Poland Syndrome: Experience in Cuba
Introduction: Breast malformations are a frequent cause of consultation in Plastic Surgery. Rarely, they are due to Poland Syndrome and are accompanied by other abnormalities that affect body self-image. Objective: To characterize patients with Poland Syndrome in Cuba. Method: A descriptive, longitudinal and prospective study was carried out with 9 patients treated at the Plastic Surgery and Caumatology Service of the Ameijeiras Hospital with a diagnosis of Poland Syndrome in the period from November 2017 to November 2020 who consented to participate. Results: 9 patients with a mean age of 27 ± 7.9 years were included. Of them, 8 were women (88.9%). According to Foulcras’ classification, 44.4% corresponded to Stage II. 55.5% had involvement of the left breast and all presented deformity of the pectoral muscle, 55.5% of them associated with deformity of the upper limb. 44.4% underwent augmentation mastoplasty and 44.4% reconstruction with tissue expansion. Only one patient did not have surgery. 33.3% underwent submuscular bilateral augmentation mastoplasty and 22.2% contralateral reduction mastoplasty. 33.3% required tissue expansion without modifying the contralateral breast, while in 11.1% it was combined with contralateral breast reduction. There were no complications. Conclusions: Poland’s Syndrome is infrequent, but it is occasionally a reason for consultation in Plastic Surgery. Surgical treatment options offer good results as long as breast reconstruction protocols are followed for deficit of the chest wall, pectoral muscles, or breast tissue.
Introduction
Plastic Surgery since its inception dealt with the treatment of body defects, whether congenital, acquired, form, function or mixed, with the intention of creating, Conceptual Paper molding or rebuilding the affected area.
The thoracic region is the seat of various deformities, especially at the mammary level, generated by pathologies such as the Poland Syndrome described for the first time in
1841 by Alfred Poland [1]. It is of unknown cause, although some authors associate it with a vascular alteration at the mesoderm level that generates a primary defect of the proximal clavicular artery causing a deficit of blood flow at the level of the pectoral region that gives rise to a partial decrease in tissue in This region [2, 3].
It has an incidence of 1/20000, has no hereditary predisposition and occurs in a higher proportion in men than in women with a 3: 1 ratio. 1 However, more women than men consult for this disease in the Plastic Surgery services.
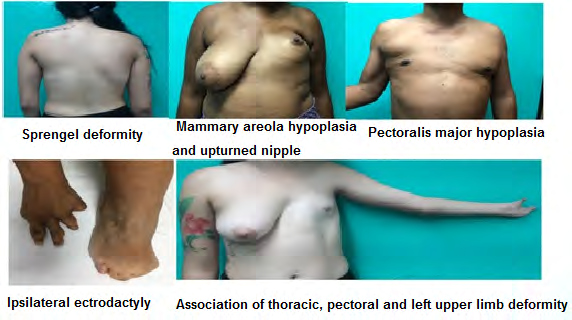
Its clinical presentation is variable with different degrees of extension and severity. It is currently defined as the association of hypoplasia or unilateral absence of the pectoralis major muscle with alterations of the ipsilateral upper limb accompanied by syndactyly, brachydactyly or oligodactyly with usual normality of the thumb [4]. At the musculoskeletal level, it can be associated with the absence of the serratus, latissimus dorsi, deltoid muscles and the sternocostal portion of the pectoralis minor muscle, which causes the Sprengel deformity or scapular elevation [5]. At the mammary level there is amastia or hypomastia, hypoplasia of the mammary areola and the nipple that is deviated upwards [5, 6]. At the osteoarticular level, patients may present agenesis of the second to fifth costal arch causing asymmetric contralateral pectum carinatum, hemivertebrae, scoliosis, agenesis or hypoplasia of the radius, ulna, carpal bones, metacarpus and phalanges [7, 8].
Other associated abnormalities are absence of axillary hair, apocrine sweat glands and armpit pterygium, pulmonary hernia, dextrocardia, interventricular septum defects, renal aplasia, hypospadias, ectopic testes, inguinal hernia and in rare cases leukemia’s, multiple hemangiomas, syndrome by Möebius, Goldenhar and Adams-Oliver [6]. It is the only malformation with an exclusively unilateral appearance affecting the right side in 70% of cases [6].
The classifications for its diagnosis are multiple to evaluate the intensity of the affectation, which provide guidance on the severity and prognosis of the patients. Among them are Al-Qattam classification [9] based on the anatomical characteristics of the hands dividing it into seven types and Foulcras classification [10] based on three stages that considers alterations at the muscular, mammary and thoracic region. Finally, there is a classification that takes into account clinical and radiological criteria, classifying it from mild to very severe according to the breast, musculoskeletal changes of the thorax, ipsilateral upper limb and association of other congenital abnormalities [11].
The cases that come to the Plastic Surgery consultation of the Hermanos Ameijeiras Clinical Surgical Hospital are not carriers of alterations of the rib cage because due to their connotation in development they are treated in pediatric age, the most striking thing in adult patients is the affectation at the level of the breast and the extremities. The mammary region is an erogenous zone par excellence that this disease affects with asymmetry and disorder of body self-image. This expresses the idea of the importance of knowing the surgical options to offer the best aesthetic result in women who suffer from it.
The diagnosis is usually clinical, but it is confirmed with complementary studies such as ultrasound, computerized axial tomography or nuclear magnetic resonance to confirm the absence of muscle structures [12].
This syndrome has more aesthetic than functional involvement in adult patients, so from the therapeutic point of view the goal is to improve the external appearance and body self-image with a minimum of sequelae. Taking into account the rarity of this syndrome and its disfiguring nature of breast development in women, this study is carried out with the objective of characterizing patients with Poland Syndrome in Cuba.
Method
A descriptive, longitudinal and prospective study was carried out in 9 patients treated at the Plastic Surgery and Caumatology Service of the Hermanos Ameijeiras Clinical Surgical Hospital with the diagnosis of Poland Syndrome, in the period from November 2017 to November 2020. Included patients older than 18 years of age, without distinction of sex. Those patients who did not consent to participate in the study and those who did not attend follow-up visits were excluded.
The variables were studied: Age: in completed years.
Sex: female, male.
Al-Qattan Classification: • Type 1: Normal hand (isolated pectoral anomaly).
• Type 2: Hand appears smaller, when compared with the contralateral side.
• Type 3: Classic deformity (brachysindactalia).
3a: Mild to moderate hypoplasia of the hand.
3b: Severe hypoplasia of the hand.
• Type 4: Some functional rays still present:
4a: Floating or absent thumb.
4b: Adactyly of the index.
4c: Adactyly of the index and long fingers.
4d: Adactyly of the central rays creating a cleft hand.
4e: Adactyly of the ulnar rays.
• Type 5: All fingers are not working or are absent.
• Type 6: Transverse deficiency proximal to the metacarpophalangeal joints.
• Type 7: Phocomelia-type deficiency [9].
Foulcras Classification
• Stage I: Mild malformation with pectoralis major muscle hypoplasia and moderate mammary hypoplasia. There is a slight thoracic asymmetry in men and mild to moderate breast asymmetry in women.
• Stage II: Moderate malformation with pectoralis major aplasia, significant breast asymmetry in women, with or without associated moderate rib malformation. There is a marked asymmetry of the thorax.
• Stage III: Severe malformation with complete muscular and mammary aplasia, other associated muscular aplasias, and significant costo-sternal malformation [10].
Surgical techniques used in the treatment of Poland Syndrome 1. Augmentation mastoplasty: Increase in breast volume with implant placement or by lipotransfer.
2. Reconstruction with tissue expansion: Expand the coverage of the breast tissue with progressive insufflation of an expansive saline prosthesis to create the pocket space for the definitive implant.
3. Contralateral reduction mastoplasty: Surgical reduction of excess breast tissue to achieve contralateral symmetry.
Complications: Categorized in presence or absence during follow-up.
Techniques and procedures Information collection: The information sources were the interview and the clinical examination. With prior consent to participation, the surgical intervention was carried out according to the characteristics of each case. The patients were evaluated one week, one month and every 3 months until one year after the surgery.
Information processing and analysis: The data obtained were collected in a Microsoft Excel database and processed using the SPSS statistical package, version 23.0. Age was summarized as mean and standard deviation, minimum and maximum. The variables measured on a qualitative scale were summarized in absolute and relative frequencies (percentages). The results were presented in tables.
The research was approved and approved by the Scientific Council and by the Medical Ethics Commission of the institution. It was carried out in accordance with current national principles of medical ethics and the principles of the Declaration of Helsinki.
Results
Nine patients with a mean age of 27 ± 7.9 years were included. Of them, 8 were women (88.9%) with a minimum age of 19 years and a maximum of 30. Table 1 presents the Al-Qattan classification. 44.4% of the cases presented anatomical characteristics of the Type 1 hands and 33.3% Type 2. It should be noted that the reported type 7 case presented ectrodactyly.
| Al-Qattan Classification | N0. | % |
|---|---|---|
| Type 1 | 4 | 44.4 |
| Type 2 | 3 | 33.3 |
| Type 6 | 1 | 11.01 |
| Type 7 | 1 | 11.01 |
| Total | 9 | 100 |
Table 1: Distribution of patients according to the Al-Qattan classification.
Most of the cases were classified in Stage II (4 patients; 44.4%), according to Foulcras’ classification (Table 2).
| Calculation De Foulcras | NO. | % |
|---|---|---|
| Stage I | 3 | 33.3 |
| Stage II | 4 | 44.4 |
| Stage III | 2 | 22.02 |
| Total | 9 | 100 |
Table 2: Distribution of patients accordding to Foulcras classification.
55.6% of the patients had involvement of the left breast and 44.4% of the right breast. 100% of the patients presented deformity of the pectoralis muscle and in 55.5% they were associated with deformity of the upper limb (Figure 1).
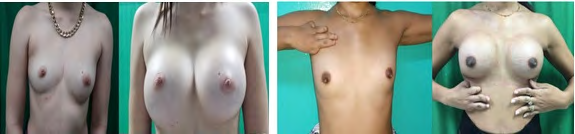
The surgical techniques used are shown in Table 3. There was a patient who did not undergo any surgical procedure. The 8 operated cases were all women. Of these, 44.4% underwent augmentation mastoplasty and a similar proportion required reconstruction with tissue expansion due to tissue deficit. 33.3% of the patients underwent submuscular bilateral augmentation mastoplasty, correcting the difference in volume with implants of different sizes (Figure 2), while 22.2% underwent contralateral reduction mastoplasty. 33.3% of the patients required tissue expansion on the affected side without modifying the contralateral breast and only one patient (11.1%) was combined with contralateral breast reduction. No complications were reported.
| Surgical Techniques | Affected breast | Contralateral Breast | Total | |||
|---|---|---|---|---|---|---|
| No. | % | NO. | % | NO. | % | |
| Augmentation mastoplasty | 4 | 44.4 | 3 | 3.33 | 4 | 44.4 |
| Reconstruction with tissue expansion | 4 | 44.4 | 0 | 0 | 4 | 44.4 |
| Reduction mastoplasty | 0 | 0 | 2 | 22.2 | 2 | 22.2 |
| None | 1 | 11.1 | 4 | 44.4 | 1 | 11.1 |
Table 3: Distribution of patients according to surgical techniques. *Percentahe calculated based on the total number of patients
Discussion
In the literature, frequent case presentations with Poland Syndrome in pediatric age are reported. Breast involvement within the Poland sequence is a reason for consultation in Plastic Surgery services [13]. In the present study, most of the patients were in their third decade of life, which is why the psychological impact of the aesthetic defect is greater, as stated in the study by Guliana Martinez [14]. Poland Syndrome is described more frequently in men than in women, but in our study the female sex prevails, which is consistent with Almanzar’s research [1]. A higher incidence of female patients is observed in the Plastic Surgery consultation with the aim of solving the alterations presented at the level of the mammary region. Most of the patients had left Poland Syndrome, which is consistent with the literature, but differs from Villalon’s study [15].
One of the alterations that Poland Syndrome usually presents is dextrocardia, which in our study occurred in one of the patients, similar to Perez Diaz’s research [16]. The different forms of presentation of the syndrome require different forms of surgical treatment. In the simplest cases, the augmentation mastoplasty with endoprosthesis or lipograft applied in the hypoplastic breast is enough to obtain good symmetry, adequate submammary groove, good infraclavicular filling and good location of the areolomamillary complex. In more complex cases, more complex reconstructive techniques such as tissue expansion and subsequent augmentation mastoplasty with implant in hypoplastic breast with the presence of pectoralis major should be used. Other surgical techniques in hypoplastic breast and absence of the pectoralis would be breast reconstruction with a major dorsal musculocutaneous flap, Transverse Rectus Abdominals or microvascularized free flaps.
For the reconstruction of the chest wall with unilateral chest depression with risk of progression, lack of protection of the lung or heart, paradoxical movement of the chest wall or cosmetic defect secondary to the absence of pectoralis major in men, reconstruction or bone stabilization using bone grafts or prosthetic meshes, closure of the muscle defect by transposition of flaps and of the breast defect with implants. In other cases, a reduction or mastopexy of the contralateral breast is necessary to achieve adequate symmetry [15]. For the reconstruction of the chest wall with unilateral chest depression with risk of progression, lack of protection of the lung or heart, paradoxical movement of the chest wall or cosmetic defect secondary to the absence of pectoralis major in men, reconstruction or bone stabilization using bone grafts or prosthetic meshes, closure of the muscle defect by transposition of flaps and of the breast defect with implants. In other cases, a reduction or mastopexy of the contralateral breast is necessary to achieve adequate symmetry.
For the reconstruction of the chest wall with unilateral chest depression with risk of progression, lack of protection of the lung or heart, paradoxical movement of the chest wall or cosmetic defect secondary to the absence of pectoralis major in men, reconstruction or bone stabilization using bone grafts or prosthetic meshes, closure of the muscle defect by transposition of flaps and of the breast defect with implants. In other cases, a reduction or mastopexy of the contralateral breast is necessary to achieve adequate symmetry [15]. None of the cases described presented serious chest wall defects, so it was not necessary to perform more complex surgical procedures.
Conclusions
Breast dysmorphia present in Poland syndrome is uncommon, but it is a reason for occasional consultation in Plastic Surgery. Surgical treatment options offer good results as long as breast reconstruction protocols are followed for deficit of the chest wall, pectoral muscles, or breast tissue.
References
-
Almanzar R (2019) Poland anomaly, regarding two cases. Science and health 3(3): 65-68.
-
Marmesat MA, Cabal GA (2020) Poland syndrome: About a case. Semergen 46(1): 7-8.
-
Gonda K, Tachiya Y, Hatakeyama Y, Momma T, Tamaoki T, et al. (2018) Poland syndrome accompanied by internal iliac artery supply disruption sequence: a case report. Journal of Medical Case Reports 12: 312.
-
Catano JC, Restrepo S (2019) Poland syndrome: unilateral hypoplastic pectorals major with brachydactyly. Postgrad Med J Epub 95(1129).
-
Nurettin Y, Turgut I, Öksüz S (2015) Clinical analysis of 113 patients with Poland syndrome. Ann Thorac Surg 99(3): 999-1004.
-
Sierra SL, Gonzalez Rodriguez MP (2008) Poland syndrome: description of two patients in the same family. Annals of Pediatrics 69(1): 49-51.
-
Olagorta S, Esteban E (2011) Poland syndrome: musculoskeletal deformity, anesthetic and surgical management. Rev Chil Anest 40: 354-356.
-
Safvet O (2017) Incidence and Classification of Chest Wall Deformities in Breast Augmentation Patients. Aesthetic Plast Surg 41(6):1280-1290.
-
Vazquez J, Aguirre J, Garcia G, Aguirre M (2018) Clinical Case: Complete vs Incomplete Poland Syndrome, Surgical Resolution. Rev Med HJCA 10(1): 56-63.
-
Garcia Verastegui LS, Motta Ramirez GA (2015) Poland syndrome. Medical Journal 6(3): 231-232.
-
Teran CG, Antezana AN (2018) Poland syndrome: description of a case in the delivery room. Gac Med Bol 41(1): 64-66.
-
Melendez NF, Monroy S, Serrano MS, de Nubila LE (2015) Imaging of Poland Syndrome: Case Report. Rev. Colomb. Radiol 26(2): 4220-4222.
-
Manzano SM, Parri F, Tarrado X (2019) Poland Sequence: Retrospective Analysis of 66 Cases. Ann Plast Surg 82(5): 499-511.
-
Martinez Guaicha GP, Apolo Abrigo M, Calva Ochoa KJ, Jumbo Cuenca AA, Galarza Sanchez CA, et al. (2019) A 22-year-old female patient with unilateral hypoplasia of the muscles belonging to the pectoral region. On the subject of a case in patient. Loja, Ecuador. Ocronos.
-
Villalon E, Garces M, Diaz A, Villafranca J, Grez E, et al.(2003) Surgical techniques for breast reconstruction in Poland syndrome. Chilean Rev. of Surgery 55(1): 86- 91.
-
Perez Diaz JM (2017) Dextrocardia, atelia, hypoplasia and pectoral hypotrichosis: diagnosis in the elderly of a rare congenital anomaly. Rev Esp Casos Clin Med Intern 2(3): 119-121.
- Reconstruction of Nasal Defect Using a Local Flap Based in the Nanoperforants Concept: A Case Report
- Transplant Tourism in Japan: Insights from Nationwide Surveys and Emerging Ethical Challenges
- The Challenge of Peritoneal Vaginoplasty in Transgender Women: Review Literature and Personal Perspectives
- Algorithmic Paternalism: Autonomy Versus Automation
- Dermatoscopy in Gorlin Syndrome: Avoiding the Disfigurement in Patients
- How Artificial Intelligence is Ushering in a New Era of Innovation in General and Plastic Surgery: A Short Communication