Comparison of Regenerative Changes in Peripheral Nerve Injuries Treated with a Regenerative Tube with Human Mesenchymal Cells and Platelet Rich Plasma Lysate Versus a Nerve Graft in Rats
Peripheral nerve injuries are a frequent pathology, and complete recovery cannot be achieved if nerve segment loss accompanied by soft tissue and concomitant bone injuries occurs. Objective: To compare the degree of nerve regeneration in peripheral nerve lesions with loss of nervous tissue after treatment with the current "gold standard", consisting of interposition of a nerve graft, and the use of a decellularized regenerative tube including mesenchymal stem cells (MSCs) and platelet rich plasma lysate. Materials and Methods: An experimental study was conducted in Wistar rats weighing 250-300 gdivided into three groups as follows: Group 1, a 1.5-cm resection was reconstructed with a nerve graft. Group 2, a 1.5-cm resection was reconstructed with interposition of a regenerative tube. Group 3, a 1.5-cm resection was reconstructed with an interpositional regenerative tube with MSCs derived from adipose tissue and platelet-rich plasma lysate. After four weeks, a biopsy of the nerve distal to the lesion and reconstruction, along with axonal counting by hematoxylin and eosin staining, were performed to compare the three groups (STATA 12). Results: The quantitative variables were compared among the three groups. The mean numbers of regenerated type A axons obtained in each group were as follows: Group 1: 485.1, Group 2: 14.2, and Group 3: 93.8.Astatistically significant difference was found among the groups. Conclusions: Improvement of axonal regeneration was observed in Group 3 compared to Group 2. This is the first experimental study to use this novel biological platform for the regeneration of peripheral nerves with xenogeneic MSCs; however, the follow-up time was limited, and the results may be improved with a longer follow-up period.
Introduction
In addition to timely intervention, the success of axonal regeneration after a peripheral nerve injury depends on the surgical technique, magnitude of the injury, nerve coaptation without tension, adequate coverage, and the interaction of key components at the cellular level in a synchronized manner, such as the extracellular matrix, nerve growth stimulating factors, cells that support axonal growth, and support structures that allow the directed growth of nervous tissue towards the target organs of each nerve [1]. To date, the best "scaffolding" or support to direct axonal growth has been an autologous nervous graft placed as a bridge between the section ends of the affected nerve. This technique has shown good results in approximately 60% of cases, but this percentage depends on factors such as age, comorbidities, and associated injuries in addition to the morbidity that results in the donor area and the corresponding functional loss [2]. Therefore, the replacement of autologous nerve grafts with different types of supports has been investigated with variable results in both animal models and clinical applications in humans. These results are reproducible for defects of up to 3 cm. Additionally, the support must have characteristics such as biocompatibility, biodegradability, porosity (for interaction with extracellular matrix receptors, which allows attachment of anchoring ligands, and neuronal growth factors, which favors cell proliferation), and adequate biological and mechanical properties so that the axons can grow, thus generating the necessary environment for an adequate regeneration [3, 4]. Substances or cells that positively influence axonal regeneration have been used as supports, including adipose tissue mesenchymal stem cells, which have a paracrine response to the secretion of nerve growth factors [5, 6, 7, 8, 9, 10, 11, 12], in addition to the ability to differentiate into Schwann cells (SC), which are crucial for axonal growth [13, 14, 15]. Several studies have shown that fibrin directs axonal growth during regeneration and can be obtained from platelet-rich plasma (PRP). When activated, PRP can also secrete many growth factors that promote regeneration [16]. The combination of these different therapies can improve the degree of nerve regeneration as indicated by axonal growth to the distal region of the lesion [1]. The objective of this study was to compare the regenerative changes in sciatic nerve lesions in Wistar rats (2 to 3 months of age weighing 250 to 300 g) using autologous nerve grafts versus a regenerative tube with mesenchymal cells (MSCs) derived from human adipose tissue and PRP lysate. The regenerative potential was evaluated for each group using light microscopy and axonal counting with hematoxylin and eosin staining.
Materials and Methods
Animals
Twenty-one 9-week-old Wistar rats weighing 250 to 300 g were included. The protocol and all procedures conducted on the rats were approved by the animal care committee of the National Institute of Health of Colombia. The rats were kept in polycarbonate cages. The facilities had a controlled temperature (22±2 °C), 40-65% humidity, and a 12-h light/dark cycle. Rats were fed a standard laboratory diet and allowed free access to drinking water.
Scaffold
Decellularized tracheas obtained from Wistar rats euthanized in other studies were used. Cleaning was performed to obtain the tracheal tissue, which was subjected to decellularization treatment with sodium deoxycholate (Sigma) at a concentration of 4% wv, 1% v/vTritonX-100, and 0.5% SDS at pH9.0, followed by enzymatic digestion with deoxyribonuclease-I (DNAase)
(Sigma). Decellularization was confirmed with hematoxylin and eosin staining.
Liposuction and Cell Culture
The Research Ethics Committee of the Central Military Hospital approved the protocol (code 2015-052). Liposuctioned material was obtained from an individual submitted to body contouring surgery after signing informed consent. The vascular stromal fraction was obtained by enzymatic digestion with 0.75% collagenase type II. The cells were cultured in plastic T25 culture flasks (TTP) at a density of 1×106 cells/cm2, with DMEM- LG supplemented with 10% FBS and1% penicillin- streptomycin and amphotericin (PSA) at a temperature of 37 °C and an atmosphere of 5% CO2. Once 80% confluence was obtained, the cells were enzymatically dissociated with trypsin and plated at a density of 5×103 cells/cm2. According to the MSC criteria of the International Society of Cell Therapy (ISCT), the expression of CD73 PerCP, CD90 FITC and CD105 APC (BD®) and the absence of the hematopoietic markers CD34 PE/CD45 PE and HLA-DR PE was verified, and the potential for in vitro differentiation to osteoblastic lineage was noted. The determination of phenotypic expression was conducted by flow cytometry using aFacs Canto II with Diva® software.
Platelet-Rich Plasma Lysate
Units obtained by direct purchase, standardized process in the "Hematológica Colombiana Foundation", for direct application in regenerative tubes.
Surgical Procedure
Randomization of seven rats to each of the three groups was performed, and the groups were treated as follows: Group 1 received a 1.5-cm lesion of the sciatic nerve that was reconstructed with a nerve graft, Group 2 received a 1.5-cm lesion that was reconstructed with placement of a regenerative tube, and Group 3 received a 1.5-cm lesion that was reconstructed by placement of a regenerative tube with MSCs derived from adipose tissue and resuspended in isotonic saline solution supplemented with 10% PRP lysate (Figure 1).
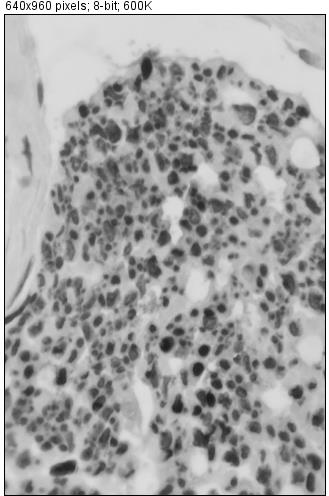
Follow-up was performed for 4 weeks, and at the end of this period, the experimental rats were euthanized according to standard procedures. The segment of the operated nerve distal to the site of the lesion was obtained. The 21 sciatic nerve explants were preserved in 10% formaldehyde, dehydrated in graduated methanol, rinsed three times with 100% xylene, and then embedded in paraffin for 24 h. Subsequently, the nerves were sliced with an American Optical microtome into 3-micron sections and stained with 1% toluidine blue after deparaffinization. The sections were observed under an Olympus DP80 microscope with a 10× objective, and sections were photographed at 40×magnification with a camera operated by Olympus Cell Sens Imaging software; photographs were evaluated offline using ImageJv1.45 software (NIH). Type Aaxons were counted, and the analysis was conducted manually and randomly by two observers who were experts in recognition of histological patterns using a double blind method [18]. From each block, three new sections of 3 microns were deparaffinized, and anti-neurofilament antibodies (Novocastra) were used for immunostaining of the axons. The axons were stained a brown color. The experiments were performed in triplicate, and data are expressed as means±standard deviations. The statistical analysis was performed with STATA 12.0 software, and a value of p<0.05 was considered statistically significant.

Results
Adipose Tissue-Derived MSCs
One line of MSCs was obtained. The cells showed adherence and fibroblast morphology in culture (Figure 2); at passage 3, the cells were cryopreserved in 12.0×106 vials at a concentration of 3.0×106 cells/mL. The ISCT criteria for MSCs were verified.

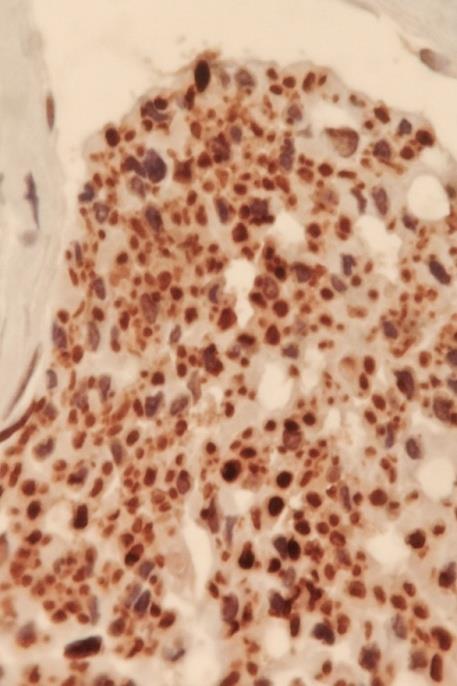
Figure 3: Immunohistochemical staining for neurofilaments. Figure 3 shows the immunophenotype obtained by flow cytometry evaluation of classical markers of MSCs as follows: CD105+, CD34-, CD73+, CD90+, and CD45-. In Figure 4, the osteogenic differentiation of MSCs after 20 days in culture is shown as part of the evaluation of the differentiation capacity of the obtained MSCs.
Regenerative Tube Preparation
The decellularized tracheas were cut to a length of 1.5 cm and a radius of 3 mm, resulting in a volume of 50 µL (V=π h r²). The cell concentration was 20×106 MSCs/mL in saline with 5% PRP lysate (Figure 5).
One of the 21rats was sacrificed due to signs of stress and lack of well-being. The rat exhibited weight loss and exudation of red hematoporphyrin around the eyes. The sacrificed rat belonged to control group (Group 1) and was replaced by another animal.
Axonal Count
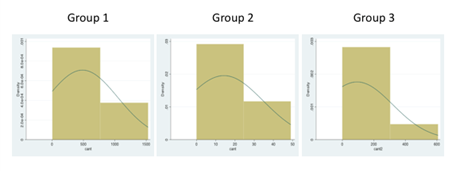
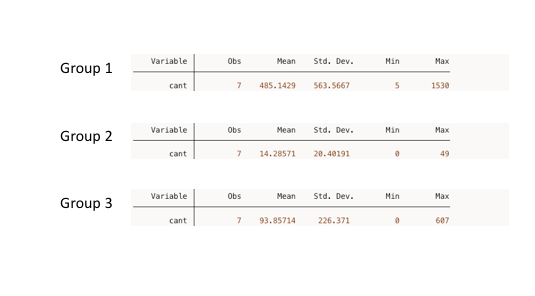
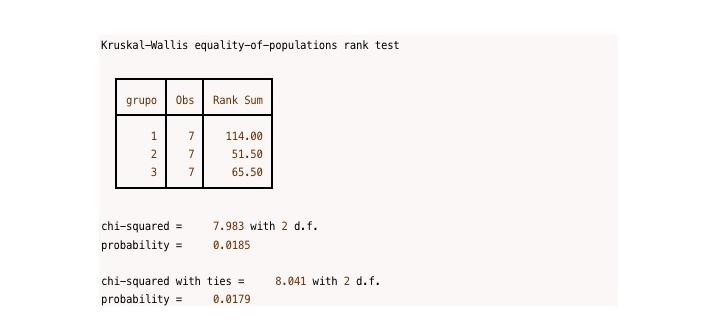
After examining the proximal and distal segments of each explant (Figure 6), 20 explants of sciatic nerves from experimental animals were processed and underwent immunohistochemical staining to detect microfilaments. Image processing and identification and quantification of myelinated axons (type A axons) were performed. Schwann cells, blood vessels with erythrocytes, small After axon counting, the percentage of regeneration was determined by dividing the total number of axons of the distal nerve by the total number of axons in the proximal nerve and multiplying by 100 [19]. Statistical analysis was performed to compare the quantitative variables among the three groups, including the count of regenerated type A axons observed under microscopy. The mean numbers of type A axons per group were as follows: Group 1 (gold standard): 485.1 SD 563.6 (5- 1530), Group 2 (negative control): 14.2 SD 20.4 (0-49), Group 3 (experimental group): 93.8 SD 226.4 (0-607).The Kruskal-Wallis test indicated a significant difference among the groups (p=0.017).

Discussion
Peripheral nerve lesions are a frequent pathology, with an estimated incidence of 13-23 cases per 100,000 people [20]. These lesions are observed in many types of clinical situations, such as sharp injuries, car accidents, motorcycle accidents, after tumor resection, congenital malformations, and gunshot wounds, and nerve injuries are difficult repair due to injuries to the adjacent soft tissues and bones.
In these cases, therapeutic intervention is required at the appropriate time using different existing techniques. Motor and sensory recovery depends on factors such as nerve type, level, and extent of the injury, patient age, comorbidities, repair technique used, and particularly, the timing of the surgical procedure. These factors affect muscular atrophy and damage to the neuromotor plate.
Current techniques for the repair of a segmental loss of a peripheral nerve are based on the interposition of tissues or materials capable of allowing the passage of the axonal growth cone to reach the distal end of the lesion and regain motor or sensory function according to the type of injured nerve. The method that has shown the best results for large defects is autologous nerve grafting, but this technique has the disadvantage that morbidity occurs in the donor area of the nerve selected to serve as a bridge between the section ends of the injured nerve. The interposition of tubes consisting of different biocompatible materials has shown good results for defects of up to 3 cm in humans. Therefore, the search for methods that allow axonal growth with the minimum possible morbidity and with the largest number of axons to the target organ of the reconstructed nerve is fundamental.
Tissue engineered nerve grafts and conduits have been extensively investigated in several experimental studies, and many novel approaches utilizing since acellular nerve grafts to bioengineered conduits have resulted in outcomes comparable to nerve autografts. Addition of Schwann cells or stem cells result in improved axonal regeneration compared with grafts nerve alone, and this can be further enhanced via gene therapy, supplemental neurotrophic factor delivery, Platelet Rich Plasma, and Chondroitinase-ABC, among others [21].
While many of these tissue engineered approaches have shown positive histological and electrophysiological outcomes, more studies emphasizing functional outcomes are needed to further assess clinical utility. This study demonstrated the potential of human adipose tissue MSCs to improve peripheral nerve regeneration after traumatic injury in a murine model, in which a biological scaffold engineered from decellularized trachea was used [22].
Many additional materials have been used as alternatives to nerve grafts for their ability to induce axonal regeneration across nerve gaps, include, acellular nerve grafts [23], pseudo nerves within silicon conduits [24], empty biodegradable collagen tubes [25], multiple channel conduits [26], biodegradable polyester tubes [27], synthetic hydrogel tubes [28], and bioidentical polysialic acid conduits [29]. Additional studies included the use of silicon tubes [30], empty Gore-Tex conduits [31, 32], alginate gels [33], polyglycolic acid tubes filled with a collagen sponge [34], and empty conduits made of arteries [35]. Most of these techniques do not induce axons to regenerate more than 1 cm, only some induce significantly longer axon regeneration, such as alginate gels, which induce axons to regenerate across gaps up to 5.0 cm in cats, and conduits composed of muscle plus muscle-vein inducing axons to regener- ate up to 5.5 cm in rats [36]. In this study we try a new natural conduit, mice descelularized trachea, with excellent resuts in consistency, ease of handling and good matching with segments of nerve to repair.
Several studies have investigated the influences of conduits containing various types of cells releasing different factors, for example, poly-epsilon-caprolactone conduits with a 3-dimensional matrix and Schwann cells plus leukemia inhibitory factor (LIF) [37], collagen tubes with Schwann cells [38], silicone tubes containing Schwann cells over expressing GDNF [39], a silk fibroin- based scaffold containing bone marrow mesenchymal stem cells (MSCs) [40], neural stem cells transfected to release glial cell line- derived neurotrophic factor (GDNF) and brain-derived neuro- trophic factor (BDNF) [41]. Other investigations have involved testing, as well as, adipose-derived mesenchymal stem cells (ASCs) which act by accelerating the growth of blood vessels and nerve by the release of BDNF [42], conduits containing neural stem cells transfected to release GDNF and BDNF [43], the administration of growth/differentiation factor-15 [44], the topical application to crushed nerves of a 26-amino- acid fragment derived from the Clostridium botulinum C3-exoenzyme [45], dissociated Schwann cells over- expressing FGF-2 [46], collagen gel containing dissociated Schwann cells [47], Schwann cells over expressing GDNF [39], Gore-Tex tubes filled with adipose-derived stem cells [48], all them induces axon regeneration not more that 3 cm, only autologous vein grafts filled with dissociated Schwann cells induce axons to regenerate longer distances more than this distance [49], therefore we believe that the combination of factors can improve said result, and our study human mesenchymal cells and platelet rich plasma.
Multiple observations in short nerve gaps become filled with PRP, show that axons regenerate across these filled gaps, with different results in increase distance axons regenerate, PRP within collagen tubes bridging rat sciatic nerve gaps [50], a slight increase in distance axons regenerate [51] and an increase in myelin thickness [52]. However, applying PRP with mesenchymal stem cells to transected nerves induces longer distances than that induced by either alone [53], one of our objectives.
The different influences of PRP, even on the same preparation, is best explained by differences in the techniques used to prepare the PRP, because they can result in PRP with considerable differences in platelet concentration and the ratio of activated to inactivated platelets, because the influences of PRP increase with the increasing concentration of inactivated platelets [54].
Therefore, to determine reliably the influences PRP can exert on axon regeneration will require using a standardization method for preparing PRP [55]. However, it will still be essential to determine whether PRP has similar effects on different preparations in the same animal model and between different animal models.
The mechanism of action of MSCs is associated their neuroprotective abilities via paracrine secretion, stimulation of cell division, retardation of the onset of apoptosis, and immunomodulatory effects. The production of neurotrophic substances [56], such as FGF, ciliary neurotrophic factor, BDNF, and GDNF, and the high levels of NGF-b, present in MSCs, improve axon regeneration and remyelination [57, 58, 59, 60, 61].
The possible role of PRP to induce nerve regeneration investigated in animal studies have shown the benefit of PRP application in peripheral nerve anastomoses, in particular in models of sciatic and facial nerve lesions. Farrag, et al. [62] have shown that PRP improved functional outcomes after facial nerve anastomosis in rats. In addition, Giannessi, et al. [63] have shown an improvement in sciatic nerve regeneration after suturing a PRP- enriched membrane at the anastomosis site. PRP may increase the thickness of the myelin sheaths and nerve fiber density through surrounding SC recruitment and angiogenesis activation.
The combination of MSCs and PRP lysate can improve axonal regeneration due to targeting by fibrin and increased quantities and numbers of growth factors present in the plasma.
While more experimental studies are needed, the continued research in the pathophysiology of peripheral nerve injury and the advances in tissue engineering techniques will one day result in a viable alternative to autografts for different lengths nerve defects.
Conclusions
This is the first experimental study worldwide to use this novel biotechnological platform to evaluate the regeneration of peripheral nerves with xenogeneic MSCs, demonstrating the usefulness and efficacy of this technique in the reconstruction of peripheral nerve lesions.The main weakness of the study is the short observation period, although if we take into account that the axonal growth in the animal model used is 3 to 5 mm / day, for the nervous defect made the time is sufficient for the axonal count in the distal to the lesion, main objective of the investigation, requiring longer periods of observation in new studies to demonstrate recovery of function and electromyographic changes.
This experimental study may facilitate new clinical studies to evaluate the effectiveness of this technique in other animal models and humans, which may generate new therapeutic options to reduce the morbidity associated with nerve reconstruction with autologous grafts.
Funding
Funding resources for this study came from research funds of the Central Military Hospital.
Conflict of Interest
The authors have no conflicts of interest to declare.
Acknowledgments
The Colombian National Institute of Health, Dr. Alejandra Muñoz Suarez and Dr.Ricardo Vanegas Romero and Basemedica SAS for their contributions in carrying out this work.
References
-
Rasulic L (2017) Current Concept in Adult Peripheral Nerve and Brachial Plexus Surgery. J Brachial Plex Peripher Nerve Inj 12(1): e7-e14.
-
Kowalska B, Sudol Szopińska I (2012) Normal and sonographic anatomy of selected peripheral nerves. Part I: Sonohistology and general principles of examination, following the example of the median nerve. J Ultrason 12(49): 120-130.
-
Dahlin LB, Wiberg M (2017) Nerve injuries of the upper extremity and hand. EFORT Open Rev 2(5): 158-170.
-
Namgung U (2014) The role of Schwann cell-axon interaction in peripheral nerve regeneration. Cells Tissues Organs 200(1): 6-12.
-
Vlot MA, Wilkens SC, Chen NC, Eberlin KR (2017) Symptomatic Neuroma Following Initial Amputation for Traumatic Digital Amputation. J Hand Surg Am 43(1): 86.e1-86.e8.
-
Carr MJ, Johnston AP (2017) Schwann cells as drivers of tissue repair and regeneration. Curr Opin Neurobiol 47: 52-57.
-
Lindsey BW, Tropepe V (2006) comparative framework for understanding the biological principles of adult neurogenesis. Prog Neurobiol 80(6): 281-307.
-
Trehan SK, Model Z, Lee SK (2016) Nerve repair and nerve grafting. Hand clin 32(2): 119-125.
-
Chiu DT, Janecka I, Krizek TJ, Wolff M, Lovelace RE (1982) Autogenous vein graft as a conduit for nerve regeneration. Surgery 91(2): 226-233.
-
Goulart CO, Fátima Rosalina PL, Zulmira Oliveira M, Severino Valentim D, Allana S, et al. (2016) Evaluation of biodegradable polymer conduits–poly (l-lactic acid)–for guiding sciatic nerve regeneration in mice. Methods 99: 28-36.
-
Gonzalez-Perez F, Cobianchi S, Heimann C, Phillips JB, Udina E, et al. (2017) Stabilization, Rolling, and Addition of Other Extracellular Matrix Proteins to Collagen Hydrogels Improve Regeneration in Chitosan Guides for Long Peripheral Nerve Gaps in Rats. Neurosurgery 80(3): 465-474.
-
Önger ME, Delibaş B, Türkmen AP, Erener E, Altunkaynak BZ, et al. (2017) The role of growth factors in nerve regeneration. Drug Discov Ther 10(6): 285-291.
-
Castelnovo LF, Bonalume V, Melfi S, Ballabio M, Colleoni D, et al. (2017) Schwann cell development, maturation and regeneration: a focus on classic and emerging intracellular signaling pathways. Neural Regen Res 12(7): 1013-1023.
-
Dominici M, Le Blanc K, Mueller I, Slaper- Cortenbach I, Marini F, et al. (2006) Minimal criteria for defining multipotent mesenchymal stromal cells. The International Society for Cellular Therapy position statement. Cytotherapy 8(4): 315-317.
-
Metcalfe AD, Ferguson MW (2007) Tissue engineering of replacement skin: the crossroads of biomaterials, wound healing, embryonic development, stem cells and regeneration. J R Soc Interface 4(14): 413-437.
-
Tondreau T, Meuleman N, Delforge A, Dejeneffe M, Leroy R, et al. (2005) Mesenchymal stem cells derived from CD133‐positive cells in mobilized peripheral blood and cord blood: proliferation, Oct4 expression, and plasticity. Stem cells 23(8): 1105- 1112.
-
Kokai LE, Rubin JP, Marra KG (2005) The potential of adipose-derived adult stem cells as a source of neuronal progenitor cells. Plast Reconstr Surg 116(5): 1453-1460.
-
Zuk PA, Zhu M, Ashjian P, De Ugarte DA, Huang JI, et al. (2002) Human adipose tissue is a source of multipotent stem cells. Mol Biol Cell 13(12): 4279- 4295.
-
Ashjian PH, Elbarbary AS, Edmonds B, DeUgarte D, Zhu M, et al. (2003) In vitro differentiation of human processed lipoaspirate cells into early neural progenitors. Plast Reconstr Surg 111(6): 1922- 1931.
-
Marquez YD, Wang MY, Liu CY (2005) Cellular signaling in neural stem cells: implications for restorative neurosurgery. Neurosurg Focus 19(3): E2.
-
Patel NP, Lyon KA, Huang JH (2018) An update– tissue engineered nerve grafts for the repair of peripheral nerve injuries. Neural Regen Res 13(5): 764-774.
-
Ohta M (2004) Implantation of neural stem cells via cerebrospinal fluid into the injured root. Neuroreport 15(8): 1249-1253.
-
Connolly SS, Yoo JJ, Abouheba M, Soker S, McDougal WS, et al. (2008) Cavernous nerve regeneration using acellular nerve grafts. World J Urol 26(4): 333-3339.
-
Zhao Q, Lundborg G, Danielsen N, Bjursten LM, Dahlin LB (1997) Nerve regeneration in apseudo- nerve'graft created in a silicone tube. Brain Res 769(1): 125-134.
-
Alluin O, Wittmann C, Marqueste T, Chabas JF, Garcia S, et al. (2009) Functional recovery after peripheral nerve injury and implantation of a collagen guide. Biomaterials 30(3): 363-373.
-
Yao L, de Ruiter GC, Wang H, Knight AM, Spinner RJ, et al. (2010) Controlling dispersion of axonal regeneration using a multichannel collagen nerve conduit. Biomaterials 31(22): 5789-5797.
-
Henry EW, Chiu TH, Nyilas E, Brushart TM, Dikkes P, et al. (1985) Nerve regeneration through biodegradable polyester tubes. Exp Neurol 90(3): 652-676.
-
Belkas JS, Munro CA, Shoichet MS, Midha R (2005) Peripheral nerve regeneration through a synthetic hydrogel nerve tube. Restor Neurol Neurosci 23(1): 19-29.
-
Haastert-Talini K, Schmitte R, Korte N, Klode D, Ratzka A, et al. (2011) Electrical stimulation accelerates axonal and functional peripheral nerve regeneration across long gaps. J Neurotrauma 28(4): 661-674.
-
Schröder JM, May R, Weis J (1993) Perineurial cells are the first to traverse gaps of peripheral nerves in silicone tubes. Clinical neurology and neurosurgery 95: 78-83.
-
Aliredjo RP, de Vries J, Menovsky T, Grotenhuis JA, Merx J (1999) The use of Gore-Tex membrane for adhesion prevention in tethered spinal cord surgery: technical case reports. Neurosurgery 44(3): 674-677.
-
Miloro M, Halkias LE, Mallery S, Travers S, Rashid RG (2002) Low-level laser effect on neural regeneration in Gore-Tex tubes. Oral Surgery, Oral Medicine, Oral Pathology and Oral Radiology 93(1): 27-34.
-
Hashimoto T, Suzuki Y, Suzuki K, Nakashima T, Tanihara M, et al. (2005) Review Peripheral nerve regeneration using non-tubular alginate gel crosslinked with covalent bonds. J Mater Sci Mater Med 16(6): 503-509.
-
Inada Y, Hosoi H, Yamashita A, Morimoto S, Tatsumi H, et al. (2007) Regeneration of peripheral nerve gaps with a polyglycolic acid-collagen tube. Neurosurgery 55(3): 640-648.
-
Anderson PN, Turmaine M (1986) Axonal regeneration through arterial grafts. J Anat 147: 73- 82.
-
Geuna S, Tos P, Battiston B, Giacobini-Robecchi MG (2004) Bridging peripheral nerve defects with muscle–vein combined guides. Neurol Res 26(2): 139-144.
-
Galla TJ, Vedecnik SV, Halbgewachs J, Steinmann S, Friedrich C, et al. (2004) Fibrin/Schwann cell matrix in poly-epsilon-caprolactone conduits enhances guided nerve regeneration. Int J Artif Organs 27(2): 127-136.
-
Stang F, Fansa H, Wolf G, Keilhoff G (2005) Collagen nerve conduits–assessment of biocompatibility and axonal regeneration. Biomed Mater Eng 15(1-2): 3- 12.
-
May F, Matiasek K, Vroemen M, Caspers C, Mrva T, et al. (2008) GDNF-transduced Schwann cell grafts enhance regeneration of erectile nerves. Eur Urol 54(5): 1179-1187.
-
Yang Y, Yuan X, Ding F, Yao D, Gu Y, et al. (2011) Repair of rat sciatic nerve gap by a silk fibroin- based scaffold added with bone marrow mesenchymal stem cells. Tissue Eng Part A 17(17- 18): 2231-2244.
-
Fu SY, Gordon T (1995) Contributing factors to poor functional recovery after delayed nerve repair: prolonged axotomy. J Neurosci 15(5): 3876-3885.
-
Lopatina T, Kalinina N, Karagyaur M, Stambolsky D, Rubina K, et al. (2011) Adipose-derived stem cells stimulate regeneration of peripheral nerves: BDNF secreted by these cells promotes nerve healing and axon growth de novo. PloS One 6(3): e17899.
-
Fu KY, Dai LG, Chiu IM, Chen JR, Hsu SH (2011) Sciatic Nerve Regeneration by Microporous Nerve Conduits Seeded With Glial Cell Line‐Derived Neurotrophic Factor or Brain‐Derived Neurotrophic Factor Gene Transfected Neural Stem Cells. Artif Organs 35(4): 363-372.
-
Mensching L, Borger AK, Wang X, Charalambous P, Unsicker K, et al. (2012) Local substitution of GDF- 15 improves axonal and sensory recovery after peripheral nerve injury. Cell Tissue Res 350(2): 225-238.
-
Huelsenbeck SC, Rohrbeck A, Handreck A, Hellmich G, Kiaei E, et al. (2012) C3 peptide promotes axonal regeneration and functional motor recovery after peripheral nerve injury. Neurotherapeutics 9(1): 185-198.
-
Haastert K, Lipokatic E, Fischer M, Timmer M, Grothe C (2006) Differentially promoted peripheral nerve regeneration by grafted Schwann cells over- expressing different FGF-2 isoforms. Neurobiol Dis 21(1): 138-153.
-
Kim DH, Connolly SE, Kline DG, Voorhies RM, Smith A, et al. (1994) Labeled Schwann cell transplants versus sural nerve grafts in nerve repair. J Neurosurg 80(2): 254-260.
-
Ghoreishian M, Rezaei M, Beni BH, Javanmard SH, Attar BM, et al. (2013) Facial nerve repair with Gore-Tex tube and adipose-derived stem cells: an animal study in dogs. J Oral Maxillofac Surg 71(3): 577-587.
-
Strauch B, Rodriguez DM, Diaz J, Yu HL, Kaplan G, et al. (2001) Autologous Schwann cells drive regeneration through a 6-cm autogenous venous nerve conduit. J Reconstr Microsurg 17(8): 589-595.
-
Piskin A, Kaplan S, Aktaş A, Ayyildiz M, Raimondo S, et al. (2009) Platelet gel does not improve peripheral nerve regeneration: an electrophysiological, stereological, and electron microscopic study. Microsurgery 29(2): 144-153.
-
Lichtenfels M, Colomé L, Sebben AD, Braga-Silva J (2013) Effect of platelet rich plasma and platelet rich fibrin on sciatic nerve regeneration in a rat model. Microsurgery 33(5): 383-390.
-
Sariguney Y, Yavuzer R, Elmas C, Yenicesu I, Bolay H, et al. (2008) Effect of platelet-rich plasma on peripheral nerve regeneration. J Reconstr Microsurg 24(3): 159-167.
-
Cho HH, Jang S, Lee SC, Jeong HS, Park JS, et al. (2010) Effect of neural‐induced mesenchymal stem cells and platelet‐rich plasma on facial nerve regeneration in an acute nerve injury model. Laryngoscope 120(5): 907-913.
-
Zheng C, Zhu Q, Liu X, Huang X, He C, et al. (2016) Effect of platelet‐rich plasma (PRP) concentration on proliferation, neurotrophic function and migration of Schwann cells in vitro. J Tissue Eng Regen Med 10(5): 428-436.
-
Sánchez M, Anitua E, Andia I (2010) Poor standardization in platelet-rich therapies hampers advancement. Arthroscopy 26(6): 725-726.
-
Avila Luz M (2008) Validación del lisado de plasma rico en plaquetas como suplemento para el crecimiento in vitro de células mensenquimales de médula ósea. Medicina Transfucional 8: 93.
-
Smith OJ, Kanapathy M, Khajuria A, Prokopenko M, Hachach-Haram N, et al. (2017) Protocol for a systematic review of the efficacy of fat grafting and platelet-rich plasma for wound healing. Syst Rev 6(1):111.
-
Bambakidis NC, Theodore N, Nakaji P, Harvey A, Sonntag VK, et al. (2005) Endogenous stem cell proliferation after central nervous system injury: Alternative therapeutic options. Neurosurg Focus 19(3): E1.
-
Tsonis PA (2007) Bridging knowledge gaps on the long road to regeneration: classical models meet stem cell manipulation and bioengineering. Mol Interv 7(5): 249-250.
-
Clavijo-Alvarez JA, Rubin JP, Bennett J, Nguyen VT, Dudas J, et al. (2006) A novel perfluoroelastomer seeded with adipose-derived stem cells for soft- tissue repair. Plast Reconstr Surg 118(5): 1132- 1142.
-
Taupin P1, Gage FH (2002) Adult neurogenesis and neural stem cells of the central nervous system in mammals. J Neurosci Res 69(6): 745-749.
-
Farrag TY, Lehar M, Verhaegen P, Carson KA, Byrne PJ (2007) Effect of platelet rich plasma and fibrin sealant on facial nerve regeneration in a rat model. Laryngoscope 117(1): 157-165.
-
Giannessi E, Coli A, Stornelli MR, Miragliotta V, Pirone A, et al. (2014) An autologously generated platelet-rich plasma suturable membrane may enhance peripheral nerve regeneration after neurorraphy in an acute injury model of sciatic nerve neurotmesis. J Reconstr Microsurg 30(9): 617-626.
- Reconstruction of Nasal Defect Using a Local Flap Based in the Nanoperforants Concept: A Case Report
- Transplant Tourism in Japan: Insights from Nationwide Surveys and Emerging Ethical Challenges
- The Challenge of Peritoneal Vaginoplasty in Transgender Women: Review Literature and Personal Perspectives
- Algorithmic Paternalism: Autonomy Versus Automation
- Dermatoscopy in Gorlin Syndrome: Avoiding the Disfigurement in Patients
- How Artificial Intelligence is Ushering in a New Era of Innovation in General and Plastic Surgery: A Short Communication