The Challenge of Peritoneal Vaginoplasty in Transgender Women: Review Literature and Personal Perspectives
Background: Peritoneal vaginoplasty has re-emerged as an alternative technique in transfeminine gender-affirming surgery due to its potential advantages over penile inversion and skin graft methods. However, variable techniques, complication rates, and long-term outcomes raise important clinical considerations. Objective: To review and synthesize the available literature on peritoneal vaginoplasty in transgender women and provide personal perspectives on its anatomical challenges, technique-specific risks, and long-term implications. Methods: A systematic literature search was conducted using PubMed, Scopus, and Web of Science. Studies describing peritoneal vaginoplasty in transgender women were included. Non-surgical studies, MRKH cases, review articles, and unclear techniques were excluded. Techniques, vascular supply, complications, and outcomes were analyzed. Results: Fifteen studies published between 2015 and 2025 met the inclusion criteria. Techniques included double-flap pull-through approaches, three-flap techniques, pedicled peritoneal flaps, and extended posterior bladder flaps. Reported complications included hypergranulation, neovaginal stenosis, difficulty with dilation, and rare intra-abdominal hernias. Outcomes varied widely depending on flap design and anastomotic tension. Conclusion: Peritoneal vaginoplasty offers a viable but technically challenging option for transgender women. Differences in epithelial interface (peritoneum-to-skin) influence healing and complication profiles. Posterior bladder-based flaps may provide the most reliable outcomes. Long-term, high-quality comparative studies are needed.
Abbreviations
MRKH: Mayer-Rokitansky-Kuster-Hauser; PIV: Penile Inversion Vaginoplasty; DIEA: Deep Inferior Epigastric Artery.
Introduction
Peritoneal vaginoplasty was originally developed by Davydov and Rothman for the treatment of congenital vaginal agenesis in Mayer–Rokitansky–Kuster–Hauser
(MRKH) syndrome [1, 2]. The technique involves mobilizing peritoneum to reconstruct a neovaginal canal, allowing a moist, hairless lining that closely mimics native vaginal mucosa. Its application in transgender women has gained widespread attention due to perceived advantages over penile skin inversion or full-thickness skin graft vaginoplasty, including potential self-lubrication and avoidance of hair- bearing tissue [3]. Multiple variations of peritoneal flap vaginoplasty have since been described, such as single posterior bladder flaps, double pull-through flaps, three-flap techniques, and pedicled flaps [4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17].
However, important anatomical differences exist. In cisgender women, peritoneum (mesoderm) is anastomosed to vaginal mucosa (endoderm), whereas in transgender women it is anastomosed to penile or scrotal skin (ectoderm). These differing epithelial interfaces may significantly affect healing, sensitivity, and long-term outcomes. Despite increasing adoption of peritoneal vaginoplasty, evidence remains fragmented. This review aims to evaluate the available literature, classify the main peritoneal flap techniques used for transgender women, and summarize complication profiles and outcomes. The author also provides a personal perspective based on anatomical principles and published data.
Materials and Methods
Search Strategy
A comprehensive literature search was conducted using PubMed, Scopus, and Web of Science from inception to 2025. Search terms included: “gender-affirming surgery”; “sex reassignment surgery”, “peritoneal vaginoplasty.”
Inclusion Criteria
- Studies describing peritoneal vaginoplasty in transgender women
- Primary surgical outcome data
- Clearly described operative techniques
Exclusion Criteria
- Duplicated studies
- Non-surgical studies
- MRKH reconstruction
- Review articles, book chapters
- Unclear techniques or mixed cohorts without trans- specific data
Data Extraction
- Eligible studies were reviewed for:
- Type of peritoneal flap
- Vascular supply
- Method of anastomosis
- Postoperative complications
- Short- and mid-term outcomes
- Year of publication Due to the limited number of studies, all eligible articles were included regardless of sample size.
Results
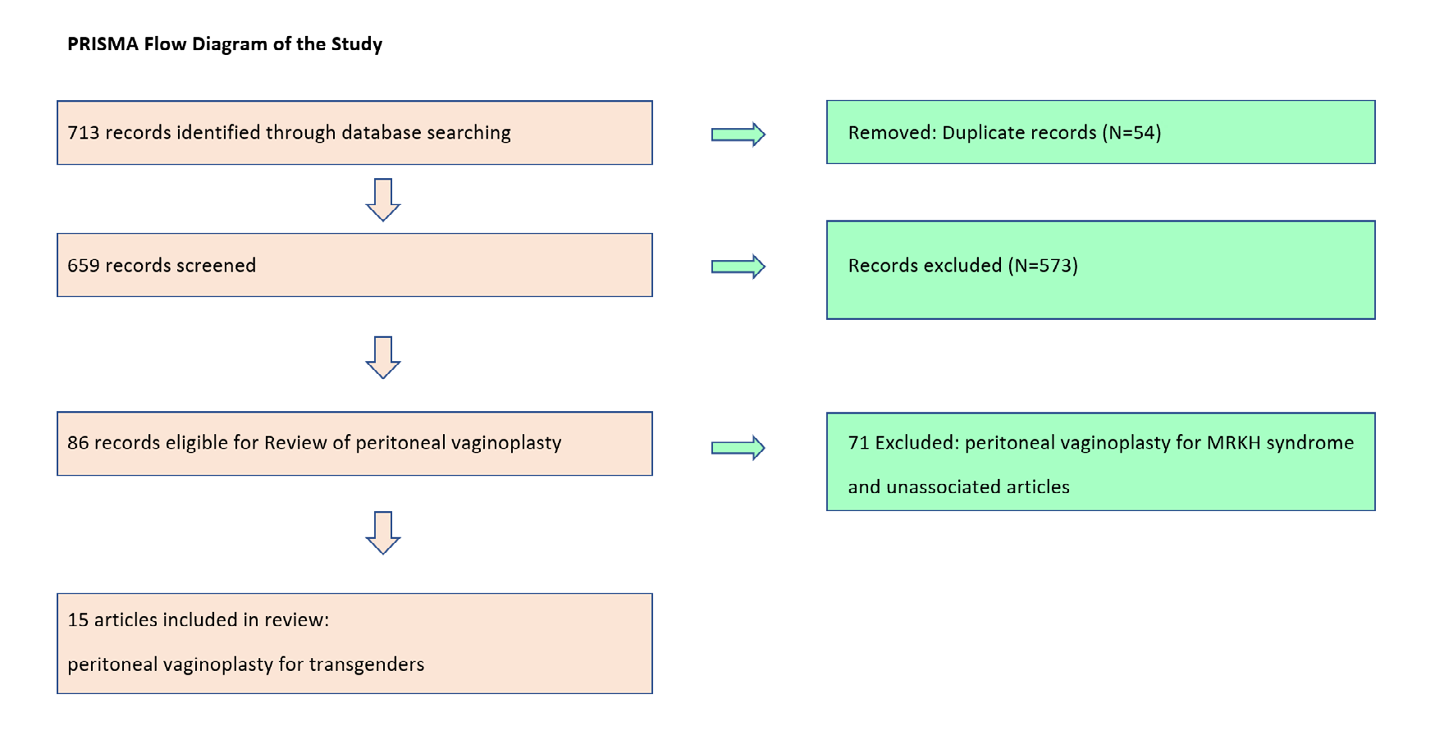
A total of 15 articles published between 2015 and 2025 met inclusion criteria (Figure 1 & Table 1). Techniques were grouped as follows:
- Double-flap pull-through peritoneal vaginoplasty
- Three-flap (modified Davydov) techniques
- Pedicled peritoneal flaps
- Extended posterior bladder peritoneal flap techniques
Summary of reviewed articles and timeline of peritoneal flaps.
| Long-term complications (>12 months po.) | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Author(s) Year | N | Peritoneal Flap Type | Blood Supply | Surgical Technique | Vaginal Depth | Vagina Stenosis | Hyper Granulation Tissue | Bowel Obstr- uction | Long-term Complications (>12 months po.) Patient Satisfaction Outcome |
| Jacoby, et al. [4] | 41 | Double-flaps | N/A | Robotic | 14.2 cm (mean) | N/A | N/A | N/A | N/A |
| Katz M, et al. [9] | 8 | Double-flaps | N/A | Robotic | 14.5 cm (mean) | N/A | N/A | N/A | N/A |
| Dy, et al. [5] | 145 | Double-flaps | N/A | Robotic | 13.6- 14.1 cm | 2 cases | 2 cases | 2 cases | N/A |
| Lava, et al. [6] | 41 | Double-flaps | N/A | Robotic | N/A | N/A | N/A | N/A | N/A |
| Dy, et al. [5] | 24 | Double-flaps | N/A | Robotic | 13.6 cm (mean) | N/A | N/A | N/A | N/A |
| Castanon, et al. [7] | 52 | Double-flaps | N/A | Laparoscopic | 14.7 cm (mean) | N/A | N/A | Patient Satisfaction 96% | |
| Blasdel, et al. [8] | 54 | Double-flaps | N/A | Robotic | 14.5 cm (mean) | N/A | N/A | N/A | |
| Lava, et al. [6] | 21 | Double-flaps | N/A | Robotic | 12.8- 13.2 cm | 5 cases | 6 cases | N/A | |
| Luna, et al. | 11 | Modified Davydov | N/A | Robotic | 15.0 cm (mean) | N/A | N/A | N/A | N/A |
| Haile, et al. [11] | N/A | Triple-flaps | N/A | Robotic | 14.7 cm (mean) | N/A | N/A | N/A | N/A |
| Suwajo, et al. [12] | 1 | Pedicled flap | DIEA | Laparoscopic | 14.0 cm | None | N/A | N/A | N/A |
| Masah, et al. | 5 | Pedicled flap | DIEA | Laparoscopic | 15.0 cm | N/A | N/A | N/A | |
| Smith, et al. [14] | 10 | Extended posterior bladder | N/A | Robotic | 12.5 cm (mean) | 2 cases | Patient Satisfaction 80% | ||
| Morelli, et al. [15] | 8 | Extended posterior bladder | N/A | Robotic | N/A | N/A | N/A | N/A | |
| Johnston, et al. [16] | 33 | Extended posterior bladder | N/A | Robotic | 11.0 (mean) | 36% | N/A | ||
| Ratanalert, et al. [17] | 10 | Extended posterior bladder | N/A | Laparoscopic | 12.5- 15.0 cm | 1 case | N/A | N/A | N/A |
Table 1: Timeline and summary of included peritoneal flap vaginoplasty studies (2015-2025).
Remark: 1. DIEA: Deep Inferior Epigastric Artery. 2. Double-flap: Anterior and posterior peritoneal flaps(pulled through technique). Table 1: Timeline and summary of included peritoneal flap vaginoplasty studies (2015-2025).
Discussion
In 2019, Jacoby, et al. [4] first described a modified Davydov pull-through peritoneal flap technique for secondary vaginoplasty in transgender women, specifically to augment neovaginal depth in cases of inadequate depth after penile inversion vaginoplasty (PIV). This technique utilized both anterior and posterior peritoneal flaps (double- flap technique). However, it demonstrated high rates of vaginal stricture and intravaginal hypergranulation tissue. Subsequent innovations aimed to reduce complication rates and improve outcomes, including single pedicled peritoneal flaps, three-flap configurations, and posterior bladder-based flaps.
Double-Flap (Pull-Through) Technique
The double-flap technique involves creating anterior and posterior peritoneal flaps. The anterior flap is harvested from the peritoneum overlying the posterior bladder and extended superiorly to the anterior abdominal wall, while the posterior flap is harvested from the pararectal peritoneum. The anterior flap is then folded downward and anastomosed to the posterior flap to create a tubular cavity. A perineal incision is made to develop the neovaginal canal. The peritoneum is opened into the abdominal cavity, after which the peritoneal tube is pulled through the canal and anastomosed to penile skin. In this method, part of the anterior rectal surface is included within the posterior flap. Both flaps are mobilized inferiorly into the neovaginal canal, hence the term “pull-through technique.” Several groups have employed this method, including Dy, et al. [5], Lava, et al. [6], Castañon, et al. [7], Blasdel, et al. [8] and Katz, et al. [9]. Among these, Lava, et al. [6] provided the most detailed outcome analysis, reporting hypergranulation tissue in 2 of 21 patients and complete vaginal stenosis in 7 of 21 patients at 30 days postoperatively. Dy, et al. [5] reported chronic granulation tissue in 2 of 24 patients. Robinson, et al. [10] described cases of internal herniation through peritoneal defects, resulting in acute abdominal pain that required reoperation.
Three-Flap Technique
Haile, et al. [11] described a robotic three-flap peritoneal vaginoplasty technique, harvesting peritoneal flaps from the pelvic sidewalls, posterior bladder surface, and the pararectal fossa. These were fashioned into a rhomboid configuration and anastomosed inferiorly to the penile skin flap. This approach represents a modification of the original Davydov procedure. However, the reported patient outcomes were unclear and limited in detail.
Pedicled Peritoneal Flap
Suwajo, et al. [12] and Sachan, et al. [13] described early experience with pedicled peritoneal flaps based on isolated peritoneal branches of the deep inferior epigastric artery (DIEA). These flaps were tubularized and their apex positioned into the neovaginal canal, followed by anastomosis to inverted penile skin. Although technically appealing due to their preserved vascularity, available series remain small and long-term outcomes are not well established.
Extended Posterior Bladder Flap
Smith, et al. [14] introduced a single posterior bladder peritoneal flap anastomosed to inverted penile skin. This wide-based flap provides robust vascularity and may be less invasive than double-flap techniques. Morelli, et al. [15] later described an extended posterior bladder–urachus hinge flap, reporting low intra-abdominal complication rates, procedural safety, effectiveness, and favorable patient satisfaction. Johnston, et al. [16] used a single anterior peritoneal flap secured with a “hitch stitch” to reduce anastomotic tension. Despite this innovation, 12 of 33 patients (36%) developed some degree of vaginal stenosis, and 13 of 33 (39%) reported difficulty with dilation, although no cases of hypergranulation tissue were observed. Ratanalert, et al. [17] reported vaginal stenosis in 1 of 10 patients at 3 months postoperatively .
Summary of Reported Outcomes
- Double-flap pull-through: High rates of vaginal stenosis, hypergranulation, and rare internal hernia (e.g: Dy, et al. [5], Lava, et al. [6] and Robinson, et al. [10]).
- Three-flap: Limited outcome data; technique feasible but poorly reported.
- Pedicled peritoneal flap: Small case series; maintains vascularity but limited follow-up.
- Extended posterior bladder flap: Lower anastomotic tension, fewer complications, and promising patient- reported satisfaction.
Personal Perspective
The peritoneum originates from mesoderm and is inherently more sensitive than skin, which is derived from ectoderm. This embryologic difference likely contributes to the discomfort and difficulty many patients experience during early postoperative dilation. In the original Davydov procedure, mesoderm-derived peritoneum was anastomosed to endoderm-derived vaginal mucosa, providing favorable epithelial compatibility. In transgender women, however, peritoneum must be anastomosed to penile skin- an ectodermal tissue-resulting in a less harmonious interface and potentially higher rates of long-term complications.
The pull-through technique is particularly prone to early
and late complications. The pararectal posterior flap exhibits significant “memory” or spring-back tension, leading to increased risks of internal herniation, hypergranulation tissue formation, and late stenosis. Although pedicled peritoneal flaps preserve vascular integrity, relatively few centers have adopted this technique, and outcomes remain limited. Due to its tissue characteristics, the peritoneal lining of the neovagina often remains hypersensitive for 3-6 months postoperatively. Patients with poor adherence to dilation regimens are therefore at increased risk of developing stenosis.
More recently, extended posterior bladder peritoneal flaps appear to offer more reliable outcomes, with lower anastomotic tension and fewer complications. Based on the author’s clinical observations, the anastomotic tension between peritoneum and penile skin is substantially lower compared with pull-through (double-flap) approaches, reducing the likelihood of hypergranulation tissue. A major limitation of the existing literature is the small number of published studies and the predominance of short-term follow-up.
Conclusion
Peritoneal vaginoplasty in transgender women remains a technically demanding procedure with multiple variations. Pain during dilation and risks of stenosis remain key challenges. Current evidence suggests that extended posterior bladder-based peritoneal flaps may offer the most favorable balance of safety and function. Long-term prospective studies are essential to establish optimal techniques and refine postoperative management.
Conflict of Interest
None declared.
References
-
Davydov SN, Zhvitiashvili OD (1974) Formation of vagina (colpopoiesis) from peritoneum of Douglas pouch. Acta Chir Plast 16(1): 35-41.
-
Tondu M, Allepot K, Youkharribache A, Cristofari S (2025) The use of peritoneum in female genital gender- affirming surgery: A systematic review. Ann Chir Plast Esthet 70(1): 26-33.
-
Horbach S, Bouman MB, Smit JM, Ozer M, Buncamper ME, et al. (2015 ) Outcome of vaginoplasty in male-to- female transgender individuals: A systematic review. J Sex Med 12(6): 1499-1512.
-
Jacoby A, Maliha S, Granieri MA, Dy GW, Bluebond- Langner R, et al. (2019) Robotic Davydov peritoneal flap vaginoplasty for augmentation of vaginal depth in feminizing vaginoplasty. J Urol 201: 1171-1176.
-
Dy GW, Blasdel G, Shakir NA, Bluebond-Longner R (2021) Robotic Peritoneal Flap Revision of Gender Affirming Vaginoplasty: a Novel Technique for Treating Neovaginal Stenosis. Urol 201(6): 1171-1176.
-
Lava CX, Lauren EB, Karen RL, Rachel NR (2024) A comparative analysis of peritoneal flap and intestinal vaginoplasty for management of vaginal stenosis. J Plast Reconstr Aesthet Surg 98: 55-63.
-
Castanon C, Matic S, Bizic M, Stojanovic B (2022) Laparoscopy Assisted Peritoneal Pull-Through Vaginoplasty in Transgender Women. Urology 166: 301- 302.
-
Blasdel G, Kloer C, Parker A, Shakir N, Zhao LC, et al. (2023) Genital Hypoplasia before Gender-Affirming Vaginoplasty: Does the Robotic Peritoneal Flap Method Create Equivalent Vaginal Canal Outcomes? Plast Reconstr Surg 151(4): 867-874.
-
Katz M, Dy G, Nolan I, Bluebond-Langner R, Zhao L (2019) V04-03 Robotic peritoneal flap technique for revision vaginoplasty in transgender women. J Urol 201(4): e491-e492.
-
Robinson IS, Blasdel G, Bluebond-Langner R, Zhao LC (2022) The Management of Intra-abdominal Complications Following Peritoneal Flap Vaginoplasty. Urology 164: 278-285.
-
Haile E, Agrawal S, Fascelli M (2024) Peritoneal Vaginoplasty in Gender Diverse Patients. Curr Obstet Gynecol Rep 13: 136-143.
-
Suwajo P, Ratanalert W, Sooksatian K, Uerpairojkit K, Dusitanond N, et al. (2020) Pedicled peritoneal flap vaginoplasty in male-to-female gender affirmation surgery: a case report. Urogynecology 26(8): e23-e26.
-
Sachan A, Jain P, Sharma P, Goel V (2022) Male-to-Female Gender Affirmation Vaginoplasty via Laparoscopic Pedicled Peritoneal Flap-An Initial Experience. Indian J Plast Surg 55(2): 211-215.
-
Smith SM, Yuan N, Stelmar J, Gupta A, Kim HL (2022) An Alternative Option for Gender-Affirming Revision Vaginoplasty: The Tubularized Urachus-Peritoneal Hinge Flap. Sex Med 10(6): 100572.
-
Morelli G, Zucchi A, Ralp D, Perotti A, Sollazzi E, et al. (2023) A single pedicled robotic peritoneal flap in penile inversion vaginoplasty augmentation. BJU Int 131(1): 125-129.
-
Johnston AW, Soyster ME, Koch MO, Roth JD (2025) Gender-affirming Robotic Tubularized Peritoneal Vaginoplasty: Feasibility and Outcomes. Urology 195: 191-198.
-
Ratanalert W, Pobpan P (2021) Full-length Peritoneal Flap Vaginoplasty: A Feasible Approach for Hairless Neovaginal Reconstruction in Gender-affirming Surgery. Plast Reconstr Surg.
- Reconstruction of Nasal Defect Using a Local Flap Based in the Nanoperforants Concept: A Case Report
- Transplant Tourism in Japan: Insights from Nationwide Surveys and Emerging Ethical Challenges
- Algorithmic Paternalism: Autonomy Versus Automation
- Dermatoscopy in Gorlin Syndrome: Avoiding the Disfigurement in Patients
- How Artificial Intelligence is Ushering in a New Era of Innovation in General and Plastic Surgery: A Short Communication
- Inferior Pedicle Mammoplasty for Complications of Free Silicone Injections to the Breast