Open Method for Surgical Removal of Modeling Substance in a Patient with Iatrogenic Gluteal Allogenosis
Introduction: Surgical removal of modeling substances is the treatment of choice in iatrogenic allogenosis. This is a disease caused by the injection of substances misnamed “biopolymers” with high antigenicity and low histocompatibility. Symptoms can be local or general, leading to a systemic inflammatory autoimmune syndrome induced by adjuvants. Method: A patient operated by open method for the surgical extraction of allogenic substances in the gluteal region is described. Results: A 46-year-old female patient with a history of injection of more than 1000 ml of liquid silicone in both buttocks and face 11 years ago is presented. Two years later, she presented erythema, increased consistency, pruritus, and hyperemia, associated with general symptoms that limited her daily activities. She was diagnosed with an adjuvant-induced systemic inflammatory autoimmune syndrome and was admitted for surgical removal of the causative agent. Surgical extraction of alloplastic material in the gluteal region was performed for the first time in Cuba without local postoperative complications. Conclusion: Surgical treatment by the open biopolymer extraction method is deforming, but it is the only solution to improve the symptoms of iatrogenic allogenosis.
Introduction
The need of human beings to improve their body self- image quickly, effectively and without scars leads them to search for facial or body fillers with modeling substances misnamed “biopolymers” consulting with unsuitable or unqualified personnel [1]. The use of these substances gives rise to the appearance of the term “modeling disease” also known as “adjuvant disease” or Iatrogenic Allogenosis described for the first time in 2008 by Coiffman F [2] that refers to the appearance of various manifestations adverse effects on the human body, caused by the use of foreign substances at the hands of health personnel [1, 2]. The most widely used biopolymer is silicone which, once injected, produces a fibrohistiocytic cell reaction, with recruitment of giant cells, which is related to the migration of the product to a distance [3] generating an autoimmune response and complications that can occur immediately, minutes or hours after the procedure both local and systemic. Within the local manifestations are granulomatous reactions to the foreign body, migration of the product to other parts of the body, fistulas, fibrosis, multiple inflammatory processes and infection. Systemic complications include autoimmune or connective tissue diseases and inflammatory processes that lead to necrosis of organic structures [4]. It is an incurable disease, whose solution is prevention and once established, only the extraction of the modeling product improves the symptoms [5]. This surgical treatment in turn constitutes a risk of secondary deformity and death. The first patient operated by the open method of biopolymer extraction in the gluteal region in Cuba is presented with the aim of showing the results of the extraction by the open method.
Case Report
A 46-year-old female patient with a history of injection of more than 1000 ml of liquid silicone in both buttocks and face, 11 years ago. Two years later, she presented erythema, increased consistency, pruritus, and hyperemia, associated with general symptoms that limited her daily activities. Her buttocks increased in size and the symptoms radiated to the lower limbs. The clinical manifestations were exacerbated with increased pain in the sacral area at the time of defecation, inability to walk and remain upright, loss of approximately 20 kg of weight in one month, and pathological fractures. She was diagnosed with adjuvant-induced systemic inflammatory autoimmune syndrome (SIAS) [1] and was admitted for surgical removal of the causative agent.
Interrogation
- General condition: Asthenia, weight loss.
- Skin and subcutaneous cellular tissue: Itching, discoloration, dryness and scaling on the buttocks.
- Digestive system: Gastroesophageal reflux, heartburn, colic, nausea, constipation alternated with diarrhea, epigastric pain, anorexia and heartburn.
- Osteomyoarticular system: Arthralgia, myalgias and difficulty walking related to deformity caused by modeling substance. Nervous system: Paresthesias in the lower extremities, fasciculations and involuntary movements.
Physical Exam
Gluteal region with hyperpigmented skin with stiff hypopigmentations areas, peeling and indurations, associated with erosion and inflammatory changes. Fibrosis cords distributed from the intergluteal line to the lumbar region and the lower limbs, associated with congestive inguinal lymphadenopathies (Figure 1).
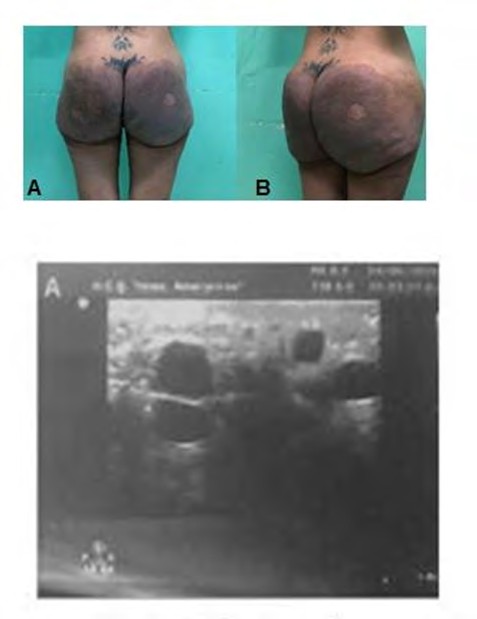
Figure1: Preoperative period. A: Rear view. B: Side view.
Complementary Exams
Laboratory: Leukocytes 16.9 10^9/L, hemoglobin 86 G/L, hematocrit 0.270 L/L, platelets 489 10^9/L, erythrocyte sedimentation rate 45 mm/h, creatinine 432 umol/L. Leukocytosis and increased erythrocyte sedimentation rate were related to the immune response to the allogenic substance. Anemia and elevated creatinine were a response to chronic renal failure secondary to interstitial nephritis due to the deposition of alloplastics substances.
Imaging Tests: Soft tissue ultrasound of the buttocks: Multiple cystic images at the subcutaneous cellular tissue level that do not exceed 2 cm in diameter. The allogenic substance is distributed throughout the subcutaneous cellular tissue at the gluteal level, forming caverns with oily content inside (Figure 2A).
A. Ultrasound Figure 2A: Imaging studies of the gluteal region.
Magnetic Resonance Imaging of the buttocks: hyperdense artifact images that distort the anatomy of the subcutaneous cellular tissue located in the gluteal region (Figure 2B).
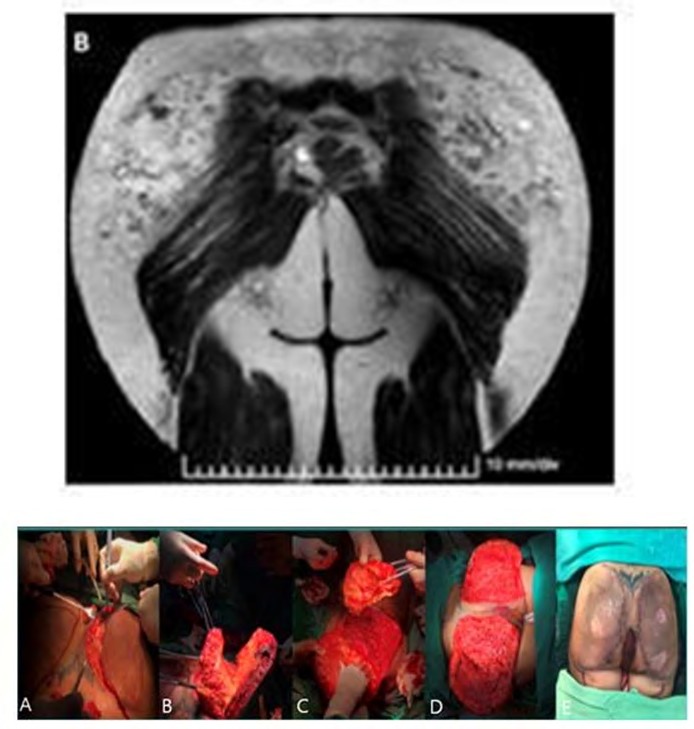
B: Magnetic nuclear response. Figure 2B: Imaging studies of the gluteal region.
Diagnosis
Iatrogenic allogenosis in the buttocks.
Treatment
Surgical.
Preoperative Preparation
Red cell transfusions to improve hemoglobin levels, prophylactic antibiotics, evacuating enemas, adequate nutrition rich in proteins and vitamins, and a reduction in steroid doses, in order to guarantee adequate evolution and healing of surgical wounds and flaps. In addition, there was the assessment of a multidisciplinary team made up of nephrology, rheumatology and psychiatry.
Surgical Technique
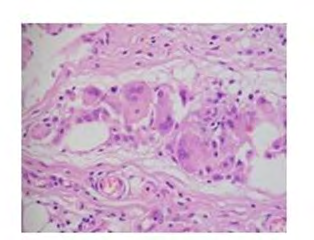
Under general orotracheal anesthesia, patient in prone position after asepsis and antisepsis placement of sterile fields, an extended skin incision was made in the internal contour of the gluteus, it was dissected at the level of the supra-aponeurotic plane and part of the product was extracted, respecting one centimeter of depth from the skin, exhaustive hemostasis was performed, excision of the excess skin in the medial region, placement of drains and suture by planes to the skin. A sample of resected infiltrated tissue was sent for histopathological study. There were no complications during surgery (Figure 3).
Posoperative Care
Recovery in prone position for 21 days, hyperbaric chamber to guarantee oxygenation of flaps, daily cures avoiding infectious processes.
Posoperative Evolution
In the immediate posoperative period, she presented acute edematous pancreatitis that remitted with medical treatment and then she had a favorable evolution. The stitches were removed at 21 days with a clear improvement in local and systemic symptoms.
Anatomopathological Study
Biopsy of infiltrated tissue in the buttocks: Xantulogranulomatous chronic inflammatory process with a foreign body in the fat. Subcutaneous cellular tissue with calcification and marked sclerosing fibrosis around multiple cystic structures of variable size in the left and right buttock samples (Figure 4).
Discussion
The application of unauthorized substances for aesthetic purposes, to improve body and facial contours, such as mineral oils, hydrocarbons, industrial silicone, among others, continues to increase indiscriminately, leading to the production of diseases in the body with local or systemic manifestations [6, 7]. Iatrogenic allogenosis is not a new health problem, it has its origin in the 17th century where it had therapeutic purposes, at the beginning of the 20th century the first adverse events related to this type of non-surgical procedure were reported, such as pulmonary embolisms or injuries similar to lipomas in the paraffin application area. In 1973, the disease was described in humans for the first time in patients with silicone breast implants. At the end of the 1970s its use was prohibited for aesthetic purposes, however, nowadays various substances are used more frequently to achieve changes in the body figure, giving rise to clinical pictures that are included under the term modeling disease or Iatrogenic allogenosis, receives this name because it is produced by allogenic substances, that is, foreign to the organism and iatrogenic because it is produced by health personnel [1]. The clinic of the disease is indefinite, although it follows a cyclical pattern with variable intervals of stability and recurrence. These asymptomatic and symptomatic periods without pharmacological treatment have a mean presentation of two to three months on average [8]. It´s local and systemic manifestations are the result of the activation of the immune system due to the infiltration of foreign substances. They influence the clinical expression, the amount of substance used being directly proportional to the damage, and the anatomical region modified by the infiltration. It is described that the symptomatology is more intense when the substance has been applied in the gluteal region [9]. The most common local signs are inflammation, irregularities in the skin, edema, erythema, keloid scars, venous neoformations, hyper or hypopigmentations, ulcerations, hardening, migration of the substance to distant sites, necrosis and fistulas. The most common systemic symptoms are pain, fever, asthenia, adynamia, arthralgia, drowsiness, and depression [1].
The diagnostic criteria for this disease are: history of application of chemical substances for aesthetic purposes, clinical manifestations of some of the autoimmune diseases, demonstration of some type of autoantibody, histological evidence of chronic inflammation and foreign body granulomatous type, absence of infectious process or neoplastic, improvement of symptoms upon withdrawal of the injected substance. All of these criteria were met in the patient presented [10, 11]. At the beginning of the disease, treatment was based on multiple pillars, both local and systemic, currently in disuse, such as punctures, liposuction, antibiotics, and steroids. The indication for punctures to drain the substance was because the cysts that form are less than 2 cm in diameter. Liposuction for extraction of the product with the use of cannulas, but it was found that more healthy tissue was aspirated than alloplastic material whose pearls obstructed the suction instrument. Antibiotics were also eliminated from the treatment scheme as they did not constitute infections but rather an inflammatory response of an immune cause, and injected and topical steroids were also eliminated, which, far from destroying the material, further thinned the healthy tissue [1, 2]. Today the treatment of choice is symptomatic with anti-inflammatory and immunosuppressant’s and the extraction of the injected substance by surgical methods. Surgical treatment is indicated when there is exposure of the modeling material, removal of the injected material, abscesses, fistulas and deformity of the affected anatomical area which in the present case was evidenced with obstruction of the anal opening due to compression, generating alterations in defecation, for which the patient required enemas to defecate [12]. Although the surgical removal of the modeling substance relieves the symptoms, the total extraction of the product is difficult, since the organism does not isolate it, but rather interacts forming masses without defined borders that modify the anatomical consistency of the affected site [1].
In the transoperative period, areas of fibrosis with indurations can be found in the form of friable cords with multiple caverns inside which oil or the substance in the form of pearly white pearls of firm consistency can be seen [13]. In the present case, given the evolution of more than 10 years, the subcutaneous cellular tissue was infiltrated throughout its thickness with little vascularization and the caverns were lined like ground glass, which made it difficult to completely extract them. However, the patient presented a marked improvement in symptoms after surgery and had adequate healing.
Conclusion
Surgical treatment using the open biopolymer extraction method is deforming, but it is the only solution to improve the symptoms of iatrogenic allogenosis.
References
-
Tamayo Carbon AM, Orozco Jaramillo MA, Posada Ruiz DA (2019) Adjuvant substances and adjuvant-induced inflammatory autoimmune syndrome. Presentation of a case. Rev Panorama. Cuba and Health 15(1): 59-64.
-
Coiffman F (2008) Iatrogenic allogenosis: A new disease. Cir Plast Iberolatinoam 34(1): 1-10.
-
Cervera M, Regueira FM, Sola J, Valenti V, Pastor C, et al. (2006) Sequelae after illegal injection of liquid silicone as a breast augmentation technique: Presentation of 2 cases. Cir Esp 80(4): 227-229.
-
Ricaurte AL, Castano DA, Castro JA, De Paz DA, Echeverry DA, et al. (2016) Iatrogenic allogenosis vs. Secondary allogenosis in Cali, Colombia. About 12 cases. Colomb Forensic 3(2): 61-72.
-
Duarte Y, Sanchez A, Hedo Toledo AH, Mora JP, Recilla VG, et al. (2016) Late complication after infiltration of biopolymers in the buttocks. Cir Plast Iberolatinoam 42(4): 385-389.
-
Cardona Gonzalez MA (2018) Iatrogenic Allogenosis: Biopolymers and other substances. Blog dermatology and plastic surgery Medellin.
-
Farinas Acosta L (2016) Iatrogenic allogenosis, a new disease?. Granma 22(5): 28.
-
Marvis A, Abreu A, Maurette P (2015) Reaction to a foreign body by an injected biopolymer: presentation of a clinical case. Spanish Journal of Oral and Maxillofacial Surgery 37(1): 23-26.
-
Ripalda A, Loja A, Victor L, Herrera PJ, Freites P, et al. (2018) Clinical consequences of the use of biopolymers as self-care practices in the process of body transformation in transsexual people. Facsalud-Unemi 2(2): 46-52.
-
Dominguez Zambrano A (2013) Modeling disease: Current problems in Mexico and presentation of cases. Cir Plast Iberolatinoam 39(4): 399-405.
-
Gallegos Morales M (2018) Efficacy and safety of surgical treatment after iatrogenic allogenosis. Guayaquil University.
-
Gordillo J, Alegre E, Torres I, Mendieta M, Sastre N, et al. (2013) Multidisciplinary approach to human disease by adjuvants. Cir Plast Iberolatinoam 39(3): 269-277.
-
Tamayo Carbon AM, Estevez del Toro MH, Alvarado Salas R, Chong Lopez A (2019) Adjuvant-induced inflammatory autoimmune syndrome after administration of a modeling agent with fibromyalgia symptomatology. Colombian Journal of Rheumatology 26(2): 145-147.
- Reconstruction of Nasal Defect Using a Local Flap Based in the Nanoperforants Concept: A Case Report
- Transplant Tourism in Japan: Insights from Nationwide Surveys and Emerging Ethical Challenges
- The Challenge of Peritoneal Vaginoplasty in Transgender Women: Review Literature and Personal Perspectives
- Algorithmic Paternalism: Autonomy Versus Automation
- Dermatoscopy in Gorlin Syndrome: Avoiding the Disfigurement in Patients
- How Artificial Intelligence is Ushering in a New Era of Innovation in General and Plastic Surgery: A Short Communication