An Overlooked Diagnosis: Orbital Emphysema
Introduction
Orbital Emphysema, is known as the presence of air in the periorbital soft tissues [1]. In part of maxillofacial traumas, fractures in the orbital bone may result in the entry of air into the orbit. Orbital emphysema caused by orbital fractures usually occur as a result of falls, assault,sport or motor vehicle accidents. Furthermore, infections secondary to gas producing microorganisms, pulmonary barotraumas, airplane trips, intubation barotraumas, frontal sinus osteomas, as well as iatrogenic causes all contribute to the development of orbital emphysema [2, 3]. The most common cause of orbital emphysema according to the literature is paranasal sinus and orbital medial wall fractures especially if followed by valsalva maneuveres such as nose blowing and sneezing [2]. In most cases, orbital emphysema tends to be self limiting, where it resolves without the need for acute surgical intervention. Despite being a rare finding, orbital emphysema may have serious complications such as loss of vision. In periorbital traumas, pathologies such as severe proptosis, exophtalmus ischemic optic neuropathy and retinal artery occlusion may require emergent surgical intervention [2, 3].
The diagnosis and hence treatment of orbital fractures is mainly based upon the clinical presentation and radiological investigations. The presence of orbital emphysema and the localisation of the air is most accurately identified by computerised tomography (CT). Herein, we present a case of orbital emphysema and its progress.
A 29- year-old female patient was admitted to the Emergency Department of our institute after being abused and battered by her husband.Since the emergency department could not give an exact diagnosis to explain her symptoms, the patient was consulted to us in order to evaluate her maxillofacial trauma. The patient started complaining of swelling in the eyelids and tenderness in the eyeball. Her examination revealed right periorbital palpebral oedema and ecchymosis periorbital subcutaneous crepitus, mild proptosis, minimal visual compromise 3 hours following the incident. There was no resctriction of the eye movement except minimal downward gaze limitation. Direct and indirect light reflex were positive, exophthalmus was absent as the patient did not complain of diplopia. In the period of observation following episodes of sniffing and crying increased the swelling and limitation in eye movements with respect to the initial examination was noticed, which raised the suspicion of orbital emphysema.
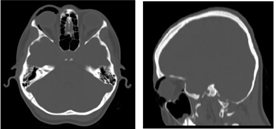
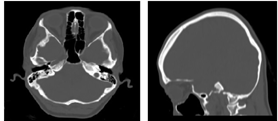
In CT scan, non- displaced fractures in the medial wall and floor of the right orbit without any herniation of the extraocular muscle or tissue was detected (Figure 1). Blow-out fracture was excluded. Air density in the right superior orbital margin were detected, which confirmed our diagnosis. Admission and inpatient follow-up in the Plastic, Reconstructive and Aesthetic Surgery clinics was adviced. However, the patient signed out against medical advice, hence pulse steroid treatment was given in the emergency department. Oral antibiotics, nasal decongestant and anti- inflamatory steroids 1mg/kg prednol were prescribed, absolute avoidance of valsalva pressure boosting maneuvers was recommended. No surgical intervention was performed. On 3rd month follow up showed full recovery and the patient’s mild downgaze restriction was totally resolved as CT scan revealed full recovery (Figure 2). Written informed consent was obtained from patients who participated in this study.
Discussion
Orbital Emphysema, is usually an overlooked clinical diagnosis in trauma patients due to its non-urgency. Orbital emphysema was first classified by Heerfordt in 1904 and according to Heerfordt Classification, orbital emphysema is classified into three types [2, 4]. Type 1 which describes palpebral or preseptal emphysema which is charactarised by intact orbital septum and subcutaneous air which is confined solely to the eyelids, isolated palpebral emphysema is rarely seen, it may be secondary to lacrimal bone fracture or lacrimal sac rupture. Air flow from the nose to the nasolacrimal drainage system may enter into the upper eyelid. As long as the orbital septum is intact the emphysema will be limited to the eyelids. Type 2 describes true orbital emphysema which occurs due to fracture of the orbita and laceration of the mucosa with accumulation of air in the air behind the intact septum. These fractures are usually seen in the ethmoidal bone and in the relatively weak lamina papyracea. Less often, frontal, maxillary and sphenoid sinus fractures may lead to orbital emphysema indirectly by the intermittent infiltration of air due to the increase in pressure in the upper airways due to nose blowing and sneezing [4]. Type 3 describes orbitopalpebral emphysema which develops as air accumulates in the orbit, the increase in the intraorbital pressure may lead to the rupture of the orbital septum ( palpebral fascia) consequently the air is allowed to traverse from the orbit into the eyelids.
Clinical signs and symptoms associated with orbital emphysema include orbital pain, hyposthesia, limited eye movement, exophthalmus or endophthalmus, diplopia, and loss of vision [1]. The most prominant finding in palpebral and orbitopalpebral emphysema is eyelid swelling, air in the subconjunctival plane may be seen as well. In most cases crepitation can be palpated. If emphysema is limited to the posterior chamber crepitation in the eyelids may be felt by the application of minimal pressure to the eyeball. In cases where the orbital septum is not intact, proptosis maybe mild or absent as air may spread into the eyelids. Occular motility may be limited in cases of severe exophthalmus and increased orbital pressure. Orbital emphysema may have serious complications such as loss of vision, exophthalmus, increase in intraorbital pressure, and retinal artery occlusion [2, 5]. The pressure of the orbital septum can range by 40-50 mm Hg, however, these levels might be lower in the elderly population. Since central retinal artery can oclude and irreversible retinal injury begins above the pressure of 65 to 70 mm, retrobulbar orbital emphysema can necessitate urgent intervention [6]. There is still no clear consensus in the literature on the management of cases of orbital emphysema. Mild to moderate cases can be followed-up without treatment. However, in the presence of anxiety, respiratory distress, severe pain and if infection is suspected the patient must be hospitalised for follow-up. In the case of progression of the symptoms, or if orbital compartment syndrome is suspected, urgent decompression is necessary and can be performed by canthotomy, cantholysis or by needle aspiration. Entrapment of soft tissue may stimulate strong vagal response, nausea, vomiting, bradychardia, heart block and syncope may be seen in oculocardiac response. In such conditions, the entrapped tissue must be released and the orbital wall must be repaired. Conservative treatment can generally be applied in cases with minimal diplopia, preserved ocular motility and no obvious enophtalmus or proptosis. On discharge the patients must be warned about the valsalva maneuvers that may increase the intraorbital pressure and be advised to avoid these actions including sneezing, coughing, vomiting or blowing air through the nose [4]. There is no sufficient clinical research about the significance of antibiotherapy in orbital emphysema. Recently, antibiotics use has been recommended in patients with orbital emphysema associated with sinus fractures [7].
To conclude, orbital emphysema should be considered in the differential diagnosis when extraocular muscle entrapment is excluded, in the presence of linear fracture, or in the presence of inexpicable ocular signs and symptoms. It should be kept in mind that conservative treatment option is sufficient in a patient with isolated orbital oedema and tenderness due to fractures in the medial and inferior orbital walls whereas an overlooked serious orbital emphysema may worsen and even lead to blindness.
References
-
Roelofs KA, Starks V, Yoon MK (2019) Orbital Emphysema: A Case Report and Comprehensive Review of the Literature. Ophthalmic Plast Reconstr Surg 35(1): 1-6.
-
Ariyoshi Y, Naito H, Yumoto T, Iida A, Yamamoto H, et al. (2019) Orbital Emphysema as a Consequence of Forceful Nose-Blowing: Report of a Case. Case Rep Emerg Med 2019: 4383086.
-
Wang H, An J (2019) Orbital Emphysema After Repair of Orbital Fracture. J Craniofac Surg 30(7): e687-e688.
-
Myers S, Bell D (2018) Orbital blowout fracture from nose blowing. BMJ Case Rep 2018:bcr2018224633.
-
Miki K, Orita Y, Kumase F, Sugaya A, Hirai M, et al. (2011) Orbital emphysema causing syncope. Acta Med Okayama 65(1): 55-76.
-
Dong QN, Ide T, Karino M, Okuma S, Koike T, et al. (2019) Retrobulbar Orbital Emphysema Associated With Medial Orbital Wall Fracture. J Craniofac Surg 30(5): 1549-1551.
-
Aslan F, Öktem C (2020) Clinical and radiological features of traumatic orbital emphysema cases. Acta Med. Alanya 4(2): 122-125.
- Reconstruction of Nasal Defect Using a Local Flap Based in the Nanoperforants Concept: A Case Report
- Transplant Tourism in Japan: Insights from Nationwide Surveys and Emerging Ethical Challenges
- The Challenge of Peritoneal Vaginoplasty in Transgender Women: Review Literature and Personal Perspectives
- Algorithmic Paternalism: Autonomy Versus Automation
- Dermatoscopy in Gorlin Syndrome: Avoiding the Disfigurement in Patients
- How Artificial Intelligence is Ushering in a New Era of Innovation in General and Plastic Surgery: A Short Communication