Laparoscopic Ascending Colon Neovagina Reconstruction for Severe Stricture of the Sigmoid Neovagina in a Transgender Woman: A Case Report
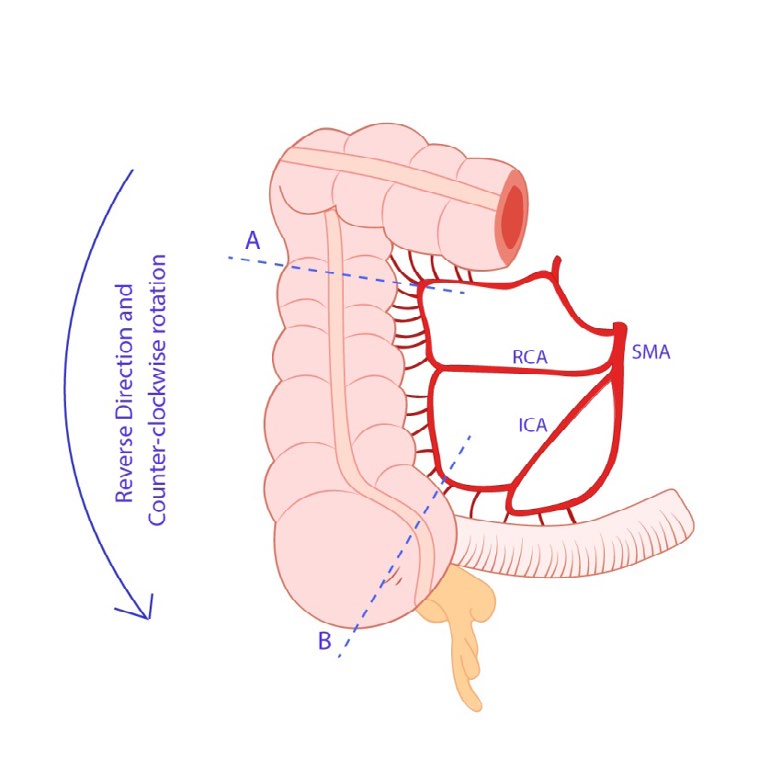
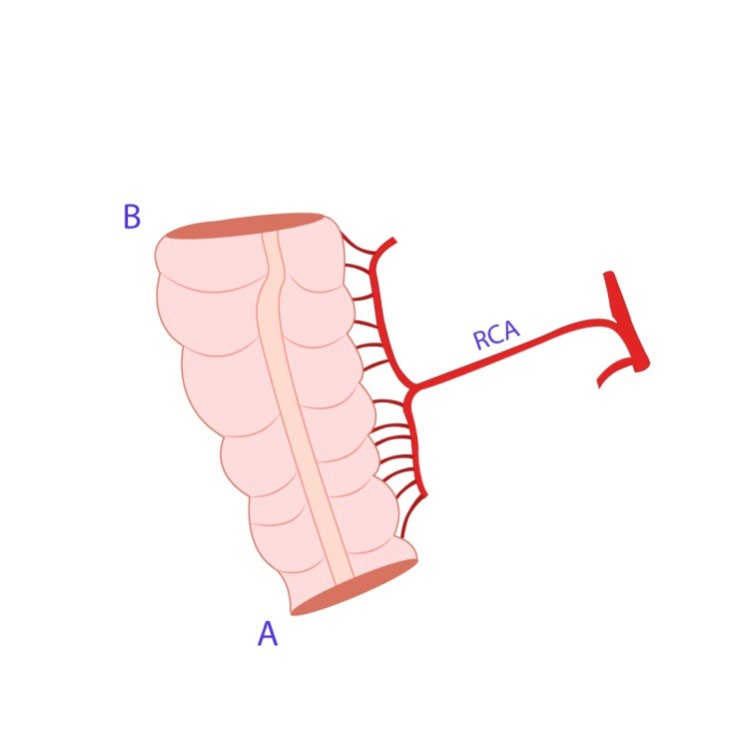
A surgical technique for neovaginal reconstruction in severe rectosigmoid vagina stricture in a trans woman has described that used laparoscopic cecum-ascending colon pedicled flap. The segment of cecum-ascending colon is based on the right colic artery, a branch of the superior mesenteric artery. The ileocecal valve is preserved; the cecum-ascending colon segment is a reverse direction and counter-clockwise rotation. This provides excellent results with adequate length. No complication was found postoperatively.
Introduction
The goal of neovaginal reconstruction in transgender women was affirmed by Karim, et al. [1], to create a perineovaginal complex as feminine in appearance and function as possible and free of poorly healed areas, scars, and neuromas. A nongenital skin graft was firstly reported in 1931 by Abraham [2]. Then, a penile skin graft was used by Fogh-Anderson in 1956 [3]. In 1957, the penile-scrotal flap was reported by Gillies and Millard [4]. Earlier, the reconstruction of genetic female genitalia in with rectum was provided by Sneguireff in 1892 [5], the first described of vaginal reconstruction with ileum was by Baldwin in 1904 [6]. Markland and Hustings reported neovagina reconstruction in transsexuals in 1974 [7, 8, 9, 10, 11, 12]. A pedicled jejunal flap for neovaginal reconstruction in the congenital absence of vagina was reported by Hung-chi Chen, et al. in 2003 [8]. Ileal vaginoplasty for transgender and non- transgender was reported by Wouter B van der Sluis, et al. in 2018 [8] as the primary and revision procedures, open and laparoscopically, a single lumen and U-pouch techniques. Nevertheless, ileal vaginoplasty was utilized for the alternative ways of neovaginal reconstruction even though excessive watery mucous. The large series of successful of cecal neovagina reconstruction in genetic female was reported by Beman R Khulpateea and David F Silver in 2014 [10]. The functional outcome was shown that the technique is a safe, uncomplicated, and viable option for neovagina reconstruction.
Surgical Technique
Under general anesthesia on lithotomy position, laparoscopic was used; the rectosigmoid vagina was excised with its pedicle and removed via the neovaginal canal. Right side colon was mobilized, the right colic artery and the ileocolic artery were identified. The cecum and ascending colon were isolated with preserved the ileocecal valve, based on the right colic artery. The appendectomy was performed. A small part of the cecum was anastomosed with the upper part of the ascending colon with staplers, the pedicled cecum-ascending colon both ends were closed with staplers. The pedicled cecum-ascending colon was then transposed to the pelvis and pull through the neovaginal canal and sutured to the penile skin part of the neovagina. The closed suction drain was placed in the perineal area.
Case Report
A 32-year old trans-woman presented with severe stricture of recto-sigmoid neovagina for 5 years. The patient underwent sex reassignment surgery (SRS) with primary sigmoid colon vaginoplasty technique 7 years ago from another hospital. She had not regulary and unproperly done vaginal dilation, developed neovaginal stricture. Since then, the neovagina became closed and be unable to do dilation for 5 years.
At first consultation and vaginal examination, the neovaginal diameter is approximately 5 mm. The neovagina introitus was attempted to surgical dilation and scar revision with Z-plasty, unfortunately, the neovaginal canal was too narrow to do postoperative manual dilation. Then the patient requested for total correction of her neovagina with another option. The request for surgical correction was accepted and the final way agreed to undergo a cecum-ascending colon substitute for neovagina.
The operation was performed on November 29, 2019, after she had tried the vaginal dilation for 7 months and eventually unsuccessful. Under general anesthesia, the patient was undergone laparoscopic cecum-ascending colon neovaginoplasty and total removal of the rectosigmoid vagina. The former rectosigmoid neovagina was removed through the neovaginal canal, the cecum-ascending colon segment base on the right colic artery was isolated, and pulled through the neovaginal canal in the reverse, anti- clockwise direction. The distal end of the cecum-ascending colon was sutured with penile skin parts of theneovagina.
The operation time was approximately 7 hours 25 minutes with none of post op complications. The patient stayed for 7 days of hospitalization, the vaginal dilation is able to resume at 14 days postoperatively with the depth of neovagina is approximately 15 cm. None of the intestinal dysfunction, and surgical wound healing went well without infection (Figures 1-4).


Discussion
Vaginal reconstruction with sigmoid segments is one of the most effective ways in non-transgender and transgender individuals as a primary or secondary neovagina reconstruction due to self-lubricated and achieved the optimal vaginal depth. Rectosigmoid colpopoiesis is commonly used for the first option to correct the primary failure of penile skin inversion or skin graft technique. Mild to moderate degree of rectosigmoid neovagina stricture can be successful with surgical dilation, this technique used to be considered in case in which other methods have failed11. Comparison to the cecum-ascending colon, the rectosigmoid is more accessible as its closed location of the native vagina and less complicated. However, after the failure of rectosigmoid vaginoplasty, almost all cases end up with their neovagina scarification. Our reason of choosing cecal-ascending colon vaginal reconstruction in this case due to its safe, reliable, and most biologic resemble the recto- sigmoid colon. The ileocecal valve was preserved to keep the physiologic intestinal function normally. Laparoscopic approached instead of transabdominal (open technique) be able to access the deep parts of the pelvic area to release the intraabdominal adhesion, and performed resection the recto-sigmoid vagina. As the cecum-ascending segment was rotate-counter clockwise, reverse direction, the mobility of the segment be able to approach the pelvis, to suture with skin parts of the residual neovagina is possible without the tension of its pedicle.
Conclusions
Cecum-ascending colon segment provided one of the alternative ways for surgical revision of severe rectosigmoid neovagina stricture in transgender women. A laparoscopic approach is reliable and the outcome has resembled to the rectosigmoid neovagina. Reverse direction and counterclockwise rotation of the segment with preserved ileocecal valve is the key to success.
References
-
Karim RB, Hage JJ, Mulder JW (1996) Neovaginoplasty in male transsexuals: Review of surgical techniques and recommendationsregarding their eligibility. Ann Plast Surg 37: 669.
-
Abraham F (1931) Genitalumwandlung an zweimannlichen Transvestiten. Sexwiss Sexpol 18: 223.
-
Fogh-Anderson P (1969) Transsexualism: An attempt at surgical management. Scand J Plast Reconstr Surg 3(1): 61-64.
-
Gillies H, Millard RD, (1957) Jr. Genitalia. In: The Principle of Art of Plastic Surgery. London: Butterworth, pp: 368- 388
-
Sneguireff WF (1904) Zwei Falle von Restitutio Vaginiae per Transplantationen. Ani Recti Zentralbl Gynakol 28: 772.
-
Baldwin JF (1904) The formation of an artificial vagina by intestinal transplantation. Ann Surg 40(3): 398-403.
-
Markland C, Hastings D (1974) Vaginal reconstruction using cecal and sigmoid bowel segments in transsexual patients. J Urol 111(2): 217-219.
-
Chen HC, Chana JS, Feng GM (2003) A New Method for Vaginal Reconstruction Using a Pedicled Jejunal Flap. Ann Plast Surg 51(4): 429-431.
-
van der Sluis WB, Pavan N, Liguori G, Bucci S, Bizic MR (2018) Ileal vaginoplasty as vaginal reconstruction in transgender women and patients with disorders of sex development: an international, multicenter, retrospective study on surgical characteristics and outcomes. BJU Int 121(6): 952-958.
-
Khulpateea BR, Silver DF (2014) A Ten year experience of cecal neovagina procedures for the restoration of sexual function on a gynecology oncology service. Gynecologic Oncology Gynecol Oncol 134(1): 150-153.
-
Djordjevic ML, Stanojevic DS, Bizic MR (2011) Rectosigmoid Vaginoplasty: Clinical Experience and Outcomes in 86 Cases. J Sex Med 8: 3487-3494.
-
Selvaggi G, Ceulemans P, De Cuypere G, VanLanduyt K, Blondeel P, et al. (2005) Gender Identity Disorder: General Overview and Surggical Treatment for Vaginoplasty in Male-to-Female Transsexuals. Plast Reconstr Surg 116(6): 135e-145e.
- Reconstruction of Nasal Defect Using a Local Flap Based in the Nanoperforants Concept: A Case Report
- Transplant Tourism in Japan: Insights from Nationwide Surveys and Emerging Ethical Challenges
- The Challenge of Peritoneal Vaginoplasty in Transgender Women: Review Literature and Personal Perspectives
- Algorithmic Paternalism: Autonomy Versus Automation
- Dermatoscopy in Gorlin Syndrome: Avoiding the Disfigurement in Patients
- How Artificial Intelligence is Ushering in a New Era of Innovation in General and Plastic Surgery: A Short Communication