Dermatoscopy in Gorlin Syndrome: Avoiding the Disfigurement in Patients
Introduction: The Gorlin Syndrome (GS), also known as Naevoid Basal Cell Carcinoma (BCC) Syndrome or Basal Cell Naevus Syndrome. The life expectancy of these patients is good and the greatest concern being the aesthetic and dysfunctional effect of the multiples tumors resections, with implications both at a psychological and social level. The objective of this paper is to demonstrate the efficiency of dermatoscopy in the diagnosis of basal cel carcinoma and their margins to avoid unnecessary resections in Gorlins syndrome, avoiding deformities. Methods: An observational retrospective study was performed on consecutive patients who underwent BCC and dermal and odontogenic cysts exeresis between 2004 and March 2020 that had a follow-up of at least 6 months after surgical resection. The dermatoscopy images were captured using the Dermlite DL4 Dermatoscope. Results: The mean age of beginning BCC is at 15.27 years. Altogether, 168 lesions were resected in the studied patients. Complaints: scarring (71.42%), periorbital region (42.85%), nasal valves incompetence (28.57%), alopecia (42.85%) and negative psychological and social influence (28.57%). Discussion: Several are the possibilities of treatment. Surgical excision is the treatment of choice. A dermatoscope can assess structures till the depth of reticular dermis to visualize subtle features of the subsurface skin structures of the lesion under investigation. Conclusion: The dermatoscope could be used to help in GS treatment considering its accuracy and level of detail to decide which lesion and margin must be resected avoiding disfigurements, without function lost and maintain patients psychologically and socially well conducted.
Abbreviations
GS: Gorlin Syndrome; BCC: Basal Cell Carcinoma; EVD: Ex-Vivo Dermoscopy; UV: Ultraviolet; MC1R:
Melanocorticortin-1 Receptor Gene.
Introduction
The Gorlin syndrome (GS) is an autosomal dominant condition, with complete penetrance and variable expressivity, also known as Naevoid Basal Cell Carcinoma Syndrome or Basal Cell Naevus Syndrome. The genetic basis of this syndrome has been identified with causative mutations in several tumor supressor genes encoding important elements in the hedgehog signaling pathway, including PTCH1, PTCH2 and SUFU [1, 2, 3, 4].
The characteristic features of the disorder are skin manifestations, jaw keratocysts, lamelar (sheet-like) calcification of the falx, childhood medulloblastoma, macrocephaly, ovarian/cardiac fibromas, ocular anomalies, and skeletal anomalies that consists in major or minor diagnostic criteria [5, 6] (Chart 1).
| Major criteria | - Multiple BCCs** or one BCC in a person younger than 20 years |
|---|---|
| - Odontogenic keratocysts | |
| - Palmar or plantar pits | |
| - Lamellar calcification of the falx cerebri | |
| - Medulloblastoma in early childhood | |
| - First-degree relative with GS | |
| Minor criteria | - Bifid, fused or splayed ribs |
| - Other specific skeletal and radiologic abnormalities (pectus excavatum, scoliosis, hemivertebrae, Sprengel’s deformity, syndactyly, bony bridging of the sella túrcica, flame-shaped lucencies of falanges) | |
| - Macrocephaly | |
| - Cleft lip or palate | |
| - Ovarian or cardiac fibroma | |
| - Lymphomesenteric cysts / ocular anomalies (coloboma, congenital cataract, glaucoma, hypertelorism, strabismus, eyelid cysts, pigmentary changes of the retinal epithel) |
*Two major criteria, one major and two minor criteria, or one major and genetic confirmation is required for diagnosis. **Basal cell carcinomas. Chart 1: Diagnostic criteria for Gorlin Syndrome (GS)*.
Skin lesions of basal cell carcinomas (BCC) as well as other skin disorders (milia, epidermoid cysts, chalazia, comedones, palmar and plantar pits) may be present from birth or develop in childhood, being, however, more frequent its appearance between puberty and 35 years. The initial site of appearance of BCC is most frequently the face and nape of the neck, but there is an increased risk of BCC in the whole body including vulva and perianal region. Rarely metastize, but can vary in number from only some to thousands. The numbers of BCC that develop have shown a significant association with skin pigmentation, sun and radiation exposure [2, 5, 7].
The high risk of recurrence of these injuries, as well as the appearance of new ones, leads patients to undergo regular evaluations and, due to their hereditary component, that of their relatives, ideally in the multidisciplinary context, when plastic surgery, stomatology, genetic counseling, among others, will intervene [8].
The term ‘dermoscopy’ (synonym: epiluminescence microscopy) refers to surface microscopy and currently indicates all methods that offer visualization at 10 fold magnification of skin tumoral lesions using optical magnification and fluid immersion or polarized lighting. Dermoscopy improves the ability of physicians to differentiate the various types of skin lesions from one another and to diagnose melanomas. The main principle of dermoscopy screening is the examination of all cutaneous lesions, not only pigmentary or nonpigmentary lesions chosen by the patient or preselected for clinical examination. Two meta-analyses have demonstrated that dermoscopy can improve the sensitivity for recognition of cutaneous tumors in comparison to examination with the naked eye [9].
Objective
The life expectancy of these patients, except in cases of medulloblastoma, is greater than sixty years, being the greatest concern aesthetic and / or functional effect of the treatment of multiple BCC and keratocysts, with implications in both the psychological and social level [10]. The objective of this paper is to demonstrate the efficiency of dermatoscopy in the diagnosis of basal cell carcinoma and their margins to avoid unnecessary resections in Gorlin’s syndrome, avoiding deformities.
Methods
An observational retrospective study was performed on consecutive patients diagnosed with Gorlin syndrome who underwent BCC and dermal and odontogenic cysts exeresis by multidisciplinary and craniofacial team, at SOBRAPAR Hospital, between 2004 and March 2020 using local flaps and total or partial-thickness skin grafts to cover excised areas who had a follow-up of at least 6 months after surgical resection. All individuals on the register have been found to have a mutation in the PTCH gene or meet clinical criteria for diagnosis of Gorlin Syndrome. Those who did not respect these requirements were excluded (Table 1).
| Major Criteria | Ptt 1 | Ptt 2 | Ptt 3 | Ptt 4 | Ptt 5 | Ptt 6 | Ptt 7 | Ptt 8 | Ptt 9 |
|---|---|---|---|---|---|---|---|---|---|
| Lamellar calcification of the falx cerebri | O | X | X | Ø | Ø | Ø | Ø | Ø | X |
| Odontogenic keratocysts | O | X | X | Ø | O | O | Ø | Ø | X |
| Palmar and/or plantar pits (2 or more) | X | Ø | O | X | O | O | O | X | X |
| Single basal cell carcinoma diagnosed before age 30 or multiple basal cell carcinomas (5 throughout life) | X | X | X | O | X | X | X | O | X |
| First-degree relative with Gorlin | X | X | O | X | O | X | X | X | O |
| Medulloblastoma in early childhood | O | O | O | O | O | O | O | O | X |
| Major Criteria | |||||||||
| Pleural or lymphomesenteric cysts | O | O | O | Ø | Ø | O | O | Ø | O |
| Macrocephaly (Head circumference in cm - Mean ± standard deviation ♀ 54.40 ± 0.13 ♂ 55.9 ± 0.17) | 57 | Ø | 56 | Ø | Ø | 58 | 55 | 56 | 59 |
| Cleft lip and / or palate | O | O | O | O | O | O | O | O | O |
| Bone abnormalities (in ribs, extra or bifid; in vertebrae, bifid, scoliosis) | O | X | O | Ø | O | X | Ø | Ø | O |
| Cardiac or ovarian fibroids | O | O | Ø | Ø | O | O | Ø | O | O |
| Eye abnormalities (cataract, pigmentary changes in the retinal epithelium, developmental defects such as strabismus, orbital cyst, microphthalmia, hypereleorbitism) | O | O | X | O | X | X | O | O | O |
| Statistics Data | |||||||||
| Age at onset of injuries or symptoms (years) | 20 | 2 | 0.41 | 3 | 40 | 13 | 12 | 36 | 11 |
| Number of injuries operated (n) | 12 | 69 | 16 | 0 | 48 | 11 | 3 | 0 | 9 |
| Need to expand margins | O | X | O | O | X | X | X | O | O |
| Follow-up (years) | 6 | 13 | 14 | 0 | 10 | 2 | 1 | 0 | 10 |
Table 2: Characteristics of patients with Gorlin Syndrome.
Ptt – patient; X – ptt has this criterion; O - ptt does not have this criterion; Ø - ptt did not bring an exam or did not show up on the day of measurement. Table 1: Characteristics of patients with Gorlin Syndrome.
In the current study, patients from five families were ascertained for GS. The clinical details for each patient were recorded from the hospital notes. The dermatoscopy images were captured using the Dermlite DL4 Dermatoscope - 3GEN (polarized lighting and pigment boost lighting, which enhances pigmentation) and dermatoscopic findings were obtained that suggested that they were basal cell carcinomas.
All subjects were enrolled upon a consent form signed by the patients and/or their parents, in accordance with the Helsinki Declaration of 1975, as amended in 1983. A local Institutional Research and Ethics Board approval was obtained for this study in the protocol number 001/20.
The surgical team treats all the cases, injuries, lesions and cysts by surgical treatment, with surgical margins being chosen for excision of the lesions between 0.4 and 1.00 cm depending on the clinical and dermatoscopic analysis with the margins being for low and high risk of malignancy, respectively. All tissues taken from patients were sent for anatomopathological examination. The patients were evaluated by physical and dermoscopic examination, inspecting the scalp, face, cervical, trunk and upper and lower limbs; genital regions were not evaluated.
In this study, pathological scars, scar contractures, loss of function in the operated area, negative psychological and social influence on patients’ lives were considered disfigurements.
Results
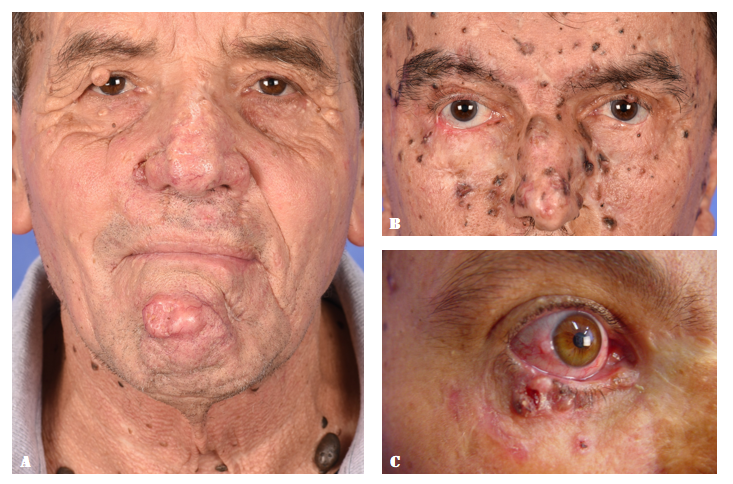
There are 9 Gorlin patients diagnosed in this study, one of the largest unicentric casuistry in Brazil, although, two of them are recently discovered during this study and haven’t undergone to any surgery yet. Confirming statistics, the mean age of beginning BCC is at 15.27 years with a SD of 14.34. Out of the 7 operated patients were found complaints about scarring (71.42%), periorbital region (42.85%), nasal valves incompetence (28.57%), alopecia (42.85%) and negative psychological and social influence (28.57%) (Figure 1).

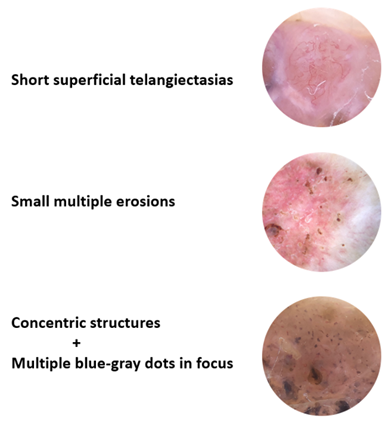
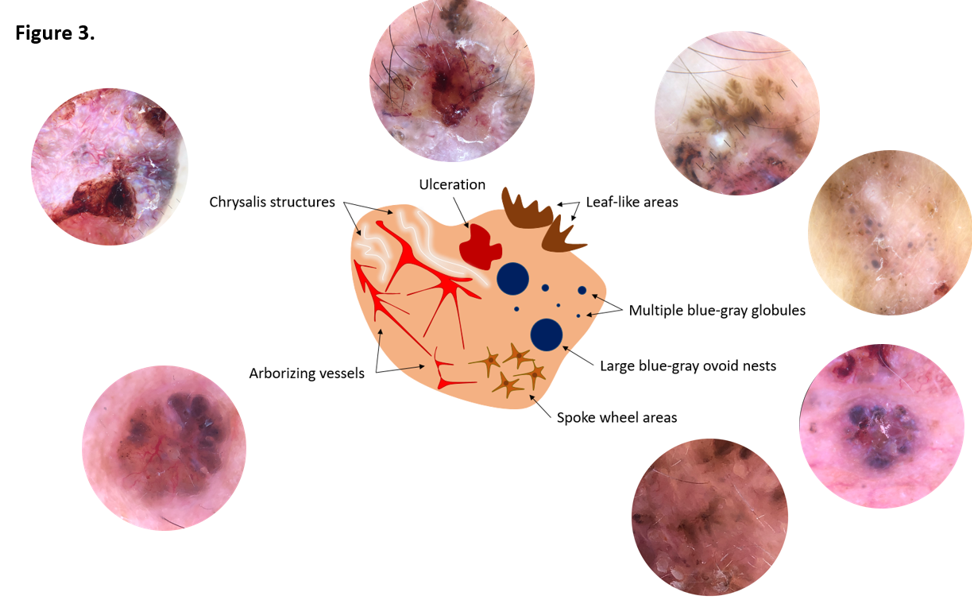
Upon inspection of the 9 patients, without and with the dermatoscope, uncountable lesions were found characteristics of BCC or not, suggesting malignance or benign lesions (Figure 2). Dermatoscopy was primordial to choose which one will be first resect or if it will be resected [11] (Figures 3 & 4). The benign lesions that were found consist in milia, seborrheic cysts, comedones, actinic keratosis, palmar and plantar pits. Basal cell cancers are distinguish from each other in many types and in the studied patients the anatomopathological shows solid, micronodular, pigmented, superficial, multifocal, scleridermiform, polypoid, cystic, ulcerated. Gorlin’s patients have a wide variety of lesions that enabled to find all BCC characteristics in dermatoscopy, even the ones that are less common. Altogether, 168 lesions were resected in the studied patients, an average of 24 ± 22.81 tumors per patient who underwent surgery. The resections came from the most diverse surgical sites, with a higher concentration of lesions on the scalp, face and trunk. Even while always taking care to choose the margins (0.4-1.0 cm), among the evaluated patients, four patients needed surgery to enlarge the margins at some point during the analyzed period.
Discussion
Described at first in 1894 by W. Jarich e J.C. White, it was just in 1960 that R. J. Gorlin and R.W. Goltz (N Engl J Med. 1960 May 5;262:908-12) established the criterias [8]. Chart 1 A wide prevalence around 1:57.000 to 1:256.000 with equal gender distribution. Even that 70-80% of patients have an affected progenitor, the first case in family could have only a few mild manifestations, explained by somatic mosaicism [8].
There is adequate variation in single families to believe that environmental exposure and perhaps modifier genes may justify much of the variation. The number of BCC that develop have shown a significant association with skin pigmentation (dark skin types developing fewer tumors) and sun exposure. Basal cell cancers are found in approximately three-fourths of non-hispanic white patients with GS but are less frequent in affected African-Americans and Asians. Common single nucleotide genetic polymorphisms in melanocorticortin-1 receptor gene (MC1R) and TERT- CLPTM1L may be associated with an earlier age of them [2, 10, 12].
A role of sun exposure in the pathogenesis of basal cell cancers in these patients is supported by the finding that tumors from individuals with a low number of BCC have fewer somatic ultraviolet (UV)-signature mutations compared with tumors from individuals with a high number of tumors. The risk of recurrence of non-melanoma skin cancer based on location, low risk in trunk and extremities, medium risk in cheeks, forehead, neck, scalp and high risk in central face, eyelids, eyebrows, periorbital area, lips, chin, mandible, pre and postauricular areas, genitalia, hands and feet [10, 12].
These patients are particularly sensitive to effects of radiation, and the development of multiple BCC within irradiated fields in affecteds is well described [10]. Having said that it is important to remember that one of diagnosis criteria is medulloblastoma which needs radiation treatment. Besides of that the other criteria need remembership for correctly multidisciplinary treatment (Chart 2) and differentiate from other diagnosis, Sotos syndrome, Bazex syndrome, Rombo syndrome, Brooke-Spiegler syndrome [8].
| Skeletal | - Scoliosis |
|---|---|
| - Arachnodactyly | |
| - Agenesis of ribs | |
| - Flat feet | |
| - Cervical ribs | |
| - Hallux valgus | |
| - Polydactyly | |
| - Cortic defects in long bones | |
| - Pelvic calcification | |
| Skin | - Milia |
| - Comedones | |
| Craniofacial | - Brachycephaly |
| - Choroidal cysts | |
| - Calcifications of the cerebellar tent | |
| Oral | - Ogival palate |
| - Malocclusion | |
| - Ectopic teeth | |
| - Maxillary fibrosarcomas | |
| - Fibromas of the palate or maxillary sinuses | |
| - Ameloblastoma | |
| Neuronal | - Meningioma |
| - Schizophrenia | |
| - Cognitive delay | |
| - Deafness | |
| - Hydrocephalus | |
| - Anosmia | |
| - Agenesis of the corpus callosum | |
| Visual | - Exotropia |
| - Amaurosis | |
| - Ptosis | |
| - Chalazion | |
| Reproductive | - Uterine fibroma |
| - Supernumerary nipple | |
| - Gynecomastia | |
| - Hypogonadism | |
| - Cryptorchidism | |
| Others | - Inguinal hernia |
| - Renal anomalies |
“Síndrome de Gorlin-Goltz: caso clínico. Nascer e Crescer, 2014; 23(2): 87-91” Chart 2: Anomalies associated with Gorlin Syndrome (excluding major and minor criteria).
Several are the possibilities of treatment, cryotherapy, electrodesiccation and curettage (small and low risk BCC), carbon dioxide laser therapy (low risk BCC), photodynamic therapy (superficial lesions), A-vitamin analogs and D-vitamin (quimioprofilaxis), topical therapies (imiquimod 5%, 5-fluorouracil, delta-aminolevulinic acid), Vismodegib (approved to treat inoperable, locally advanced, or metastatic BCC) and surgical excision. Radiotherapy must be avoided [1, 3, 4, 8, 9, 10, 11, 12].
Surgical excision is the treatment of choice and offers overall cure rates greater than 90 percent. For low-risk nonmelanoma skin cancers extending into the dermis only, excision with standard margins (4 mm for basal cell carcinoma). A 2-mm margin yields a cure rate of 94 percent in small (<1 cm) nodular basal cell carcinomas. Margins of 3 to 5 mm around a tumor and extending into subcutaneous fat are recommended for primary basal cell carcinomas less than 2 cm in diameter. Basal cell carcinomas more than 2 cm may require margins as wide as 10 mm, as do tumors with aggressive histologic growth patterns. Frozen sections of tumor margins are expensive and not recommended for every suspected nonmelanoma skin cancer. They are unnecessary for well-circumscribed lesions less than 1 cm in diameter, for lesions in noncritical areas in locations where wide surgical margins can be taken, for lesions where repair requires only direct suture closure, and for low-risk patients. Indications for Mohs surgery include tumors greater than 2 cm, recurrent tumors, tumors in high-risk areas, tumors with indistinct clinical margins, and tumors in cosmetically sensitive regions. Caution must be exercised in multifocal tumors, such as recurrent tumors within a surgical scar [4,10,12,].
Surgical procedure is the golden standard for the treatment of Gorlin syndrome. Taking into consideration that Gorlin’s patients have uncountable lesions and that the margins vary according to the lesions risk; if chose criterion is always to resect the biggest margin to avoid residual BCC, considerable sequels will disfigure these patients [13]. Moreover, the lesions sometimes are close and the margins overlap each other.
A dermatoscope functionally simulates a magnifying lens, with the added features of much higher magnification, and an adjustable inbuilt illuminating system. A hand-lens even with in-built illumination, can not see beyond the surface of the skin because of the reflection and scattering of light from the stratum corneum. A dermatoscope can assess structures till the depth of reticular dermis and record images for future comparison. The basic principle of dermoscopy is transillumination of a lesion and studying it with high magnification to visualize subtle features improving the visibility of the subsurface skin structures of the lesion under investigation. As a non-invasive technique, dermoscopy is essentially free of complications [14].
The dermatoscope is an immensely versatile tool, with many more uses beyond diagnosis. Its uses beyond diagnosis include disease activity evaluation, early comparison of pre- and post-treatment, Ex-Vivo Dermoscopy (EVD) to improve histopathological evaluation, better doctor-patient communication, dermoscopic images as an evolving tool for clinical studies, dermoscopy in Dermatosurgery & Aesthetics [14].
Conclusion
The dermatoscope could be used to help in GS treatment considering its accuracy and level of detail to decide which lesion and margin must be resected. Given that the margins overlap each other, it can help to keep healthy skin between lesions especially in vital areas and/or maintaining function. Dermatoscopy and its accurate diagnosis associated with surgical methods makes possible to avoid disfigurements, without function lost and mantain patients psychologically and socially well conducted.
References
-
Mendes-Abreu J, Pinto-Gouveia M, Tavares-Ferreira C, Brinca C, Vieira R (2017) Síndrome de Gorlin-Goltz: Diagnóstico e Hipóteses de Tratamento. Acta médica portuguesa 30(5): 418.
-
Jones EA, Sajid MI, Shenton A, Evans DG (2011) Basal Cell Carcinomas in Gorlin Syndrome: A Review of 202 Patients. Journal of Skin Cancer 2011: 217378.
-
Hill CR, Theos A (2019) What’s new in genetic skin diseases. Dermatol Clin 37(2): 229-239.
-
Vieira EC, Patricia FLA, Marques SA, Marques EAM, Stolf HO (2012) Síndrome de Gorlin. Diagn Tratamento 17(3): 110-114.
-
Durmaz CD, Evans G, Smith MJ, Ertop P, Akay BN, et al. (2018) A novel PTCH1 frameshift mutation leading to nevoid basal cell carcinoma syndrome. Cytogenetic and Genome Research 154(2): 57-61.
-
Reinders MG, Van Hout AF, Cosgun B, Paulussen AD, Leter EM, et al. (2018) New mutations and an updated database for the patched-1 (PTCH1) gene. Mol Genet Genomic Med 6(3): 409-415.
-
Oliveira LNB, Tolstoy F, Lobão D (2014) Síndrome de Gorlin Goltz: relato de um caso exuberante. Surgical & Cosmetic Dermatology 6(3): 28992.
-
Domingues S, Pereira S, Machado A, Bezerra R, Figueira F, et al. (2014) Gorlin-Goltz: caso clínico. Nascer e Crescer 23(2): 87-91.
-
Grajdeanu IA, Vata D, Statescu L, Adriana Popescu I, Porumb-Andrese E, et al. (2020) Use of imaging techniques for melanocytic naevi and basal cell carcinoma in integrative analysis (Review). Experimental and Therapeutic Medicine 20(1): 78-86.
-
Benjamin Barankin, Goldenberg G (2024) Nevoid basal cell carcinoma syndrome (Gorlin syndrome) – UpToDate.
-
Peter CN, Geoffrey CG (2016) Plastic Surgery. In: 4th(Edn.), Principles 1(28): 531.
-
Netscher DT, Leong M, Orengo I, Yang D, Berg C, et al. (2011) Cutaneous malignancies: melanoma and nonmelanoma types. Plast Reconstr Surg 127(3): 37e-56e.
-
Kuhn-Dall’Magro A, Ottoni R, Lauxen J, Santos RD, Valcanaia TDC, et al. (2014) Gorlin-goltz syndrome – cases report 19(2).
-
Sonthalia S, Yumeen S, Kaliyadan F (2024) Dermoscopy Overview and Extradiagnostic Applications. In: StatPearls, Treasure Island, Finland.
- Reconstruction of Nasal Defect Using a Local Flap Based in the Nanoperforants Concept: A Case Report
- Transplant Tourism in Japan: Insights from Nationwide Surveys and Emerging Ethical Challenges
- The Challenge of Peritoneal Vaginoplasty in Transgender Women: Review Literature and Personal Perspectives
- Algorithmic Paternalism: Autonomy Versus Automation
- How Artificial Intelligence is Ushering in a New Era of Innovation in General and Plastic Surgery: A Short Communication
- Inferior Pedicle Mammoplasty for Complications of Free Silicone Injections to the Breast