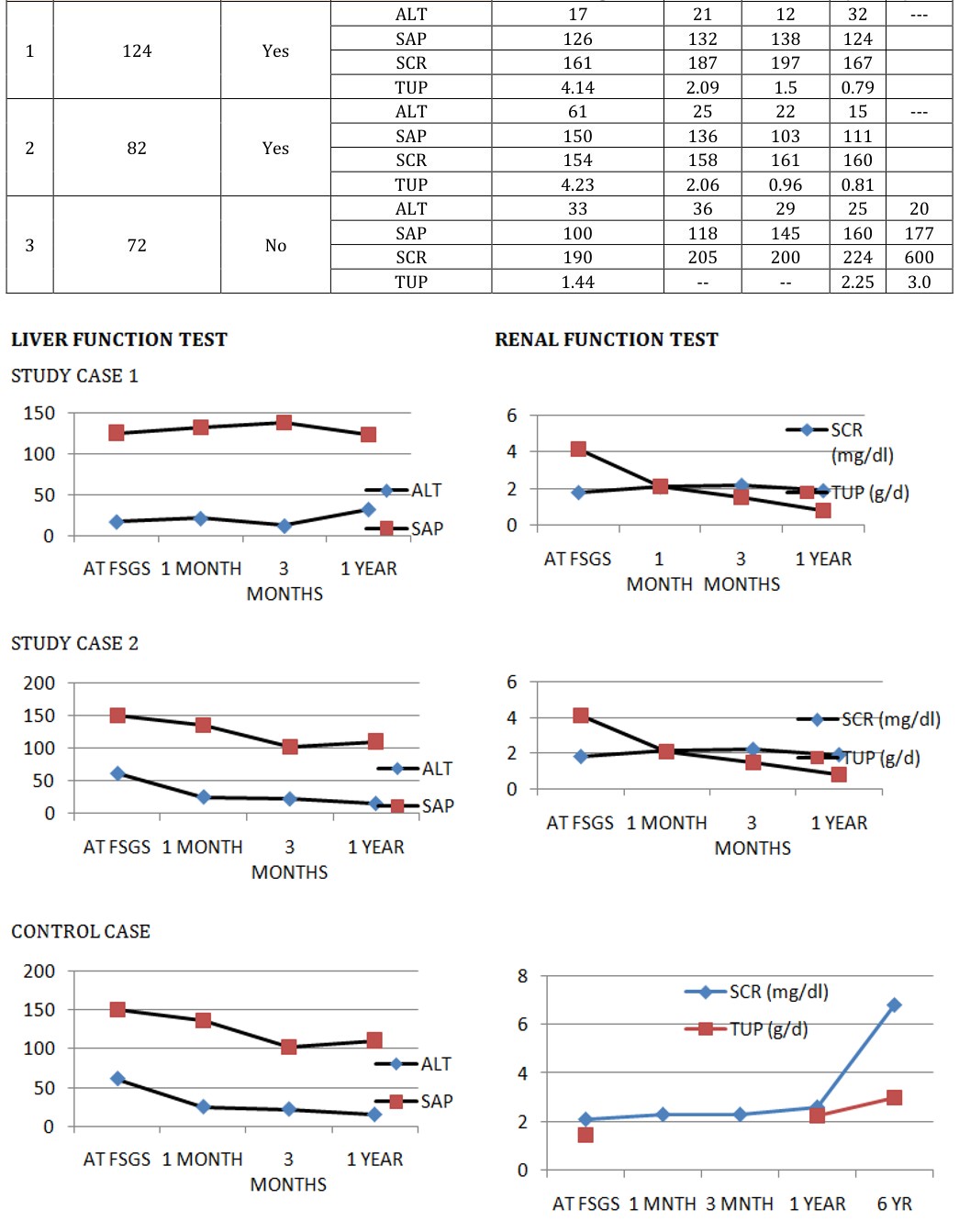
Table 1: Patients’ demographics. FK- FK506, CsA- Ciclosporin–A, FSGS- Focal and segmental glomerulosclerosis, HBsAg- hepatitis B surface antigen, HCVAb- hepatitis C antibody. Liver function test (LFT) and renal function tests (RFT) included serum alanine aminotransferase (ALT), serum alkaline phosphatase (AP), serum creatinine (SCR) and 24 hours urinary protein (TUP) in addition to other routine tests. These tests were done at the time of drug switch (M0) and repeated at 1 month (M1), 3 months (M3) and 12 months (M12) intervals. Liver biopsy in the transplanted liver was done at the time of drug switch to diagnose graft status and was planned to repeat at times of abnormal liver function to diagnose acute rejection in the liver graft. In the 2 cases (1st and 2nd case) where FK506 was stopped and CsA was started at a dose of 3-5 mg/kg in 2 divided doses, the trough levels were maintained at about150 ng/ml. In the control case (3rd case) where FK was continued, renal biopsy was repeated 5 years after the 1st biopsy. Rejection episode in liver graft post conversion to CsA was monitored by LFT and Liver biopsy. Remission of FSGS was defined as a more than 50% reduction of TUP with stable RFT. All 3 cases were on oral Enalapril tablet. Prednisolone was the second immunosuppressive medicine in all 3 cases of OLTX.
Course of Subsequent Liver and Renal Status
The 3 patients were all male (age: 47, 42 and 64 years) with HBV positive in 1st and 2nd, and HCV positive in 2nd
as proven by biopsy. The 2nd case developed recurrent HCV disease. Renal biopsy was repeated in the 2 cases that showed 50% reduction of TUP. The case where proteinuria increases and progressed to ESRF was not subjected repeat renal biopsy. The renal biopsy showed stability of glomerular sclerosis without further progression.
| Time (M) to FSGS | Start of CsA | Laboratory tests | Intervals after conversion to CsA from FK | |||||
|---|---|---|---|---|---|---|---|---|
| At FSGS diagnosis | 1 month | 3 months | 1 year | 6 years | ||||
| 1 | 124 | Yes | ALT | 17 | 21 | 12 | 32 | --- |
| 1 | 124 | Yes | SAP | 126 | 132 | 138 | 124 | |
| 1 | 124 | Yes | SCR | 161 | 187 | 197 | 167 | |
| 1 | 124 | Yes | TUP | 4.14 | 2.09 | 1.5 | 0.79 | |
| 2 | 82 | Yes | ALT | 61 | 25 | 22 | 15 | --- |
| 2 | 82 | Yes | SAP | 150 | 136 | 103 | 111 | |
| 2 | 82 | Yes | SCR | 154 | 158 | 161 | 160 | |
| 2 | 82 | Yes | TUP | 4.23 | 2.06 | 0.96 | 0.81 | |
| 3 | 72 | No | ALT | 33 | 36 | 29 | 25 | 20 |
| 3 | 72 | No | SAP | 100 | 118 | 145 | 160 | 177 |
| 3 | 72 | No | SCR | 190 | 205 | 200 | 224 | 600 |
| 3 | 72 | No | TUP | 1.44 | -- | -- | 2.25 | 3.0 |
Table 2: Status of liver function and renal function during the follow up after drug switch.
Prognosis
These 2 cases of OLTX who developed FSGS while on FK506, revealed attainment of partial remission of FSGS with stability of RFT upon conversion to CsA from FK506, while the 3rd case where FK was continued, there was progression to ESRD at the end of further 6 years without any remission of GN.
Discussion
This case reports of three cases of OLTX is a retrospective, and at the same time prospective representation of a sequential event of effect of immunosuppression for one organ affecting another vital organ, and depicts an strategy of conversion of a compatible immunosuppression to overcome the apparent adverse outcome of the vital organs. The 3 cases of OLTX were on standard FK base regimen and were stable. However, they developed FSGS in their respective kidneys after a few years. FSGS is a common glomerular finding resulting as a primary phenomenon. Less commonly it represents a result of sustained and persistent injury to the kidney. FK is a calcineurin inhibitor (CNI) that is known to cause striate fibrosis in the renal interstitial tissue after long exposure in renal transplant [19, 20]. However, de-novo FSGS in native kidney while FK is used for non-renal indications is not reported in literature enough [8, 9, 10]. In this regards, these three cases of post OLTX FSGS in native kidney after several years is notable. Drug induced FSGS can be caused by CNI by dint of two pathway: (a) by inducing ischemia to renal tissue as CNI is known to cause vasoconstriction [14, 15] as supported by the need of CCB to counteract it. Renal ischemia is a known cause of FSGS [12]; and (b) by inducing Thrombotic microangiopathy (TMA) in renal tissue [14, 15] which in turn lead to FSGS as TMA is a known cause of secondary FSGS [11]. Our cases were on Fk for liver transplant. FK is more potent then CsA as immunosuppression. It is also more potent in TMA induction and ischemia induction [15]. As evidenced in our case series, basing on the available literatures we hypothesized that FK could be more potent in inducing FSGS than CsA [11, 12, 13, 14, 15, 16]. Therefore we changed FK to CsA in two cases keeping Fk in the 3rd case to continue. The results were self- explanatory. The conversion cases showed remission of proteinuria and stablisation of renal function, while, the case where Fk was not changed to CsA did not show remission of proteinuria. Rather the renal impairment progressively worsened to ESRF. This hard evidence prompted us to report these 3 cases of OTLX to make the transplant community aware of this phenomena, so far a rarely noticed sequela of FK. As there is limited therapeutic option to treat FSGS other than using CNI in order to keep the OLTX functioning and rejection free, a switch to a different kind of CNI appears to be a reasonable alternative. It was presumed that the FSGS would undergo remission when the offending agent, in this case FK for OLTX, is taken off and replaced with a different CNI – CsA. CsA also causes striate fibrosis in the transplant kidney, but occurrence of FSGS in a renal allograft is considered to be a recurrent GN [15]. With this hypothesis FK was changed to CsA in the 2 cases and the 3rd case was kept on FK as before. There was no episode of AR in the 2 case of OLTX post conversion to CsA as proven by Liver biopsy. However, the 3rd case with FK developed recurrent HCV liver disease. Moreover, the case progressed to end-stage renal disease (ESRD) without remission of proteinuria. The association of HCV with FSGS is a known phenomenon [17]. However, not all cases of HCV end up with FSGS. Many cases of liver transplant are associated with presence of HCV liver diseases. Incidence of FSGS in those cases is also not so closely associated with HCV. Two of the three cases of our series had HCV before liver transplant. We changed FK to CsA in one of these 2 cases and kept FK unchanged in the other case of HCV. The 3rd case without HCV also received CsA instead of FK. The 2 cases (one HCV and one without HCV), where we changed FK to CsA, underwent remission of proteinuria with change to CsA and did not progress to ESRF at the time of documentation of this case report. The case with HCV where FK was kept continuing, did not go into remission and rather progressed to ESRF after several years. This observation dissociates the role of HCV from the role of FK in inducing FSGS in kidney, post liver transplant. This observation of dissociation of HCV from FK is further reinforced by the observation of remission of FSGS in the HCV positive case and HCV negative case where proteinuria went into remission after switching FK to CsA. The 2 cases of OLTX, who developed FSGS while on FK506, attained of partial remission with more than 50% reduction of TUP, and stability of RFT upon conversion to CsA from FK506. Renal biopsy was repeated in these 2 cases. The renal biopsy showed stability of glomerular sclerosis without further progression. The case where proteinuria increased and progressed to ESRF was not subjected repeat renal biopsy.
Conclusion
FK506 in OLTX may induce FSGS in the native kidney. This can undergo remission when the medicine is changed to CsA. Immunosuppression for OLTX can be maintained with CsA. Acknowledgement: I deeply acknowledge the contribution of Dr Ali Al-Lehbi of KFSH&RC, Riyadh, 1102, for the production of this case report while I was Assistant Consultant, Renal section there. Conflict of Interest: There is no conflict of interest in the production of this case report. The only interest for the production is meant for sharing this unique experience with global renal and liver transplant community. The cases had been anonymized completely.
References
-
Adam R, Karam V, Delvart V, Trunečka P, Samuel D, et al. (2015) Improved survival in liver transplant recipients receiving prolonged-release tacrolimus in the European Liver Transplant Registry. Am J Transplant 15(5): 1267-1282.
-
Shaked A, Ghobrial RM, Merion RM, Shearon TH, Emond JC, et al. (2009) Incidence and severity of acute cellular rejection in recipients undergoing adult living donor or deceased donor liver transplantation. Am J Transplant 9(2): 301-308.
-
Stifft F, Stolk LM, Undre N, van Hooff JP, Christiaans MH (2014) Lower variability in 24-hour exposure during once-daily compared to twice-daily tacrolimus formulation in kidney transplantation. Transplantation 97: 775-780.
-
Fung JJ, Alessiani M, Abu-Elmagd K, S Todo, R Shapiro et al. (1991) Adverse effects associated with the use of FK 506. Transplant Proc 23(6): 3105-3108.
-
Tauxe WN, Mochizuki T, McCauley J, Starzl TE, Jain A, et al. (1991) A comparison of the renal effects (ERPF, GFR, and FF) of FK 506 and cyclosporine in patients with liver transplantation. Transplant Proc 23(6): 3146-3147.
-
European FK506 Multicentre Liver Study Group (1994) Randomised trial comparing tacrolimus (FK506) and cyclosporin in prevention of liver allograft rejection. Lancet 344(8920): 423-428.
-
José M Álamo, Claudia Olivares, Lydia Barrera, Luis M Marín, Gonzalo Suarez, et al. (2015) Conversion from calcineurin inhibitors to mTOR inhibitors stabilizes diabetic and hypertensive nephropathy after liver transplant. World J Transplant 5(1): 19-25.
-
McCauley J, Fung JJ, Todo S, Jain A, Deballi P, et al. (1991) Changes in renal function after liver transplantation under FK 506. Transplant Proc 23(6): 3143-3145.
-
Bahirwani R, Reddy KR (2009) Outcomes after liver transplantation: chronic kidney disease. Liver Transpl 15(2): S70-S74.
-
Allen AM, Kim WR, Therneau TM, Larson JJ, Heimbach JK, et al. (2014) Chronic kidney disease and associated mortality after liver transplantation--a time-dependent analysis using measured glomerular filtration rate. J Hepatol 61(2): 286-292.
-
(FSGS) TMA causing FSGS.
-
Ben Sprangers, Björn Meijers, Gerald Appel (2016) FSGS: Diagnosis and Diagnostic Work-Up. Biomed Res Int 2016: 4632768.
-
Glen S Markowitz, Andrew S Bomback, Mark A Perazella (2015) Drug-Induced Glomerular Disease: Direct Cellular Injury. Clin J Am Soc Nephrol 10(7): 1291-1299.
-
George Sunny Pazhayattil, Anushree C Shirali (2014) Drug-induced impairment of renal function. Int J Nephrol Renovasc Dis 7: 457-468.
-
Naesens M, Kuypers DR, Sarwal M (2009) Calcineurin inhibitor nephrotoxicity. Clin J Am Soc Nephrol 4(2): 481-508.
-
Carson JM, Newman ED, Farber JL, Filippone EJ (2012) Tacrolimus-induced thrombotic microangiopathy: natural history of a severe, acute vasculopathy. Clin Nephrol 77(1): 79-84.
-
Stehman-Breen C, Alpers CE, Fleet WP, Johnson RJ (1999) Focal segmental glomerular sclerosis among patients infected with hepatitis C virus. Nephron 81(1): 37-40.
-
Vento S, Cainelli F (2002) Does hepatitis C virus cause severe liver disease only in people who drink alcohol? Lancet Infect Dis 2(5): 303-309.
-
Nadasdy T, Allen C, Zand MS (2002) Zonal distribution of glomerular collapse in renal allografts: possible role of vascular changes. Hum Pathol 33(4): 437-441.
-
Stokes MB, Davis CL, Alpers CE (1999) Collapsing glomerulopathy in renal allografts: a morphological pattern with diverse clinicopathologic associations. Am J Kidney Dis 33(4): 658-666.
- Reconstruction of Nasal Defect Using a Local Flap Based in the Nanoperforants Concept: A Case Report
- Transplant Tourism in Japan: Insights from Nationwide Surveys and Emerging Ethical Challenges
- The Challenge of Peritoneal Vaginoplasty in Transgender Women: Review Literature and Personal Perspectives
- Algorithmic Paternalism: Autonomy Versus Automation
- Dermatoscopy in Gorlin Syndrome: Avoiding the Disfigurement in Patients
- How Artificial Intelligence is Ushering in a New Era of Innovation in General and Plastic Surgery: A Short Communication