Postmastectomy Mammary Reconstruction with Musculocutaneous Flap of Latissimus Dorsi and Placement of Definitive Endoprosthesis
Introduction: The increase in the incidence of breast cancer at a global and national level, presupposes a challenge both for the surgical elimination of breast cancer and for breast reconstruction postmastectomy, as an integral part of the definitive treatment. There is an important group of techniques, within which breast reconstruction with the use of the myocutaneous flap of the Dorsal Ancho muscle is one of the most implemented. Objective: To evaluate the use of the myocutaneous flap of the Dorsal Ancho muscle in postmastectomy mammary reconstruction and definitive prosthesis placement. Material and methods: A retrospective, descriptive and longitudinal study was carried out by the Plastic Surgery Department of the Hermanos Ameijeiras Hospital in the implementation of this surgical procedure, between 2016 to 2018, 22 mastectomized patients were operated on for breast restoration using a Dorsal Ancho myocutaneous flap breast endoprosthesis placement. Results: The 22 postmastectomy patient’s predominantly infiltrating ductal carcinoma and they performed the Madden technique mostly. In more than 70% of the cases a skin island of horizontal design was planned on the muscle and complications were scarce except for the seroma in the donor area, which was observed in 63% of the cases. In general in more than 80% of the cases, results were obtained between very good and good. Conclusions: The complication rate was low, with very good results and a high degree of satisfaction of the majority of the patients, which allowed to show the utility of the application of this procedure in postmastectomy breast reconstruction.
Introduction
The importance of the breast for the quality of life of the woman is evident [1], since the breasts have always been thought of as a synonym of eroticism and femininity, for each of the women [2]. The physical and psychological trauma of mastectomy can be alleviated by breast reconstruction [1, 2].
In 2012, more than 408,000 women were diagnosed with breast cancer in America, and 92,000 died of this disease. Breast cancer in America will increase by 46% in 2030. The proportion of women who died due to breast cancer under 65 years of age is higher in Latin America and the Caribbean (57%) than in North America (41%) [1]. In Cuba there is a tendency to increase mortality due to this disease, it represents the 2nd cause of death due to neoplasia in women [2, 3, 4].
For breast reconstruction, there are different surgical procedures.
Mammary reconstruction is a surgical challenge for two fundamental aspects, such as the choice of the appropriate technique depending on the patient and the remodeling of the flap obtaining a breast as natural as possible. In 1906, Tansini [5] first described the broad dorsal musculocutaneous flap (DMF) as a resource for the coverage of mastectomy defects. However, it was not until 1977 when Schneideretal [6] described the anatomy of the flap, thus disseminating the use of the flap in breast reconstruction. The possibility of reconstructing the breast with completely autologous tissue with cutaneous characteristics very similar to the breast relegates "temporarily" the use of DMF. In 1979, Hamstroml [7] presented the first Transverse Rectus Abdominis Musculocutaneus (TRAM) for breast reconstruction. However, the problems that can occur, such as ventral hernias due to the large muscle defect, become complications that limit the use of this technique. And finally the principles introduced by Taylor [8] allowed Allen and Treece [9] to apply them to breast reconstruction by introducing the Deep Inferior Epigastric Perforator (DIEP) in 1983 with microsurgery.
The first modern descriptions of autogenous breast reconstruction were made at the end of the seventies of the last century. Brantigan [10] described in 1974 the transposition of the latissimus dorsi (latissimus dorsi) to restore the pectoralis muscle defect after radical mastectomy.
In Cuba, since 1986, at the Hermanos Ameijeiras Hospital, Dr. Martinez, Cairos and Valdivia performed mammary reconstructions with latissimus dorsi flaps, intervening surgically to more than 45 patients with this technique, obtaining satisfactory results [11].
Currently, the Dorsal Ancho Myocutaneous Flap (DAMF) is one of the most commonly used alternatives for the reconstruction of the breast using autologous tissue, having as advantages that it replaces the loss of skin and muscle in the company of a prosthesis, provides greater thoracic filling, shows a breast of natural appearance, is more reliable for its great vascularization and provides axillary filling.
Because the musculocutaneous flap of latissimus dorsi is one of the most widely used techniques for delayed reconstruction and is subject to frequent studies and modifications to achieve better aesthetic results, the motivation to carry out the present work with the purpose of improving medical behavior arose -surgical and verify that the breast reconstruction technique with DAMF, is a feasible reconstruction alternative in mastectomized patients due to breast cancer.
Material and Methods
A retrospective, descriptive and longitudinal investigation was carried out. In which, patients referred by the multidisciplinary group of mastology and oncology were evaluated to assess their reconstruction and attended the outpatient clinic of plastic surgery of the "Hermanos Ameijeiras" Hospital, with absence of unilateral or bilateral breast due to radical mastectomy by Cancer. The study was carried out from August 2016 until August 2018, where a deferred breast reconstruction technique was applied using the Dorsal Ancho Musculocutaneous Flap and Silicone stent placement. The results were evaluated, as well as the possible complications derived from this procedure during a follow-up period of up to one year after its conclusion.
Planning and Surgical Technique
The necessary and indispensable preoperative check- up was indicated by external consultation. The day before surgery, the following indications were made: Fasting from 6:00 p.m.; shave armpits; Cefazolin (1 gr) EV one hour before surgery and one hour after surgery; Diazepam (5 mg) 1 tablet V.O. 9:00 pm; Anesthesia consultation.
Operative Planning
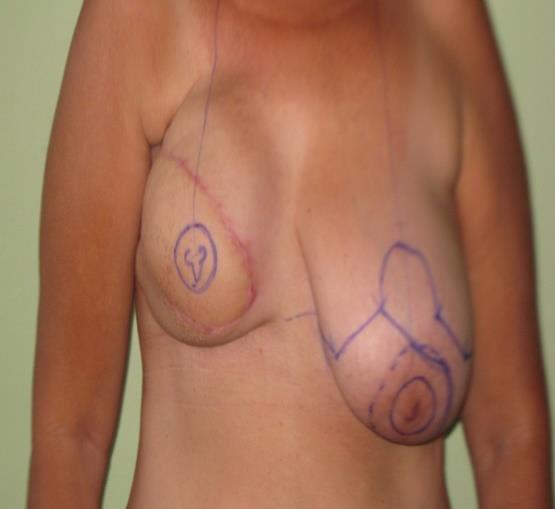
Mark the submammary groove equal to the contralateral groove. Mark the edges of the Dorsal Muscle Width according to its inserts. External: Arm in abduction and contraction for the muscle. Internal: A 1 cm from the paravertebral line from the fifth dorsal vertebra to a transverse line at the level of the two iliac crests. Superior: A line is drawn from the highest area of the posterior axillary ridge that passes below the inferior tip of the scapula to the middle vertebral line. Lower: Transverse line at the level of the two iliac crests. The island of skin is marked in elliptical form, the orientation of this can be transverse or oblique, depending on the defect to be reconstructed.
Surgical Technique 1st Time: Reconstruction of the Neomama with DAMF
Patient in lateral decubitus with arm in 90º abduction and forearm in flexion. Asepsis and antisepsis of the donor area and of the mammary region to be reconstructed. Placement of sterile fields. The cutaneous region is affected according to the design until the superficial aponeurosis of the Dorsal Ancho muscle, the extension of this plane to the limits of the muscle is performed. Disinsertion of the muscle of the lumbar fascia and the spinous processes of the dorsal vertebrae, maintaining its insertion in the humerus.
Excision of the scar of the mastectomy, skin dissection and TCS, preparation of the skin pocket for stent placement. Preparation of a transversal subaxillary tunnel and placement of the muscle with the skin island through it, up to the pectoral region. Closing of the infrascapular donor area and placement of negative suction drainage. Placement of the silicone prosthesis on the rib cage and placement of the lower edge of the skin island exactly at the level of the submammary groove, which is determined by extending the line of the intact breast groove. Covering it with the muscle and the spindle of skin. Fixation of the dorsal muscle around the prosthesis to the rib cage with non-absorbable sutures. Drainage placement in the TCS around the skin flap island. Suture of the skin island at the edges of the pectoral wound with Prolene 3.0. 2nd Stage: Reconstruction of the Nipple Areola Complex (NAC) and Contralateral Breast Plasty at 3 Months a) NAC: Reconstruction of the nipple using the stripe technique (design of 3 small flaps in the shape of a cloverleaf, the middle one is raised and the bloody face is covered by approaching the laterals. Reconstruction of the areola using graft areola against lateral if macrotelia, or using total skin graft of the inner thigh or by performing medical tattoos. b) Reducer mammary plasty: Modified Weiner technique, Robins technique, Strombeck monopediculado technique, Thorek technique, Mckissock technique. Mastopexy: Meyer, Peixoto and Pintanguy.
Postoperative Care and Follow Up
Immediate Postoperative
Parenteral hydration with Dextrose 5%; Dipyrone (600 mg) 1 IM vial every 8 hours; Gravinol (50mg) 1 IM vial if vomiting occurs; Cefazolin (1g) EV at 6:00 pm; monitor amount of bleeding through drains; Flap monitoring every 2 hours (coloring and capillary refill); 24 hours after surgery, a dry cure is made with local antiseptic and the collection of the drainage is measured; drainage is removed when the collection is less than 10 ml in 24 h; discharge on the fifth day after surgery if there are no complications; the points will be removed after 15 days.
Postoperative Period
Follow-up by external consultation was weekly until the month of surgery and then every 3 months until the year of the first surgical time. The patients continued their follow-up simultaneously by oncology consultation. The control of the cases was carried out 3 months after the first surgery, and the second time was evaluated for reconstruction of the nipple areola complex.
Results
The average age of the patients at the time of the mastectomy was 47.27 years and at the time of reconstruction of 50.95 years (range of 38-60). Most of the reconstruction was done after 4.1 years on average and 2 years as a fashion after the mastectomy.
The distribution of the patients according to the histological diagnosis showed a predominance of infiltrating ductal carcinoma in 21 patients for 86.4%. Infiltrating papillary carcinoma was diagnosed in 3 cases (13.6%). No case of medullary carcinoma was found. The distribution of patients according to the mastectomy technique resulted in 21 patients (95.5%) undergoing the Madden technique and 1 case (4.5%) using the Halsted technique.
As for the planning of the cutaneous island 15 (68.2%) were horizontal and 7 (31.8%) oblique. Different sizes of skin islands were used depending on the amplitude of the contralateral mammary base, the magnitude of the defect to be repaired and the orientation of the design. The size of the islands in the horizontal designs (17 cases) had an average of 14.8 cm long by 7.9 cm wide. The size of the island for the oblique orientation (5 cases) had an average of 19 cm long by 6.8 cm wide.

Postoperative complications occurred in 77.3%. In the donor area in 72.7% (16 cases) and in the receiving area in 13.6% (3 cases). The most frequent complication in the recipient area was partial necrosis of the flap with 9.1% (2 cases) as an immediate complication. The capsular contracture was found as mediate complication in one case for 4.5% and that same case presented hematoma as a late complication (4.5%).
The complications of the donor area that presented as mediate complications were seroma (14 cases, 63.6%) and local infection (1 patient, 4.5%), while delayed were dehiscence (2 cases, 9.1 %) and again the seroma (2 cases, 9.1%). For a total of 16 cases of seroma (72.7%), 2 cases of wound dehiscence (9.1%) and 1 case of sepsis (4.5%).
The evaluation of surgical treatment showed a predominance of good results obtained in 13 patients (59.1%), followed by very good results in 5 (22.7%), regular and poor in the same number of cases (2 patients each for 9 patients). , 1% respectively).




Discussion
Breast cancer is a major health problem that can affect women at any age, however, most of the literature consulted [3, 12]. It is more frequent between 40 and 50 years of age, which coincided with this study. Global reports indicate that infiltrating ductal carcinoma is the highest incidence within the malignant processes of the breast, which coincides with this study [12, 13].
The design and orientation of the cutaneous island, on the Dorsal Ancho muscle flap, is adapted according to the individual needs of each patient. This is determined to a large extent by the size of the defect to be reconstructed and the reliability of the flaps in the resected area, as recommended by Hammond [14].
Recently, the use of the cutaneous island along the resting tension lines of the skin was described, that is, an island in the inferolateral to superomedial sense, citing that the result is an almost imperceptible scar in the donor area. Bailey [15] (2009) performs a comparative study with the preference of patients between a horizontal and an oblique design, having as using this type of design, Hankins and Friedman [16] report that in order to perform the same it is necessary to release the muscle insertion by 90%, to rotate the pedicle and fix the cutaneous island to its new medial position.
Medium-profile circular base mammary endoprostheses with textured surface and volume between 170 and 200 ml were used. This last aspect was determined by the possibility of the Dorsal Ancho flap to cover the prosthesis, without compromising the vitality of the muscle due to the tension caused by the presence of an implant in a pocket of smaller dimensions.
Seroma was the complication that was most frequently found in the donor area, a similar aspect reported by the studies reviewed, where they indicate as means to prevent the implementation of compressive bandage, repeated long-term aspirations, insufflation of talc, fibrin sealants, suture padding and triamcinolone infiltration [17, 18].
Capsular contracture in the recipient area is the most frequent complication of the breast implant and is identified as the cause of poor aesthetic results. The risk of capsular contracture is related to two main factors, to the formation of bruises in the receiving area and to the complementary treatment with postoperative radiation, appearing as a late complication [18, 19, 20].
The study does not aim to find ideal aesthetic results, but to assess within established parameters in plastic surgery, the presence of asymmetries and deforming alterations that go against the quality of life of the patient. In more than 80% of the patients, results were obtained between very good and good, which coincides with other reports [18, 19] where, as in our research, the resulting scar in the donor area and breast symmetry are the most evaluated parameters to qualify the final result.
Conclusions
The musculocutaneous flap of the latissimus dorsi is a very safe technique, with few possibilities of tissue necrosis. Its execution is relatively fast, with very well vascularized tissues, but has the disadvantage that the skin island has a slightly different color to the rest of the skin of the anterior wall of the thorax and the sensitivity of the cutaneous island of the dorsal will be diminished or absent.
References
-
Colas C, Lozano JA, Pelay MJ (2005) Breast reconstruction through the musculocutaneous flap of the latissimus dorsi. An Sist Sanit Navar 28(2): 55-61.
-
Berrocal M (2014) Psychological sequelae of mastectomy and benefits of breast reconstruction. The four seasons of the breast. Bogota: Medical Printing.
-
PAHO (2014) Breast cancer in the Americas.
-
Ministry of Public Health. National Bureau of Statistics, Statistical Yearbook of Health. Havana, 2017.
-
Tansini I (1906) Sopra il mio nuovo proceso di amputazione della mammella. Gazeta Italiana 57: 141.
-
Schneider WJ, Hill HL Jr, Brown NG (1977) Latissimus dorsi myocutaneous flap for breast reconstruction. Br J Plast Surg 30: 277-281.
-
Holmstrom H (1979) The free abdominoplasty flap and its use in breast reconstruction. Scand J Plast Surg 13(3): 423-427.
-
Taylor R (1983) The extended Deep inferior epigastric flap: a clinical technique. Plast Reconstr Surg 72(6): 751-765.
-
Allen RJ, Treece J (1994) Deep inferior epigastric perforator flap for breast reconstruction. Ann Plast Surg 32(1): 32-38.
-
Brantigan OC (1974) Evaluation of Hutchins modification of radical mastectomy for cancer of the breast. Am Surg 40(2): 86-88.
-
Sanchez Wals L (2018) Breast reconstruction in patients with mammary pathology. Rev Cubana Cir 52(2): 154-161.
-
Park JH, Lee SK, Lee JE, Kim SW, Nam SJ, et al. (2018) Breast Cancer Epidemiology of the Working-Age Female Population Reveals Significant Implications for the South Korean Economy. J Breast Cancer 21(1): 91-95.
-
Reiner AS, Sisti J, John EM, Lynch CF, Brooks JD, et al. (2018) Breast Cancer Family History and Contralateral Breast Cancer Risk in Young Women: An Update From the Women's Environmental Cancer and Radiation Epidemiology Study. J Clin Oncol 36(15): 1513-1520.
-
Hammond DC (2007) Latissimus dorsi breast reconstruction. Clin Plast Surg 34(1): 75-82.
-
Bailey S, Saint-Cyr M, Zhang K, Mojallal A, Wong C, et al. (2010) Breast Reconstruction with the Latissimus Dorsi Flap: Women's Preference for Scar Location. Plastic Reconstructive Surg 126(2): 358-365.
-
Hankins CL, Friedman J (2008) A 7-Year Experience in Utilizing the Latissimus Dorsi Myocutaneous Flap for Bilateral Breast Reconstruction. Ann Plast Surg 60(2): 134-140.
-
Lee KT, Mun GH (2015) Fibrin Sealants and Quilting Suture for Prevention of Seroma Formation Following Latissimus Dorsi Muscle Harvest: A Systematic Review and Meta-analysis. Aesthetic Plast Surg 39(3): 399-409.
-
Shin IS, Lee DW, Lew DH (2012) Efficacy of quilting sutures and fibrin sealant together for prevention of seroma in extended latissimus dorsi flap donor sites. Arch Plast Surg 39(5): 509-513.
-
Kallaway C, Humphreys A, Laurence N, Sutton R (2016) Latissimus dorsi myocutaneous reconstruction: a study of long-term outcomes in a district general hospital. Ann R Coll Surg Engl 98(8): 574-577.
-
Zhu L, Sun Q, Liu Z, Zeng A, Jia Y, et al. (2014) Immediate breast and nipple reconstruction with the latissimus dorsi myocutaneous flap. Zhonghua Zheng Xing Wai Ke Za Zhi 30(2): 89-92.
- Reconstruction of Nasal Defect Using a Local Flap Based in the Nanoperforants Concept: A Case Report
- Transplant Tourism in Japan: Insights from Nationwide Surveys and Emerging Ethical Challenges
- The Challenge of Peritoneal Vaginoplasty in Transgender Women: Review Literature and Personal Perspectives
- Algorithmic Paternalism: Autonomy Versus Automation
- Dermatoscopy in Gorlin Syndrome: Avoiding the Disfigurement in Patients
- How Artificial Intelligence is Ushering in a New Era of Innovation in General and Plastic Surgery: A Short Communication