Decadal Outcomes of Prefabricated Urethral Reconstruction in Phalloplasty
Urethral reconstruction in phalloplasty for transgender men poses considerable challenges and risks. Despite numerous surgical techniques, an ideal method has yet to be found. This study offers a 10-year follow-up on prefabricated urethral reconstruction with full-thickness skin grafts in radial forearm free flap phalloplasty. Sensory outcomes of the neophallus after one year matched those of the control area, and patients successfully achieved self-standing urination. Penile prosthesis insertion took place five years post-surgery. A thorough review of existing literature and surgical methods is included for discussion.
Introduction
Achieving the ability to urinate while standing has been a longstanding goal in penile reconstruction. Since the first total phalloplasty with optional urethral reconstruction using an inlaid skin graft in 1936, various techniques for urethral reconstruction in phalloplasty have been used, including the one-stage tube-in-tube technique and prefabricated urethral reconstruction with full-thickness skin grafts in lateral arm free flap and fibula flap methods, other approaches, such as Techniques such as the double flap method, which combines the anterolateral thigh flap with the radial forearm flap, small intestinal mucosal grafts, buccal mucosa, peritoneum, and bladder mucosal grafts, have also been applied [1, 2, 3, 4, 5, 6].
The limitations of each technique prevent there from being a perfect technique. This study provides long-term successful outcomes of prefabricated urethral reconstruction in radial forearm free flap phalloplasty using full-thickness skin grafts.
A 32-year-old transgender male with gender dysphoria was referred for penile reconstruction, specifically radial forearm phalloplasty. The patient had a BMI of 23.5 and no history of smoking. He had been on male hormonal therapy for three years and had previously undergone a mastectomy, hysterectomy, and oophorectomy. After discussing the surgical procedure details and options for neourethral reconstruction and phalloplasty, the patient chose a left radial forearm free flap with a prefabricated urethra using a skin graft. The Allen test of both forearms was positive, and the left mid-forearm circumference was 17.0 cm.
Surgical Procedures
Stage I
Prefabricating Urethra with Full-Thickness Skin Graft A full-thickness skin graft from the left gluteal fold was inverted and sutured around a 24 French silicone catheter. The patient was required to maintain the stent, with daily changes, for six months postoperatively (Figure 1). A total vaginectomy and urethral lengthening with an anterior vaginal flap for pars fix a urethral reconstruction were also performed.

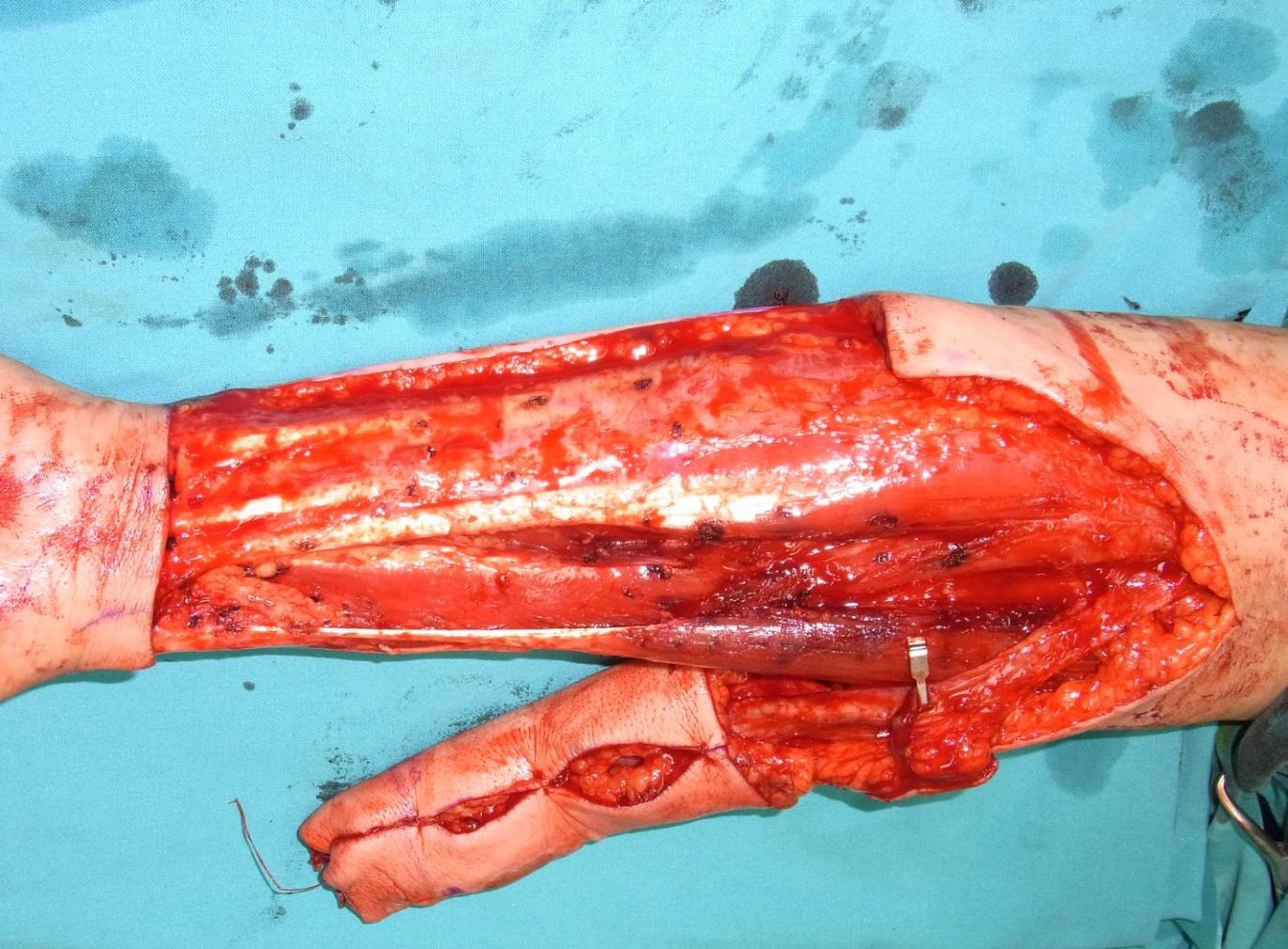
Stage II
Radial Forearm Free Flap Six months after urethral prefabrication, the patient underwent microscopic radial forearm phalloplasty under general anesthesia in a supine position. A radial forearm flap, approximately 12 cm wide and 13 cm long, was marked on the skin. The radial artery and concomitant veins were identified, including the anterior branch of the medial antebrachial cutaneous nerve and the lateral antebrachial cutaneous nerve in the flap. The radial forearm flap was mobilized for the neophallus (Figure 2). The femoral artery and great saphenous vein served as recipient vessels, with the distal saphenous vein used for the vein graft to extend the radial artery for microscopic anastomosis. Two sensory nerves were connected to the clitoral nerves and the right ilioinguinal nerve, respectively. The urethral pars pendulans were joined to the pars fixa with a 20 French silicone Foley catheter. The donor site on the left forearm was covered with a split-thickness skin graft from the left thigh. The urinary catheter was retained for three weeks postoperatively, and the patient urinated successfully without fistula (Figure 3). To prevent urethral stricture from skin graft contracture, the patient was advised to maintain the urethral stent for 12 months. Follow-up visits at three months and one year postoperatively showed penile sensation comparable to the control area. The patient received a malleable penile prosthesis five years postoperatively. At the 10-year follow-up, the patient reported a satisfaction score of 5/5, penile sensation of 5/5, and self-confidence of 5/5 on a scale of 1 to 5 (Figure 4).


Discussion
The incidence of complications in urethral reconstruction during phalloplasty varies among the different surgical techniques. Both urethral strictures and fistulas are commonly observed in patients who undergo phalloplasty, regardless of whether a single-stage or multi-stage operation is performed. There is ongoing debate regarding the optimal approach, with some surgeons preferring to offer urethral reconstruction as an additional, separate procedure [4]. The application of mucosal grafts from the bladder, small intestine, vaginal lining, or peritoneum has been documented infrequently [1, 2, 3, 4, 5, 6].
The one-stage tube-in-tube technique is often preferred in radial forearm flap phalloplasty because it has a reduced likelihood of causing urethral stricture [2]. However, this method may not be suitable for patients with smaller forearms, as seen in this study with a patient having a 17.0 cm mid-forearm circumference. We opted for prefabricating the urethra using a skin graft in radial forearm phalloplasty due to its comparably low risk of urethral fistula and its suitability for patients with smaller forearm circumferences. Moreover, the staged technique involving skin grafting is generally more dependable for wound healing than grafting onto flaps in a single-stage surgery. Skin graft donor sites from the gluteal fold area have less hair compared to those from the groin or lower abdomen, though preoperative hair removal is recommended to prevent hair growth within the urethra.
This study highlights the successful long-term outcomes of urethral prefabrication in radial forearm flap phalloplasty, followed by secondary penile prosthesis insertion. However, this technique has its limitations, including the need for staged surgeries, careful selection of donor skin graft sites, the presence of hair in skin graft donor areas, and the necessity for the patient to use a urethral stent or undergo urethral dilation for at least one year postoperatively. Future research should include a larger cohort of patients and employ statistical analysis to further validate these findings.
Patient Consent: The patients provided written consent for the use of images.
Conflicts of Interest: The authors have nothing to disclose.
Ethical Approval: The procedures were in accordance with the ethical standards of the institutional research committee.
Funding: None.
References
-
Hage JJ, de Graaf FH, Van den Hoek J, Bloem JJ (1993) Phallic construction in female-to-male transsexuals using a lateral upper arm sensate free flap and a bladder mucosa graft. Ann Plast Surg 31(3): 275-280.
-
Chen ML, Reyblat P, Poh MM, Chi AC (2019) Overview of surgical technique in gender-affirming genital surgery. Transl Androl Urol 8(3): 191-208.
-
Sluis WBVD, Smit JM, Pigot GLS, Buncamper ME, Winters HAH, et al. (2017) Double flap phalloplasty in transgender man: surgical technique and outcome of pedicled anterolateral thigh flap phalloplasty combined with radial forearm free flap urethral reconstruction. Microsurgery 37(8): 917-923.
-
Djorrdjevic ML (2018) Novel surgical techniques in female to male gender confirmation surgery. Transl Androl Urol 7(4): 628-638.
-
Rubino C, Figus A, Dessy LA, Alei G, Mazzocchi M, et al. (2009) Innervated island pedicled anterolateral thigh flap for neo-phallic reconstruction in female-to- male transsexuals. J Plast Reconstr Aesthet Surg 62(3): e45-e49.
-
Pansritum K, Yingthaweesittikul S, Attainsee A (2022) Urethral reconstruction with peritoneal graft in phalloplasty for male transgender. J Plast Reconstr Aesthet Surg 75(7): 2387-2440.
- Reconstruction of Nasal Defect Using a Local Flap Based in the Nanoperforants Concept: A Case Report
- Transplant Tourism in Japan: Insights from Nationwide Surveys and Emerging Ethical Challenges
- The Challenge of Peritoneal Vaginoplasty in Transgender Women: Review Literature and Personal Perspectives
- Algorithmic Paternalism: Autonomy Versus Automation
- Dermatoscopy in Gorlin Syndrome: Avoiding the Disfigurement in Patients
- How Artificial Intelligence is Ushering in a New Era of Innovation in General and Plastic Surgery: A Short Communication