Steroid Withdrawal in Pediatric Kidney Recipients: Is it Safe?
Introduction: In the last decades, immunosuppressive therapy for pediatric kidney recipients has changed dramatically. Early steroid withdrawal, being one of these, has shown comparable outcomes on graft function and survival compared to steroidbased regimens. Less is known about the possible negative effects of this regimen. The aim of this study was to evaluate the safety of the steroid-sparing TWIST regimen in pediatric kidney recipients. Design: Data were collected among pediatric kidney transplant recipients during the first five years of follow-up in a single center. Documented data included immunosuppressive protocols, infections, hypertension, diabetes, anemia, leucopenia, candiduria, growth retardation, gastrointestinal complaints, nephrotoxicity, lymphoma and rejection. Occurrence of these effects was compared between patients that started on a steroid-sparing regimen and those starting on a steroid-containing regimen using an intention to treat analysis with censoring at the moment of switching. Results: Out of 100 recipients, 44 patients started the steroid-sparing regimen immediately after transplant surgery. Twenty (45%) of these remained on this regimen during whole follow-up period. Patients on a steroid-based regimen had significantly more urinary tract infections, cmv infections and rejections than those on a steroid-sparing regimen. Other side effects did not differ between the groups. Conclusion: Steroid-sparing immunosuppressive therapy regimen is preferable and safe in pediatric kidney transplant recipients without additional potential risk factors and is accompanied with less opportunistic infections.
Loes Oomen1*, Liesbeth L de Wall1, Elisabeth AM Cornelissen2, Wout FJ Feitz1 and Charlotte MHHT Bootsma-Robroeks2
Introduction
Pediatric kidney transplantation is the treatment of choice for children with end-stage renal disease (ESRD). It significantly improves survival, growth and health-related quality of life compared to dialysis [1]. In the Netherlands, approximately 30 pediatric kidney transplants are performed yearly.
In the last decades, overall graft survival has significantly improved, among others due to changes in both type of immunosuppressive medication and regimens. Large variabilities still exist between various immunosuppressive therapy regimens, centers and countries [2].
Pediatric protocols are mainly based on data of adult transplant care. However, pediatric metabolism involves different age and weight, - drug processing capacity and calculated doses and requires adjusted immunosuppression [3]. Because of the relatively small numbers of pediatric recipients compared to adult kidney recipients, adequate powered randomized controlled trials are currently missing. As a result, little is known of the effects of different immunosuppressive regimens used in this specific population. Since the TWIST (Transplant WIthout STeroids) study in 2010, steroid withdrawal has been preferred by most centers [2].
Previous literature suggests steroid-sparing regimens to result in better growth [4], but also cause an increased risk for Epstein Barr virus (EBV) infection and post-transplant lymphopr1oliferative disorder (PTLD) [5]. The goal remains to find the best combination of immunosuppressive agents in order to optimizes graft survival and function. A balance between preventing rejection while limiting side effects can be challenging.
The aim of this study was to evaluate the safety of the steroid-sparing TWIST regimen in pediatric kidney recipients. In addition this study examines the occurrence of side effects and infections with regard to the immunosuppressive regimens.
Method
Design
A retrospective single center cohort study was conducted. Our pediatric kidney transplant recipients, actively under control during the last five years, were reviewed. After obtaining informed consent, medical records of these patients were analyzed for a maximum of five-year post-transplant or until graft loss. Transplantations were performed between 2002 and 2018. Patients with numerous missing data or those who received their kidney transplant elsewhere were excluded.
Data Collection
Uses of immunosuppressive drugs over time were documented, including type of medication, documented side effects, moment and reason for switching medication. The following parameters were studied: patient demographics, type of donation, previous therapy, age of donor and recipient, placement of the graft, ischemia time, peri- operative parameters, height standard deviation score (SDS), number of episodes of CMV, EBV and BKV infection, number of culture proven urinary tract infections (UTIs), occurrence of side effects of the different regimens: hypertension, diabetes, anemia, leucopenia, candiduria, growth retardation, gastrointestinal complaints, nephrotoxicity, PTLD and acute rejection [6]. Based on protocol, CMV prophylaxis in high‐ risk patients (CMV serostatus Donor+ Recipient−) consisted of valganciclovir during three months post-transplant. All recipients received uro-prophylaxis, by means of trimethoprim, during the first three months after transplant.
In our nation, pneumocystis pneumonia (PCP) prophylaxis is not standard protocol because of the low incidence in this region.
Basiliximab was given as induction therapy in all patients. Before 2012, maintenance therapy consisted of three immunosuppressive agents including prednisone (TRIPLE). In 2012, the steroid-sparing TWIST protocol was introduced for all patients, except those who were highly sensitized or had glomerular kidney disease with high risk of recurrence [7]. The TWIST protocol limits steroid-use to the first five days after transplant. Immunosuppressive treatment was according to the protocol active at the moment of transplant and personalized on clinical course. In the analysis, difference between TWIST and TRIPLE regimen only consist in the use of prednisone.
Height‐SDS was calculated and compared pre‐ and post‐transplant. The pretransplant data were collected a few weeks before transplant, and the post‐transplant values were documented yearly during the study period of five years of follow‐up.
Rejection was defined as a biopsy‐proven acute rejection using the Banff classification [8]. UTI was defined as urine culture demonstrating the presence of >50 000 colony forming units/mL of a single pathogen in combination with clinical symptoms and fever [9].
CMV and EBV infections were defined as more than 250 copies/ml in plasma CMV/EBV viremia by PCR testing at any moment during follow-up [10]. BKV replication was quantified using real-time quantitative PCR assay using BKV specific primers [11]. Surveillance CMV, EBV, and BKV blood viral loads were obtained at a minimum of every three months during the first year and thereafter once a year scheduled according to protocol. Children were monitored for any clinical symptoms and additional viral testing was performed at the discretion of the treating physician. In order to determine whether there was a primo-infection or a reactivation, CMV and EBV serology was tested, at least yearly.
Data Analysis
Data were analyzed using SPSS statistics 25.0. Descriptive statistics were used to describe the baseline demographics and the frequency of occurrence of independent and dependent variables, including the mean, median, standard deviation and percentage. Maintenance on initial therapy was analyzed using Kaplan-Maier curves. Differences between groups were analyzed using chi-square tests, independent T-tests and Mann Whitney U test for data that were not distributed normally. Data were analyzed using an intention to treat method with censoring at the moment of regimen switch. Differences were considered statistically significant at p <0.05.
were excluded because of numerous missing data, loss of follow-up or transplants in other hospitals. The demographic characteristics are shown in Table 1. Median donor age was 42 years and ranged between 5 and 69 years. Patients intentional treated according the TWIST protocol received more often a graft from a living donor and had more pre- emptive and first transplantations. Follow-up was longer in the TRIPLE group.
- Results
- Demographic Characteristics
- In total, 108 patients were reviewed. Eight patients
- TWIST
- (N=44)
- TRIPLE
- (N=56)
- Male: Female
- 27:17
- 30:26
- 57:43
- 0.23
- Age at transplantation (years) [range]
- 8.0 [2, 18]
- 7.5 [1, 16]
- 8.0 [1, 18]
- 0.45
- Follow-up (months) [range]
- 18 [0, 60]
- 45 [3, 63]
- 47 [3, 64]
- <0.01*
- Donor type % (n)
- Deceased donor
- 16% (7)
- 41% (23)
- 30% (30)
- 0.02*
- Heart-beating donor
- 14% (6)
- 32% (18)
- 24% (24)
- Non heart-beating donor
- 2% (1)
- 9% (5)
- 6% (6)
- Living donor
- 84% (37)
- 59% (33)
- 70% (70)
- First transplant: Second transplant
- 44:00
- 48:08
- 92:08
- 0.01*
- Pre-emptive: Dialysis prior to transplant
- 23:21
- 19:37
- 42:58
- 0.05
- Retro-peritoneal: Intra-abdominal placement
- 28:16
- 49:07
- 77:23
- 0.05
Table 1: Patient characteristics.
Use of Immunosuppressants
In the past, standard immunosuppressive regimens included prednisolone, mycophenolate (MMF) and cyclosporine. In 2012, a steroid-sparing regimen (TWIST) was introduced. Over time, a decline in use of prednisone, cyclosporine and MMF was seen, whereas use of tacrolimus increased.
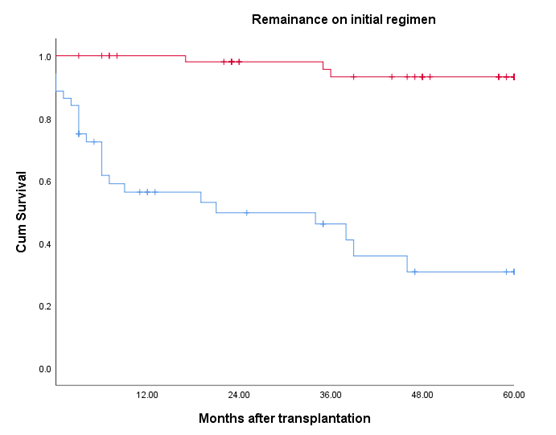
Since the introduction in 2012, 44 out of 67 patients started with the TWIST regimen, directly after transplantation. During follow-up, 45% (20) remained on this regimen (Figure 1). Switches between regimen occurred mainly in the first year after transplantation. After two years half of the patients that started steroid-free were still on TWIST regimen. In our cohort of 100 recipients, 51 patients (33 were transplanted before 2012) remained on the TRIPLE regimen during follow-up, 5 stopped using prednisone. In total 29 patients switched regimens during follow-up. Main reasons for switching regimens were gastro-intestinal complaints, nephrotoxicity, infection and bone marrow depression (Table 2). Most common TRIPLE regimens were prednisone/MMF/Tacrolimus (after rejection), prednisone/ azathioprine/tacrolimus (after intestinal complaints), prednisone/tacrolimus (high infection pressure).
In total, 69% of the patients did switch medication during follow-up. The main reasons for changing medication dosage and/or regimen were gastrointestinal side effects (23%) and viremia of EBV of BK (23% and 17%, respectively).
| Switch (N=29) | |
| Male: Female | 16:13 |
| Age at transplantation (years) [range] | 8 [2,17] |
| Follow-up (months) [range] | 36 [3,64] |
| Donor type % (n) |
Table 2: Characteristics of the switch group. Median [range]. BKV: BK- virus, EBV: Epstein-Barr virus, HLA: human leukocyte antig
| Deceased donor | 28% (8) |
|---|---|
| Heart-beating donor | 28% (8) |
| Non heart-beating donor | |
| Living donor | 72% (21) |
| Total mismatches | 3 [0, 5] |
| HLA-DR mismatches | |
| 0 | 31% (9) |
| 1 | 66% (19) |
| 2 | 3% (1) |
| First transplant: Second transplant | 28:01 |
| Pre-emptive: Dialysis prior to transplant | 13:16 |
| Retro-peritoneal: Intra-abdominal placement | 21:08 |
| Reason for switch % (n) | |
| Gastro-intestinal complaints | 21% (6) |
| Bone marrow depression | 7% (2) |
| Nephrotoxicity | 21% (6) |
| Rejection | 21% (6) |
| BKV or EBV infection | 21% (6) |
| Other | 10% (3) |
Table 3: Characteristics of the switch group. Median [range]. BKV: BK- virus, EBV: Epstein-Barr virus, HLA: human leukocyte antig
Side Effects by Initial Immunosuppressive Regimen
Patients that started on a TRIPLE regimen had more UTI (p< 0.01) overall, more UTI’s in the first year (p=0.04) and more often recurrent UTI’s (p=0.02) (Table 3). In this group there was a significant higher incidence of CMV primo infection (p=0.03), whereas there was no difference in use of CMV prophylaxis.
No differences were seen in occurrence of gastrointestinal complaints, nephrotoxicity, lymphoma (PTLD). Nor did groups did differ in hypertension, diabetes, anemia, leucopenia and candiduria (Table 3). PCP did not occur in these patients.
Biopsy proven rejection was found in 10 patients of which 6 did switch regimen during follow up. Switching took place when those patients had already switched to the TRIPLE regimen. Rejection was not a reason for switching. No rejection occurred in the TWIST group, which was significant less than in TRIPLE group (p=0.02). Donor specific antibodies were found in 3 patients (1 had class I antibodies, 2 had class II antibodies).
| TWIST N =44 | TRIPLE N =56 | p -value | |
|---|---|---|---|
| Opportunistic infections | |||
| UTI | |||
| UTI during follow-up | 25% | 63% | <0.01* |
| UTI during first year | 18% | 46% | 0.04 |
| Recurrent (2 or more) | 14% | 41% | 0.02* |
| Candiduria | 2% | 4% | 0.59 |
| CMV | |||
| Primo infection | 0% | 11% | 0.03* |
| Re-activation | 7% | 5% | 0.54 |
| CMV prophylaxis | 59% | 64% | 0.54 |
| BKV | |||
| BKV viremia | 14% | 9% | 0.33 |
| EBV | |||
| Primo infection | 14% | 14% | 0.58 |
| Re-activation | 9% | 14% | 0.32 |
| PTLD | 2% | 4% | 0.59 |
| Other side effects | |||
| Need of antihypertensives | 96% | 100% | 0.57 |
| Bone marrow depression | |||
| Anemia (need of erythropoietin) | 46% | 30% | 0.09 |
| Leucopenia (leucocytes <3.0 *109/L) | 5% | 2% | 0.41 |
| Diabetes | |||
| Need of antidiabetics | 7% | 9% | 0.5 |
| HbA1c (mmol/mol) [range] | 35 [23, 41] | 46 [20, 49] | 0.87 |
| Height | |||
| ≤ -2.5 SDS at transplant | 16% | 14% | 0.52 |
| ≤ -2.5 SDS at end of follow-up | 14% | 27% | 0.09 |
| Δ SDS height per year [range] | -0.02 [-2.0, 1.3] | -0.06 [-4.1, 1.0] | 0.83 |
| Nephrotoxicity | 12% | 20% | 0.41 |
| Biopsy proven acute rejection | 0% | 18% | 0.02* |
| Gastrointestinal complaints | 18% | 20% | 0.53 |
Table 4: Occurrence of opportunistic infections and side effects during follow-up for different immunosuppressive regimens. Media
Table 3: Occurrence of opportunistic infections and side effects during follow-up for different immunosuppressive regimens. Median [range]. BKV: BK- virus, CMV: cytomegalovirus, EBV: Epstein-Barr virus, HBA1c: Hemoglobin A1c, PTLD: post-transplant lymphoproliferative disease, SDS: standard deviation score, TRIPLE: steroid containing regimen, TWIST: transplantation without steroids, UTI: urinary tract infection, * p <0.05.
Graft Function Over Time
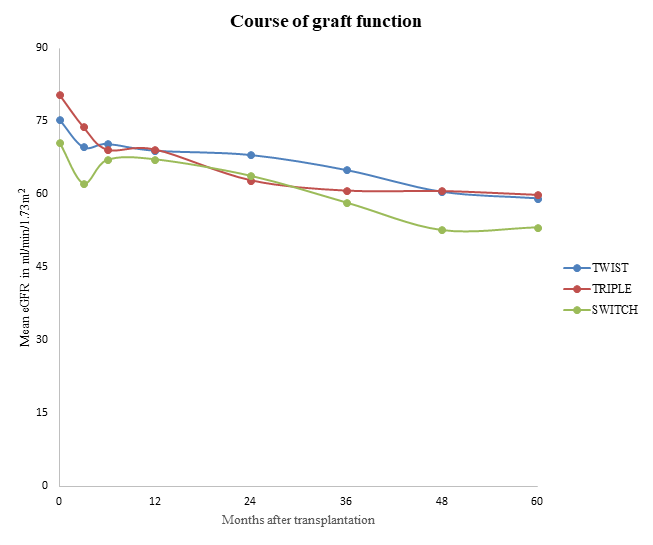
Figure 2 depicts graft function over time for the different medication regimens. Graft function decreases equally in all groups.
Opportunistic infections
In our cohort of 100 patients, CMV-, BK- and EBV-viremia was diagnosed in 14, 11 and 24 children, respectively. Co- infection of CMV + EBV or EBV+ BK was seen in five children, co-infection of CMV + BK in two recipients. UTIs occurred in 55 patients of which 41 (75%) had an UTI in the first year and 37 (67%) having 2 or more UTI’s. Infections occurred mainly in the first year.
Discussion
Immunosuppressive protocols used in pediatric kidney transplant have changed substantially over time in order to improve patient and graft survival in kidney recipients and reduce adverse effects [2]. This study revealed a 50% decrease in prolonged prednisone use after introduction of TWIST (steroid-sparing regimen) in 2012. During the follow- up, 45% of the patients who started with a steroid-sparing regimen, remained on this protocol. In our cohort, starting a steroid-sparing protocol was possible safe, resulting in less side effects and rejection without risk for loss of graft function. Opportunistic infections occurred mainly during the first year after kidney transplant and more often in the steroid-based TRIPLE regimen.
Immunosuppressive Regimen
Half of the patients starting on a steroid-sparing regimen remained steroid free during follow-up. Switching regimen was mostly due to a combination of complaints, caused by immunosuppressants. Main reasons to switch immunosuppressive agents were consistent with literature on gastro-intestinal complaints following mycophenolate mofetil use and tacrolimus nephrotoxicity [12, 13]. Additionally, occurrence of infection led to switches in immunosuppressants. The regimen that was used after switching depended on the cause of switching, as we practice personalized medicine
Efficacy
Graft function seems to be comparable between groups, supporting the hypotheses that starting on a TWIST regimen does not endanger the graft function, whereas it result in less side effects. However, groups were too small to draw conclusions on these data.
In our study, acute rejection occurred significantly more in patients starting on a TRIPLE regimen. Even more, there was no rejection in the TWIST group. This doesn’t meet the expectations of TRIPLE being a more potent regimen and might be caused by the differences in follow-up period between the groups and the differences in deceased and living donors. Additionally, patients starting on a TWIST had a relatively better starting position because patients at high risk for recurrence of rejection would start with TRIPLE. However, these results show that starting on a TWIST regimen does not lead to increased rejection.
Opportunistic Infections
Immunosuppressive therapy interferes with the individual balance between virus replication and the immune response which might result in viremia. Children on an immunosuppressive regimen are prone for CMV, EBV and BKV infections [14]. These infections remain a significant cause of morbidity and mortality following kidney transplantation [14]. They can impair graft survival, patient survival and quality of life through multiple hospitalizations [15].
Viral infections were mainly present in the first year after transplant, which has been reported by other studies a well [14]. Without viral prophylaxis, infection is most likely to occur in the early months after transplant because of transmission trough the donor kidney and potentiated immunosuppression during this period [16]. With the use of prophylaxis, the onset of CMV disease usually occurs after the cessation of prophylaxis [16, 17, 18]. According to literature, the incidence of viral infections after kidney transplant ranges between 10% and 30% for CMV infection, 9 to 67% for EBV infection, and 7% and 10% for BKV viremia [17, 18, 19]. This study supports these results with an incidence of 14%, 24% and 11% for respectively CMV, EBV and BKV.
Consistent with findings in the adult population, a steroid-sparing regimen was not associated with an increase in CMV infections [20]. Even more, patients that started on a TRIPLE regimen had more urinary tract infections and primo cmv infections regardless of prophylaxis. This is in consistence with earlier studies in adults, showing a decrease in CMV infections after steroid withdrawal [20, 21] and might be due to a diminished suppression of the native immune system.
Little is known about the effect of steroid-sparing regimen on UTI in children. This study showed that patients on a steroid-sparing regimen had significant less UTI’s compared to those on a steroid-based regimen, which is consistent with literature in adults [22].
Uro-prophylaxis is standard care in the first three months after transplantation for all patients. Prolongation to 6 or 12 months might be considered given the fact that 43% of all UTI’s occur in months 4 to 12 after transplantation.
Consistent with findings in the adult population, a steroid-sparing regimen was not associated with an increase in EBV or BKV infections [18, 20, 23, 24]. No difference between both regimens was found. In contrast to other studies no association could be found in PTLD occurrence [5, 25]. This probably due to the relative short time of follow- up for malignancies to develop and low patient numbers. Previous studies hypothesized that avoiding corticosteroids leads to an increase in PTLD because of the intensification of other immunosuppressive drugs. In our centre, target values are comparable between TWIST and TRIPLE regimens.
Growth
In concordance to the 130-subject SNS01 RCT of Sarwall, et al. steroid withdrawal was not was not associated with improved growth velocity [4]. This in contrast to previous literature studies [2]. This might be explained by the wide recipient age range in this study, the majority of prepubertal patients or the limited follow-up, as a catch-up growth might be expected later.
The limited follow-up might as well explain the fact that we found no differences in the incidence of diabetes mellitus. We do expect a steroid withdrawing regimen to decrease the risk on diabetes on a later age [26, 27, 28].
Limitations
These data must be interpreted with caution since the analyzed groups were not identical. After 2012 the patients who received TWIST, had a better starting position because the patients that were highly sensitized or at risk for recurrence of the native disease were excluded from TWIST and treated with TRIPLE. Before 2012 however, all patients received the same therapy and patient characteristics did not differ between groups. When analyses were conducted only on patients transplanted after 2012, results do not differ from those currently shown (data not shown).
Previous literature supports the idea that starting with steroid avoidance might even be safe in high-risk patients [29]. Differences found might also be biased by the use of other immunosuppressive medication, since the use of these was personalized. Retrospective data collection was a limitation of this study, as was a follow-up period of only five years after kidney transplant. Patients on TRIPLE regimen had significantly longer follow-up periods which might bias the results.
The present study provides an analysis of a relatively large cohort of pediatric patients with well-documented long- term post-transplant follow-up in a single center. It provides new insight in the use and switches in immunosuppressive medication over time.
Conclusion
Based on the presented data, we conclude the TWIST protocol to be safe in pediatric kidney recipients. Introduction of a steroid-sparing regimen was not associated to an increase in rejection or other feared side effects. Steroid withdrawal was associated with less opportunistic infections. In addition, efficacy was similar to steroid-based immunosuppressive regimens. Therefore, we recommend considering this protocol for patients without additional potential risk factors, e.g. highly sensitized patients or high chance of recurrence of disease in the kidney.
References
-
Van Arendonk KJ, Boyarsky BJ, Orandi BJ, James NT, Smith JM, et al. (2014) National trends over 25 years in pediatric kidney transplant outcomes. Pediatrics 133(4): 594-601.
-
Pape L (2019) State-of-the-art immunosuppression protocols for pediatric renal transplant recipients. Pediatric Nephrology 34(2): 187-194.
-
Verghese PS (2017) Pediatric kidney transplantation: a historical review. Pediatric research 81(1-2): 259-264.
-
Webb NJ, Douglas SE, Rajai A, Roberts SA, Grenda R, et al. (2015) Corticosteroid-free Kidney Transplantation Improves Growth: 2-Year Follow-up of the TWIST Randomized Controlled Trial. Transplantation 99(6): 1178-1185.
-
McDonald RA, Smith JM, Ho M, Lindblad R, Ikle D, et al. (2008) Incidence of PTLD in pediatric renal transplant recipients receiving basiliximab, calcineurin inhibitor, sirolimus and steroids. Am J Transplant 8(5): 984-989.
-
Ponticelli C (2011) Present and future of immunosuppressive therapy in kidney transplantation. Transplant Proc 43(6): 2439-2440.
-
Nehus E, Liu C, Hooper DK, Macaluso M, Kim MO (2015) Clinical Practice of Steroid Avoidance in Pediatric Kidney Transplantation. Am J Transplant 15(8): 2203-2210.
-
Roufosse C, Simmonds N, Clahsen-van Groningen M, Haas M, Henriksen KJ, et al. (2018) A 2018 Reference Guide to the Banff Classification of Renal Allograft Pathology. Transplantation 102(11): 1795-1814.
-
Becknell B, Schober M, Korbel L, Spencer JD (2015) The diagnosis, evaluation and treatment of acute and recurrent pediatric urinary tract infections. Expert review of anti-infective therapy 13(1): 81-90.
-
Meerbach A, Wutzler P, Hafer R, Zintl F, Gruhn B (2008) Monitoring of Epstein-Barr virus load after hematopoietic stem cell transplantation for early intervention in post- transplant lymphoproliferative disease. J Med Virol 80(3): 441-454.
-
Ding R, Medeiros M, Dadhania D, Muthukumar T, Kracker D, et al. (2002) Noninvasive diagnosis of BK virus nephritis by measurement of messenger RNA for BK virus VP1 in urine. Transplantation 74(7): 987-994.
-
Bentata Y (2020) Tacrolimus: 20 years of use in adult kidney transplantation. What we should know about its nephrotoxicity. Artif Organs 44(2): 140-152.
-
Hardinger KL, Brennan DC, Lowell J, Schnitzler MA (2004) Long-term outcome of gastrointestinal complications in renal transplant patients treated with mycophenolate mofetil. Transpl Int 17(10): 609-616.
-
Scaggs Huang FA, Danziger-Isakov L (2019) Infectious disease risks in pediatric renal transplantation. Pediatric Nephrology 34(7): 1155-1166.
-
Hogan J, Pietrement C, Sellier-Leclerc AL, Louillet F, Salomon R, et al. (2017) Infection-related hospitalizations after kidney transplantation in children: incidence, risk factors, and cost. Pediatric Nephrology 32(12): 2331- 2341.
-
Green M, Avery RK, Preiksaitis J (2004) Guidelines for the prevention and management of infectious complications of solid organ transplantation.
-
Weikert BC, Blumberg EA (2008) Viral infection after renal transplantation: surveillance and management. Clin J Am Soc Nephrol 3(2): S76-S86.
-
Randhawa P, Brennan DC (2006) BK virus infection in transplant recipients: an overview and update. Am J Transplant 6(9): 2000-2005.
-
Aloufi M, Alzahrany G, Abdulmajeed N, Alzahrani S, Alghwery S, et al. (2019) Viral Infections After Kidney Transplantation in a Cohort of Children: A Retrospective Single-Center Study. Transplant Proc 51(2): 522-525.
-
Matas AJ, Kandaswamy R, Gillingham KJ, McHugh L, Ibrahim H, et al. (2005) Prednisone-free maintenance immunosuppression-a 5-year experience. American journal of transplantation. Am J Transplant 5(10): 2473- 2478.
-
Axelrod D, Leventhal JR, Gallon LG, Parker MA, Kaufman DB (2005) Reduction of CMV Disease with Steroid-Free Immunosuppresssion in Simultaneous Pancreas–Kidney Transplant Recipients. Am J Transplant 5(6): 1423-1429.
-
Tan JY, Zhao N, Wu TX, Yang KH, Zhang JD, et al. (2006) Steroid Withdrawal Increases Risk of Acute Rejection but Reduces Infection: A Meta-Analysis of 1681 Cases in Renal Transplantation. Transplant Proc 38(7): 2054- 2056.
-
Hirsch HH, Brennan DC, Drachenberg CB, Ginevri F, Gordon J, et al. (2005) Polyomavirus-associated nephropathy in renal transplantation: interdisciplinary analyses and recommendations. Transplantation 79(10): 1277-1286.
-
Knight RJ, Gaber LW, Patel SJ, DeVos JM, Moore LW, et al. (2013) Screening for BK viremia reduces but does not eliminate the risk of BK nephropathy: a single-center retrospective analysis. Transplantation 95(7): 949-954.
-
Opelz G, Dohler B (2004) Lymphomas after solid organ transplantation: a collaborative transplant study report. Am J Transplant 4(2): 222-230.
-
Garro R, Warshaw B, Felner E (2015) New-onset diabetes after kidney transplant in children. Pediatric nephrology (Berlin, Germany) 30(3): 405-416.
-
Mourad G, Glyda M, Albano L, Viklický O, Merville P, et al. (2017) Incidence of Posttransplantation Diabetes Mellitus in De Novo Kidney Transplant Recipients Receiving Prolonged-Release Tacrolimus-Based Immunosuppression With 2 Different Corticosteroid Minimization Strategies: ADVANCE, A Randomized Controlled Trial. Transplantation 101(8): 1924-1934.
-
Song TR, Jiang YM, Liu JP, Wang ZL, Zeng J, et al. (2019) Steroid withdrawal or avoidance is safe in high-risk kidney transplants: A systematic review and meta- analysis. Kaohsiung J Med Sci 35(6): 350-357.
-
Nehus EJ, Liu C, Lu B, Macaluso M, Kim MO (2017) Graft survival of pediatric kidney transplant recipients selected for de novo steroid avoidance-a propensity score-matched study. Nephrol Dial Transplant 32(8): 1424-1431.
- Reconstruction of Nasal Defect Using a Local Flap Based in the Nanoperforants Concept: A Case Report
- Transplant Tourism in Japan: Insights from Nationwide Surveys and Emerging Ethical Challenges
- The Challenge of Peritoneal Vaginoplasty in Transgender Women: Review Literature and Personal Perspectives
- Algorithmic Paternalism: Autonomy Versus Automation
- Dermatoscopy in Gorlin Syndrome: Avoiding the Disfigurement in Patients
- How Artificial Intelligence is Ushering in a New Era of Innovation in General and Plastic Surgery: A Short Communication