Immediate Combined Hand Reconstruction in a Patient with Complex Tissue Defect and Total Finger Amputation
Clinical evaluation of bones, tendons, joints, vessels, nerves and muscles at the patient's first presentation plays a critical role in determining the reconstruction plan of injured hand. In crush injury, skeletal stabilization forms the foundation for the entire reconstruction plane. In the basic approach, debridement of devitalized tissues, bone fracture stabilization, neurovascular repair, graft and flap coverage of critical tissues are applied respectively. In certain circumstances ectopic replantation can be an option in severely crushed injuries. Here in, we present the combined immediate reconstruction process of a patient applied with soft tissue defect in the hyposthenia region of the left hand, bony defect of the 4th and 5th metacarpals and total amputation of the 5th finger.
Introduction
Crush injuries of the hand are injuries that may cause a wide range of defects; from soft tissue laceration to complex tissue defects and even amputation. Clinical evaluation of bones, tendons, joints, vessels, nerves and muscles at the patient’s first presentation plays a critical role in determining the next step [1]. The main goal of treatment is to restore the basic functions of the hand, especially grasping and pincer movement. Thus, staged reconstruction is often preferred. In crush injury skeletal stabilization forms the foundation for the entire reconstruction plane. The other steps come as revascularization and skin coverage which can be done through local of free flaps [2]. In this case, we aimed to present the combined immediate reconstruction process of a patient applied with soft tissue defect in the hyposthenia region of the left hand, bony defect of the 4th and 5th metacarpals and total amputation at the level of the metatarsophalangeal joint of the 5th finger.
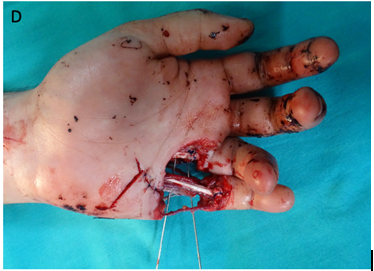
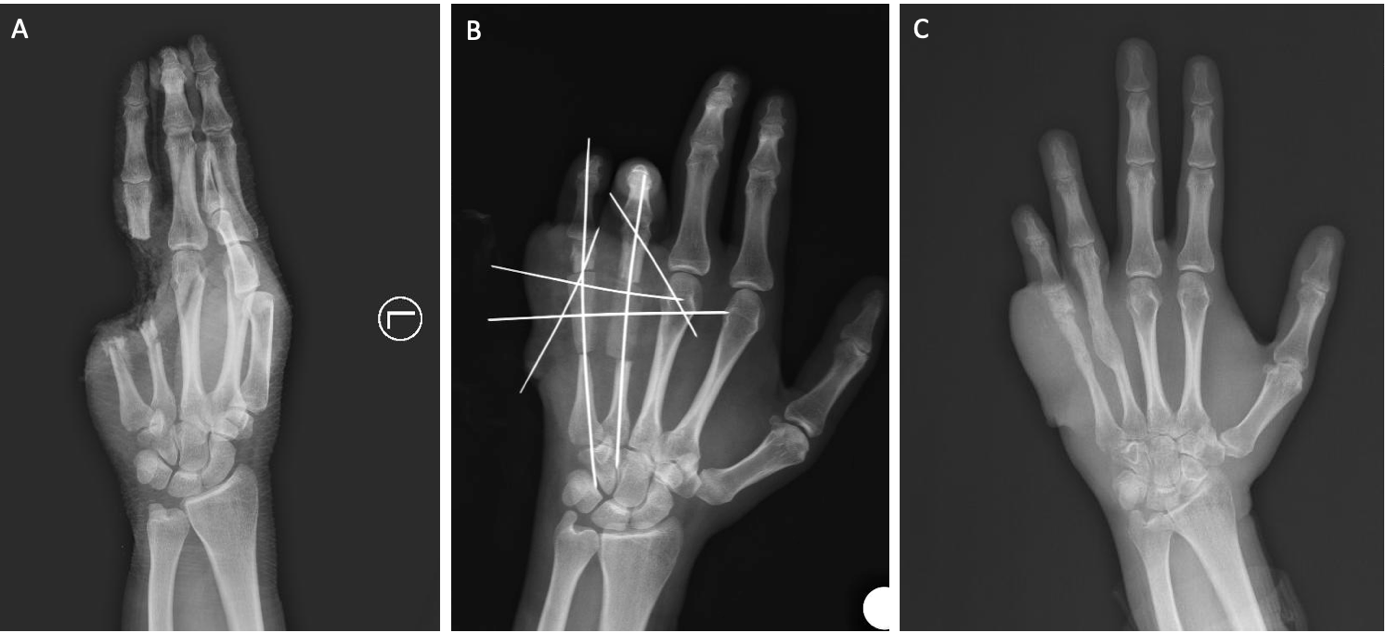
A 27-year-old man was admitted to our emergency department after his left hand was caught in a press machine. Physical examination of the patient revealed bone defects in the 4th and 5th metacarpals of the left hand (Figure 1A), total amputation of the 5th finger, the 4th finger was attached to the hand with a skin island on the radial side and capillary refill was normal (Figure 1B). Direct radiographs confirmed that the 4th finger of the left hand had a bony defect extending from the middle of the metacarpal bone to the middle of the proximal phalanx, 2/3 of the original 5th metacarpal bone was defective, the 5th finger was totally amputated from the middle level of the proximal phalanx (Figure 1C). The patient, who had no comorbidities and was a smoker, was operated under general anesthesia (Figure 1D).



Intraoperative evaluation showed that the radial side digital artery and nerve of the 4th finger were intact, all flexor and extensor tendons of the 4th and 5th fingers were totally lacerated. 4th and 5th finger’s metacarpal bones were defective. FDS tendon of the 5th finger was found to be long enough for repair, the digital arteries, nerves and 1 vein each on the volar and dorsal sides of the amputate were marked. A groin interpolation flap was planned for soft tissue reconstruction of the hyposthenia region of the left hand, bone grafting from the iliac bone through the same incision in the groin area was also planned for the reconstruction of the 4th-5th metacarpals (Figure 3A). A planned superficial circumflex iliac artery-based groin interpolation flap was harvested from the left inguinal region. As planned, a 4x2 cm bone graft was harvested from the iliac bone and split into half to obtain 2 bone grafts. After the bone grafts were placed in their appropriate places, they were fixed vertically with one Kitschier wire extending from the proximal phalanx to the carpometacarpal junction and horizontally to the 3rd metacarpal with two kitschier wires from the ulnar side of the hand (Figure 3B).
FDS tendon of the 5th finger was harvested to be used as a graft for reconstruction of the extensor tendons of the 4th and 5th finger and FDP tendon of the 5th finger. Defective digital nerves could not be repaired due to the wide gap and nerve repair was left for the next session. The common
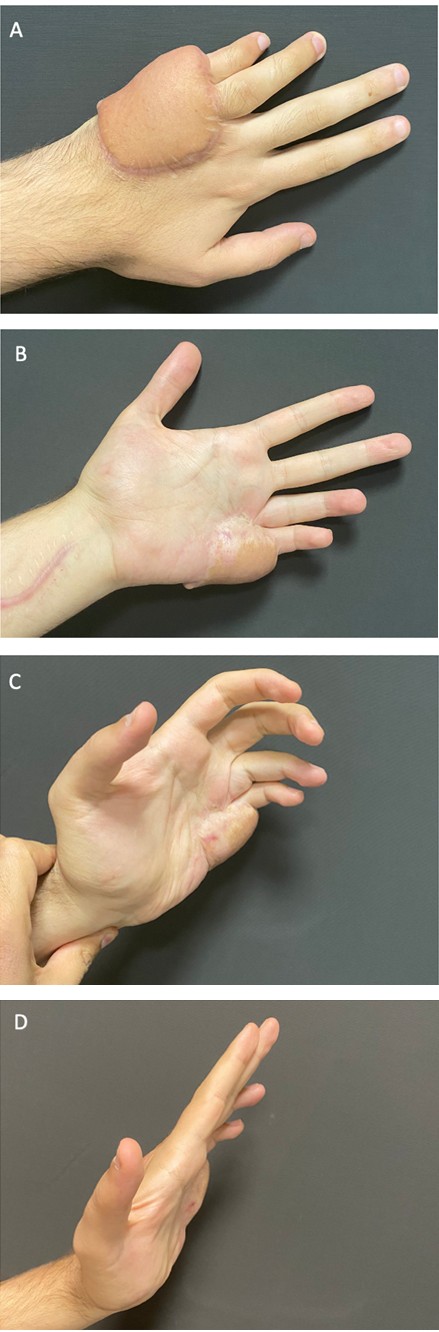
digital artery supplying the 4th and 5th fingers and the ulnar digital artery of the 5th finger were defective from the point where they branch from the palmar arch. Three vein grafts were harvested from the left forearm. The defective ulnar and radial digital arteries of the 5th finger and a previously marked vein on the volar side of the same finger were repaired using these vein grafts. All of the anastomosis worked well and capillary refill was noticed. Then, a vein with a vertically course on the dorsal aspect of the 4th finger was transposed and anastomosed to a previously marked vein on the dorsal aspect of the amputated 5th finger. All of the anastomosis worked well and normal capillary refill was observed on the 5th finger. For the repair of the soft tissue defect, the superficial circumflex iliac artery-based groin interpolation flap was used after kitschier wires were passed through the flap on the ulnar side of the hand. The groin flap was detached from the donor area after 3 weeks. Although a superficial circulatory defect was encountered at the distal end of the flap during follow-up, it didn’t require secondary surgery and the wound was healed completely (Figure 3C). The bone grafts healed very well without any sign of malunion (Figure 3D).
Discussion
Crush injuries are encountered in different ways depending on many variables such as the severity of the trauma, the mechanism of trauma and the characteristics of the tissue damage. In this context, it is important to establish patient-specific treatment management after detailed examination of the trauma site, as different tissues are damaged at varying rates in each patient [3, 4, 5]. General factors such as age of the patient, stability of the circulatory system, presence of life-threatening conditions, additional medical conditions, hot-cold ischemia time and local factors such as circulatory disorders, motor-sensory nerve examination findings and bone and joint damages play a critical role in the surgical planning [6].
In the basic approach, debridement of devitalized tissues, bone fracture stabilization, neurovascular repair, graft and flap coverage of critical tissues are applied respectively [7]. In high-energy hand injuries such as in our case; since the damage is spread to wider areas, other reconstructive processes such as reconstruction of defective bones, tendon repair and nerve repair can often be postponed after the viability of the fingers is ensured. Although it is not routinely practiced, a temporary ectopic replantation of the amputated tissues may be considered as an alternative option until the inflammatory process at the trauma site diminishes. This is considered to be a safer method [8].
However, it is important to keep in mind the disadvantages of delayed reconstructions which include the need of two microsurgery teams, the need for at least two major operations and the risk of thrombosis of the anastomosis will be at the same level for both of the operations [9, 10]. In our case, the combined loss of both bone and soft tissue accompanied with total amputation led us to search for a treatment that could provide both soft tissue and bone repair as soon as possible to secure the replantation. Considering the need for vein graft, it was necessary to have intact soft tissue cover to protect the anastomosed vascular structures. Therefore, by planning a superficial circumflex iliac artery- based groin interpolation flap, we obtained sufficient soft tissue coverage for bone grafts, repaired artery and veins and structures that would be reconstructed in the following stages. We reconstructed the defected metacarpals with bone graft obtained from the same incision and achieved bony skeletal stabilization without the need of another donor area.
Conclusion
Treatment of crush injuries of the hand requires early and accurate assessment of the injuries and a systematic approach tailored to each patient. First, the patient and the limb should be kept alive. Then, the function of the hand should be restored as much as possible. Although not always possible, but immediate reconstruction may be the ideal option in line with the opportunities provided by the trauma characteristics. It is easier for patients to undergo the rehabilitation process earlier so that they can return to their social and work life earlier.
References
-
Soucacos PN (2001) Indications and selection for digital amputation and replantation. J Hand Surg Br 26(6): 572- 581.
-
Lahiri A (2020) Guidelines for management of crush injuries of the hand. published correction appears in J Clin Orthop Trauma 11(4): 517-522.
-
Tang JB, Neumeister MW (2014) Hand repair and reconstruction. Clin Plast Surg 41: 13-14.
-
Gerken M, Saller MM, Ockert B, Böcker W, Volkmer E (2023) Detailed analysis of surgically treated hand trauma patients in a regional German trauma centre. PLoS One 18(3): e0283388.
-
Dadaci M, Ismayilzade M, Zuhour M, Uyanık O, Ince B, et al. (2021) Management of mole gun injuries: Review of 19 cases with proposed treatment algorithm. Hand Surg Rehabil 40(3): 319-325.
-
Hart RG (2005) Hand injury prevention. Ann Emerg Med 45(6): 636-638.
-
Del PF (2020) An Update on the Management of Severe Crush Injury to the Forearm and Hand. Clin Plast Surg 47(4): 461-489.
-
Nazerani S, Motamedi MKH (2009) Ectopic single-finger transplantation, a novel technique for nonreplantable digits: assessment of 24 cases--presenting the “piggyback” method. Tech Hand Up Extrem Surg 13(2): 65-74.
-
Yoshida S, Koshima I, Narushima M, Nagamatsu S, Yokota K, et al. (2019) Usefulness of ectopic implantation in multiple finger amputation injury. Clin Case Rep 7(3): 546-549.
-
Yousif NJ, Dzwierzynski WW, Anderson RC, Matloub HS, Sanger JR (1996) Complications and salvage of an ectopically replanted thumb. Plast Reconstr Surg 97(3): 637-640.
- Reconstruction of Nasal Defect Using a Local Flap Based in the Nanoperforants Concept: A Case Report
- Transplant Tourism in Japan: Insights from Nationwide Surveys and Emerging Ethical Challenges
- The Challenge of Peritoneal Vaginoplasty in Transgender Women: Review Literature and Personal Perspectives
- Algorithmic Paternalism: Autonomy Versus Automation
- Dermatoscopy in Gorlin Syndrome: Avoiding the Disfigurement in Patients
- How Artificial Intelligence is Ushering in a New Era of Innovation in General and Plastic Surgery: A Short Communication