The Influence of the Concurrent Use of Catha edulis Forsk (Khat) and Empagliflozin on Dexamethasone-Induced Hyperglycemia in Rabbits
Background: Despite the abundance of reports highlighting the negative health consequences allied with Khat chewing, a considerable number of individuals worldwide, particularly in its countries of origin, persist in using Khat on a daily basis. This presents a significant risk of co-administering Khat and drugs, thereby increasing the likelihood of adverse interactions between Khat and drugs. Hence, it is imperative to evaluate the effects of simultaneous usage of Khat and drugs. The current study primarily focused on empagliflozin, a sodium glucose cotransporter-2 inhibitor that has emerged as a prominent treatment for Type 2 diabetes mellitus (T2DM) by targeting SGLT-2 in the kidney. Aim: The present study aimed to assess the impact of administering Khat and empagliflozin together on dexamethasoneinduced hyperglycemia in rabbits. Methods and Materials: Thirty adult male rabbits weighing between 1-1.3kg were randomly divided into six groups, each consisting of five rabbits. During two weeks, dexamethasone (10 mg/kg) was administered orally to four groups continuously to induce hyperglycemia. Group I, which served as the control, received normal saline. Group II, however, received a Khat dose (1500 mg/kg). Group III consisted of diabetic rabbits who remained untreated and only received normal saline in an equivalent dosage. The fourth, fifth, and sixth groups of animals were treated with daily oral doses of Khat (1500mg/kg), empagliflozin (10 mg/kg), and a combination of both, respectively, to treat dexamethasone-induced hyperglycemia for two weeks. At the end of the experiment, samples of blood were gathered in the morning after an overnight fasting period. Results: The study findings revealed that both Khat (p <0.00) and empagliflozin (p <0.00) monotherapy significantly reduced hyperglycemia and body weight. However, the combination of Khat and empagliflozin was found as the most effective, surpassing the effects of Khat alone. Conclusion: These findings suggest that the combination of empagliflozin and Khat had a greater efficacy in reducing fasting blood glucose levels in comparison with the ordinary control group. However, caution should be exercised as this may potentially lead to hypoglycemia in Khat chewers who are also using empagliflozin as a medication.
Introduction
Catha edulis, generally called as “Khat,” is tree or large shrub that is endogenously found in Arab peninsula specially in Yemen, some African countries such as Ethiopia and Kenya, and in Western Asia [1]. For centuries, Khat had been traditionally and mainly used for its psychostimulant, euphoric, and analgesic activity. People chew the Khat leaves to release the active constituents slowly to be ingested with saliva. Chewing sessions can last from 3 to 7 hours. It is estimated that 20 million people worldwide chew Khat leaves daily [2].
The habit of Khat chewing is widespread with a deep- rooted sociocultural tradition in Yemen and as such poses a public health problem. Khat consumption has intensely increased recently, and the drug has also appreared in Great Britain. Khat chewing may have a negative effect on the central nervous system, cardiovascular system, digestive system and genitourinary system, oral-dental tissues, diabetes mellitus and cancer. Khat chewing may be associated with increased risk of cardiovascular and blood coagulation disorders [3, 4, 5]. It also may interfere with absorption, metabolism and mechanism action of some orally administered drugs.
Diabetes mellitus (DM) is a group of metabolic diseases distinguished by hyperglycemia caused by deficiencies in insulin secretion, insulin action or both. Diabetes is linked with long-term damage, dysfunction and failure of different organs, especially eyes, kidneys, nerves, heart and blood vessels. Over the past three decades, the prevalence of DM in the global adult population has surged by 20%, and projections indicate that by 2040, the worldwide diabetic population will reach 642 million [6].
Empagliflozin, an inhibitor of the sodium-glucose cotransporter 2 (SGLT2), is a relatively new medication that has shown promising results in the management of Type 2 diabetes mellitus (T2DM). By increasing urinary glucose excretion, it helps increase glycemic control, enhance glucose metabolism, and reduce glucotoxicity and insulin resistance. However, its benefits extend beyond its original purpose.
Besides its hypoglycemic effect, empagliflozin has demonstrated nephroprotective properties and has emerged as a breakthrough treatment for heart failure (HF). Studies have revealed that empagliflozin can decrease hospitalizations for HF and the rate of cardiovascular-related deaths. Furthermore, it has been found to reduce the risk of renal events, including death by renal causes, and the growth of end-stage renal failure.
Empagliflozin is generally well-tolerated and considered safe. When used as monotherapy or in combination with other therapies, it efficiently reduces fasting blood glucose, postprandial blood glucose, regular daily glucose levels, and glycated hemoglobin A1C (HbA1C). Additionally, it has been associated with substantial weight decrease in patients having T2DM who have insufficient glycemic control.
Overall, empagliflozin provides a range of advantages to manage T2DM. These include enhanced control over blood sugar levels, protection for the kidneys, and a groundbreaking treatment for heart failure. Its favorable safety profile and additional effects make it a valuable choice for patients who struggle with maintaining adequate glycemic control [7]. Despite the abundance of reports underscoring the severe health risks linked to Khat consumption, a considerable portion of the global population persists in using Khat regularly, especially in its nations of origin. This behavior significantly heightens the chances of simultaneous intake of Khat and medications, thereby elevating the probability of negative reactions between the two substances [8]. In light of this situation, it is imperative to ascertain whether chewing Khat negates or amplifies the effects of oral antidiabetic medications, which are administered to reduce blood sugar levels in patients with Type 2 diabetes mellitus.
Material and Methods
Materials
Fresh Khat (leaves and stem tips) were consistently sourced from a nearby supplier named Hamdani. The leaves were moist and finely ground using a blender machine prior to being given via gastric gavage. Empagliflozin from YEPHCO in Yemen and dexamethasone from Memphis in Egypt were purchased from a local pharmacy.
Methods
Ethical Consideration: The current study got approval from the ethical committee of Al-Razi University, Sana’a, Faculty of Medicine and Health Sciences that adopt the guidelines for ethical conduct in the care and use of animals provided by American Association of Psychologists.
Animals Handling
It is a prospective study carried out on thirty adult male rabbits, each weighting 1-1.2kg. They have acclimatized for one week and were caged (5 / cage) in fully ventilated room. They were allowed to free access to water and diet containing cereals and bread. The study lasted for 5 weeks during November and December, 2023. Adult female rabbits were omitted from the study for removing the potential impact of pregnancy and the oestrous cycle on the parameters. The rabbits were bought from the neighborhood market, taken in and acclimated to their new surroundings at a steady temperature. They were then given an unlimited supply of a typical chow diet for one week.
The experiment used thirty rabbits in total. Following a week of acclimation, the animals under study were divided into six groups, with five animals in each group, and two groups kept as controls. The experimental conditions for both the control and experimental groups were the same. For two weeks, dexamethasone (10 mg/kg) was administered orally to five groups continuously to induce hyperglycemia (a blood sugar level higher than that of humans). One control group received simply normal saline. Daily oral doses of Khat (1500 mg/kg) or empagliflozin (10 mg/kg) singly and combination were used to treat dexamethasone-induced hyperglycemia in the fourth, fifth and sixth groups of animals respectively for two weeks. Samples of blood were gathered after the experiment end early at morning when the animals had been kept fasting over the night. The fasting blood sugar measurement was done in accordance with the method of Trinder [9]. The body weight was measured regularly for 14 days.
Preparation of Khat Extract
Fresh Khat leaves were acquired from a nearby market in Sana`a. The botanical composition of the plant material was determined and verified by a taxonomist at the Faculty of Sciences, Sana`a University. The leaves underwent a thorough washing with distilled water before 30 g of meticulously chosen fresh leaves were blended using an electric blender. Subsequently, they were immersed in 10 mL of distilled water for 2 hours to achieve a concentration of 3000 mg/ mL. Following this, 0.5 mL (equivalent to a concentration of 1500 mg/kg body weight) of the filtrate was administered via gavage intra-gastrically to each rabbit undergoing Khat treatment for 14 days. The selection of this particular dose (1500 mg/kg) depended on the average amount chewers typically consume and dosages utilized in comparable research studies [10].
Experimental Design
In the beginning of the experiment animals were divided into 6 groups (5 rabbits each). All animals except group I and II received dexamethasone induced hyperglycemia by oral (10 mg/kg) for 2 weeks as a method for induction of Type
2 diabetes [11]. For such animals, non-fasting blood glucose level was measured by electronic glucose meter (Accu-Chek Active apparatus, Germany) using a drop of blood obtained from marginal ear vein puncture. Animals which showed FBG levels > 150 mg/dl were recognized diabetic and enrolled in the experiment.
Animal Groups
Group1: Normal rabbits and received drug vehicle in comparable volume to administered drugs. Group 2: Normal rabbits treated with Khat in a dose of 1500 mg/kg for 2 weeks. The dose signifies the regular Khat consumption in humans according to [3, 10]. Group 3: Diabetic rabbits (Non-treated diabetic control). Group 4: Diabetic rabbits treated with Khat in a dose of 1500 mg/kg for 2 weeks. Group 5: Diabetic rabbits treated with empagliflozin (EMPA) which was administered in a dose 10 mg/ kg /day for 2 weeks [12]. Group 6: Diabetic rabbits treated with Khat and EMPA in doses of (1500 mg/kg) and (10 mg/kg) respectively, for 2 weeks.
Statistical Analysis
The results were experienced as mean ± standard error of the mean (S.E.M). The overall significance was measured by One Way Analysis of Variance (ANOVA). The statistical analysis program, Statistical Package Social Sciences (SPSS) version 25, was used. The p values are considered significant when p <0.05 or less [13].
Results
Body Weight
The mean body weight of the control group was 1044.80 ± 21.10g. Introducing hyperglycemia through oral dexamethasone administration led to a notable increase in body weight in comparison with the control group. Diabetic rabbits treated with Khat exhibited a significant decrease in body weight in comparison with the untreated diabetic group refer to Table 1. Treatment with EMPA resulted in a significant decrease in body weight compared with the untreated diabetic group. Concurrent administration of EMPA and Khat presented a significant decrease in total body weight in comparison with both the untreated diabetic group and the control group (Figure 1).
Fasting Blood Glucose
The fasting blood glucose (FBG) levels of the normal control group were recorded as 94.00 ± 0.70 md/dl. The group that received Khat treatment displayed a significant decrease in FBG levels to be compared to the normal control group. In contrast, the Dexamethasone administration orally induced hyperglycemia, leading to a significant increase in FBG levels in comparison with the normal control group. In the diabetic group, the Khat-treated group exhibited a significant decrease in FBG levels compared to the non-treated diabetic group. These values were considered statistically significant based on the data presented in Table 2. Furthermore, the diabetic group that received EMPA treatment showed a significant decrease in FBG levels compared to the non- treated diabetic rabbits. Interestingly, when EMPA and Khat were co-administered, a significant reduction was displayed in FBG levels compared to the non-treated diabetic rabbits, as shown in Figure 2.
| Groups | Normal rabbits | Normal rabbits treated with Khat | Diabetic rabbits (non-treated) | Diabetic rabbits treated with Khat | Diabetic rabbits treated with EMPA | Diabetic rabbits treated with EMPA and Khat |
|---|---|---|---|---|---|---|
| Body weight (g) | 1054.60 ± 19.45 | 1075.80 ± 36.30 | 1333.00 ± 25.18acd | 938.0 ± 25.15 be | 900.60 ± 35.36abce | 728.20 ± 21.20abcde |
Table 1: The impact of combining Khat and EMPA during 2 weeks on, on dexamethasone induced hyperglycemia in rabbits, on average (
Table 1: The impact of combining Khat and EMPA during 2 weeks on, on dexamethasone induced hyperglycemia in rabbits, on average (mean ± S.E) body weight (kg) (n=5). a,b,c,d,e: Significant versus control, Khat treated control, non-treated diabetic rabbits, diabetic rabbits-Khat treated, EMPA group and Khat+ EMPA treated diabetic group respectively at p<0.000.
| Groups | Normal Control | Normal rabbits treated with Khat | Diabetic rabbits (non- treated) | Diabetic rabbits treated with Khat | Diabetic rabbits treated with EMPA | Diabetic rabbits treated with EMPA and Khat |
|---|---|---|---|---|---|---|
| Fasting blood glucose (mg/dl) | 94.00 ± 0.70 | 83.00 ± 2.12a | 169.80 ± 2.78abcde | 127.40± 1.91abcde | 109.40 ± 0.81abcde | 82.60 ± 3.74acde |
Table 2: Effect of co-administration of Khat and EMPA for 2 weeks, on dexamethasone induced hyperglycemia in rabbits, on average
Table 2: Effect of co-administration of Khat and EMPA for 2 weeks, on dexamethasone induced hyperglycemia in rabbits, on average (mean ± S.E) FBG levels (mg/dl) (n=5) a,b,c,d,e: Significant versus control, Khat treated control, non-treated diabetic rabbits, diabetic rabbits-Khat treated, EMPA group and Khat+ EMPA treated diabetic group respectively at p<0.000.
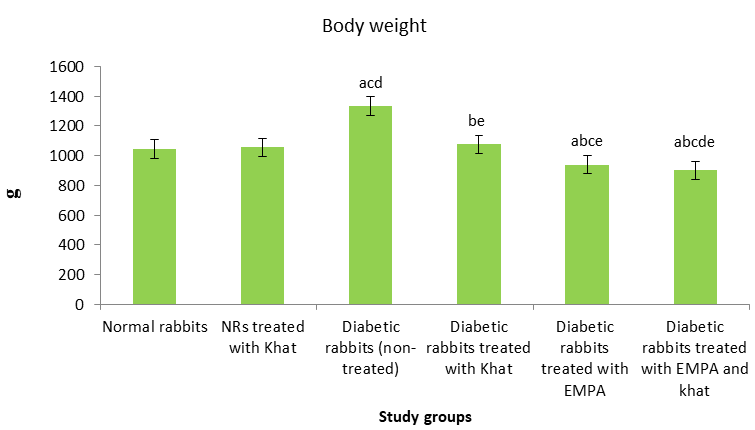
Figure 1: Effect of administering Khat and EMPA simultaneously for 2 weeks, on dexamethasone induced hyperglycemia in rabbits, on average (mean ± S.E) body weight (kg) (n=5). a,b,c,d,e: Significant versus normal control group, normal rabbits with Khat, non-treated diabetic group, diabetic with Khat group, EMPA treated diabetic group and EMPA with Khat treated diabetic group respectively at P < 0.000.
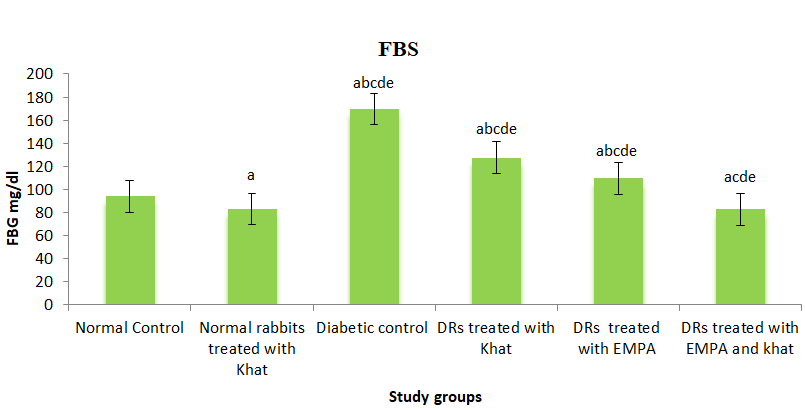
Figure 2: Impact of concurrent use of Khat and EMPA for 2 weeks, on dexamethasone induced hyperglycemia in rabbits, on average (mean ± S.E) FBG levels (mg/dl) (n=5). a,b,c,d,e: Significant versus control, Khat treated control, non-treated diabetic rabbits, diabetic rabbits-Khat treated, EMPA group and Khat+ EMPA treated diabetic group respectively at p<0.000.
Discussion
Although several reports have concerned the associations between Khat chewing and acute health complications, a significant percentage of the global population goes on involving in everyday Khat consumption, mainly in its countries of origin. This creates a sensitive risk of co-administering Khat with drugs among these people, thereby increasing the possibility of contrary interactions between Khat and medications [8]. Under these conditions, it is important to assess the effect of associated administration of Khat and EMPA, a recently developed medication, acts as an inhibitor of the sodium-glucose cotransporter-2 (SGLT2). This mechanism leads to greater removal of glucose through urine, leading to improved glycemic control, enhanced glucose metabolism, reduced glucotoxicity, and decreased insulin resistance [7].
In this study, the use of oral dexamethasone was functioned as a means to simulate the beginning of Type 2 diabetes. This method resulted in developing the insulin resistance, as specified by a significant increase in total body weight and FBG levels [14, 15]. This result agrees with who revealed that such model produces insulin resistance rather than insulin shortage. Glucocorticoid-induced hyperglycemia mainly happens through the stimulation of hepatic glucose production and increased lipolysis in adipose tissue. This causes the development of insulin resistance throughout the body, as well as reduced production and secretion of insulin by pancreatic β-cells. The glucocorticoid receptor plays a substantial role in mediating many of these effects by binding to definite target genes and regulating their transcriptional appearance. The tissue-specific effects of glucocorticoids contribute to the total diabetogenic effect in vivo through inter-organ signaling.
The administration of fresh leaves extracted from Khat resulted in a remarkable reduction in FBG levels, while no significant modification was perceived in the overall body weight of normal control rabbits. These findings are consistent with the findings of a study carried out by Albaser NA, et al. [3] which revealed that Khat consumption led to a substantial reduction in FBG levels among non-diabetic rats. This effect attributed to the appetite sedative and the delayed gastric emptying time effects of Khat [16, 17]. The reduction in fasting blood glucose levels in diabetic and healthy rats due to Khat may be associated with a reduction in the absorption rate of carbohydrates into the portal hepatic circulation. The delayed absorption of glucose from the gastrointestinal tract could be attributed to the delayed gastric emptying caused by tannins and inorganic ions observed in Khat.
Moreover, the present study demonstrated that the administration of Khat resulted in a decrease and complete restoration of FBG levels and body weight. These reductions were found to be significantly lower in comparison with the higher values observed in the non-treated diabetic rabbits group. In addition, Khat treatment assisted in regularizing these levels. This phenomenon can be attributed to the reduction of blood glucose levels through the mechanisms previously stated. The study showed that EMPA treatment effectively reduced and removed insulin resistance indicators. FBG levels and body weight were remarkably lower in comparison with the high levels observed in untreated dexamethasone-induced hyperglycemia, and were brought back to normal. Empaglifozin’s effectiveness in improving insulin sensitivity is attributed to its specific mechanism of action, including the liver, muscles, adipocytes, pancreas, and neuroendocrine system in the regulation of glucose levels [7]. Additionally, the current study indicated that the kidneys assist to maintain glucose balance by reabsorbing filtered glucose, confirming ample energy during fasting. In diabetes mellitus, the overexpression and activity of SGLT2 in the kidney’s proximal tubule due to high blood sugar disrupts this mechanism [18]. SGLT2, located in the proximal convoluted part of the proximal tubule, works as a high-capacity, low-affinity glucose transporter. It combines glucose transport to the electrochemical Na+ gradient and simplifies 90% of renal glucose reabsorption, with the remaining 10% being reabsorbed by the high- affinity, low-capacity SGLT1 transporter. The process of SGLT2 includes the absorption of sodium through the luminal cell membrane, producing a gradient that lets glucose to inactively pass in the cell. Consequently, the sodium is transported back to the bloodstream by the adenosine triphosphatase-mediated sodium–potassium pump, while glucose disperses to the basolateral glucose transporter 2 for re-entry into the bloodstream. Elevated blood sugar levels improve the function of SGLT2, leading to an increase in glucose reabsorption by as much as 20% in patients with uncontrolled diabetes. Empagliflozin works by blocking SGLT2, thus was reducing the reabsorption of glucose in the kidneys and lowering the onset for glucosuria. Accordingly, this causes higher excretion of glucose in the urine and a reduction in hyperglycemia [19]. Its action leads to excretion of 60–100 g of glucose per day, development of glucose control with low risk of hypoglycemia and also results in loss of 240–400 kcal/day into the urine with associated weight reduction. In healthy volunteers, EMPA produces a dose- dependent growth in urinary glucose excretion of up to 90 g per day. The mechanism results in the elimination of 60– 100 g of glucose daily, enhancing glucose regulation while lessening the probabilities of hypoglycemia. In addition, it leads to the expulsion of 240–400 kcal/day through urine, contributing to weight loss. EMPA makes an increase in urinary glucose excretion of up to 90 g per day in healthy participants.
The combination of EMPA and Khat resulted in a more significant decrease in fasting blood glucose (FBG) levels and body weight. The impact on serum glucose was mainly remarkable in comparison with the empagliflozin group. Furthermore, the combination therapy had a significant effect on overall body weight and FBG levels in comparison with the EMPA group alone. These additional effects observed with the combination of Khat and EMPA can be attributed to the separate mechanisms of action of the two drugs. Khat mainly works by decreasing the carbohydrate absorption rate into the portal hepatic circulation, as proved by a recent study conducted by Alqahtani AS, et al. [20]. This study confirmed that the combination treatment significantly improved the blood sugar-lowering effects of metformin. The results also showed that the combined treatment led to increased systemic exposure to MT, with Cmax and AUC levels rising by 33.42% and 45.23% respectively. Additionally, the combination treatment resulted in significantly lower FBG levels in comparison with the groups treated with MT alone. Additionally, Vitro findings from the same study proposed that high doses of Khat extract may affect CYP3A4 activity [20]. The delayed gastric emptying effect of tannins and the existence of inorganic ions in Khat may contribute to the delayed absorption of glucose from the gastrointestinal tract, while empagliflozin works as an inhibitor of the sodium-glucose cotransporter 2 (SGLT2) [7]. Therefore, the simultaneous use of EMPA and Khat may have an additional effect on FBG levels. It is crucial to thoroughly follow up this interaction in diabetic patients who consume Khat and are undergoing EMPA treatment, as it could potentially lead to hypoglycemia [21, 22].
Limitation of the Study
The current study was conducted as an preliminary assessment to investigate the effects of combining Khat with EMPA on blood glucose levels over a specific period. However, additional research, including prolonged animal experiments, clinical trials, the effect of Khat on EMPA pharmacokinetics, and the assessment of other factors, is required.
Conclusions
According to the above findings and observations, it can be concluded that Khat and metformin combination could be more effective than metformin in treatment of insulin resistant diabetes. The combined administration of Khat and EMPA is much more effective in controlling the insulin resistant diabetic state.
Conflict of Interest
The author declares no conflict of interest.
Acknowledgments
The author expresses thankfulness to the investigators who took part in this study: Abdul-Rahman Zuhair, Abdullah Naif, Abdul Rahman Nassar, Abdullah Dubaish, Mohammed Derhm, Marwan Aissa, Moaied Saif, Mohammed Nasser, and Ali Abdul Kareem, for their valuable assistance during the research.
References
-
Al-Juhaishi T, Al-Kindi S, Gehani A (2012) Khat: A widely used drug of abuse in the Horn of Africa and the Arabian Peninsula: Review of literature. Qatar Med J 2012(2): 1-6.
-
Alsalahi A, Alshawsh MA, Mohamed R, Alyousefi NA, Alshagga MA, et al. (2016) Conflicting reports on the role of the glycemic effect of Catha edulis (Khat): A systematic review and meta-analysis. J Ethnopharmacol 186: 30-43.
-
Albaser NA, Mohamad A-WH, Al-Kamarany MA (2021) Influence of co-administration of Khat (Catha edulis Forsk) and metformin on metabolic syndrome in high fructose diet induced Type 2 diabetes in rats. Natl J Physiol Pharm Pharmacol 11(7): 767-773.
-
Albaser NA, Mohamad AWH, AL-Kamarany MA, Al-Ahdal SA, Al-Awar MSA, et al. (2022) Impact of Khat (Catha Edulis Forsk), During Chewing Session, on Serum RBG Level in T2DM Patients Treated with Metformin. J Pharm Negat Results. Published online 13(7): 43-47.
-
Al-Kamarany MA, Albaser NA, Kadi HO, Lyoussi B (2022) Effect of Khat on Blood Coagulation. Abhath J Basic Appl Sci 1(2): 1-5.
-
Bodke H, Wagh V, Kakar G, WAGH V (2023) Diabetes mellitus and prevalence of other comorbid conditions: a systematic review. Cureus 15(11): e49374.
-
Forycka J, Hajdys J, Krzemińska J, Wilczopolski P, Wronka M, et al. (2022) New Insights into the Use of Empagliflozin-A Comprehensive Review. Biomedicines 10(12): 3294.
-
Albaser NA, Mohamad A-WH, AL-Kamarany MA (2021) Khat-drug interactions: A systematic review. J Pharm Pharmacogn Res 9(3): 333-343.
-
Trinder P (1969) Determination of glucose in blood using glucose oxidase with an alternative oxygen acceptor. Ann Clin Biochem 6(1): 24-27.
-
Kennedy C, Okanya P, Nyariki JN, Amwayi P, Jillani N, et al. (2020) Coenzyme Q10 nullified Khat-induced hepatotoxicity, nephrotoxicity and inflammation in a mouse model. Heliyon 6(9): e04917.
-
Doa’a AI (2009) Study of the Effect of Panax Ginseng versus Gliclazide on hyperglycaemia induced by dexamethasone in experimental animals. Sultan Qaboos Univ Med J 9(1): 63-69.
-
Liu Y, Wu M, Xu J, Xu B, Kang L, et al. (2021) Empagliflozin prevents from early cardiac injury post myocardial infarction in non-diabetic mice. Eur J Pharm Sci 161: 105788.
-
Hill BA (1971) Principles of medical stastics 9th(Edn.), The Lancet, London, pp: 147-283.
-
Ackerman Z, Oron-Herman M, Grozovski M, Rosenthal T, Pappo O, et al. (2005) Fructose-induced fatty liver disease: hepatic effects of blood pressure and plasma triglyceride reduction. Hypertension 45(5): 1012-1018.
-
Chou CL, Lai YH, Lin TY, Lee TJF, Fang TC, et al. (2011) Aliskiren prevents and ameliorates metabolic syndrome in fructose-fed rats. Arch Med Sci AMS 7(5): 882-888.
-
Murray CDR, Le Roux CW, Emmanuel AV, Halket JM, Przyborowska AM, et al. (2008) The effect of Khat (Catha edulis) as an appetite suppressant is independent of ghrelin and PYY secretion. Appetite 51(3): 747-750.
-
Heymann TD, Bhupulan A, Zureikat NEK, Bomanji J, Drinkwater C, et al. (1995) Khat chewing delays gastric emptying of a semi‐solid meal. Aliment Pharmacol Ther 9(1): 81-83.
-
DeFronzo RA, Davidson JA, Del Prato S (2012) The role of the kidneys in glucose homeostasis: a new path towards normalizing glycaemia. Diabetes, Obes Metab 14(1): 5-14.
-
Chawla G, Chaudhary KK (2019) A complete review of empagliflozin: Most specific and potent SGLT2 inhibitor used for the treatment of Type 2 diabetes mellitus. Diabetes Metab Syndr Clin Res Rev 13(3): 2001-2008.
-
Alqahtani AS, Parvez MK, Alqahtani AM, Fantoukh OI, Herqash RN, et al. (2023) Effects of Catha edulis (Khat) on the Pharmacokinetics of Metformin in Diabetic Rats Using UPLC/MS/MS Analysis and Its Impact on Hepatic CYP450 Enzymes. Separations 10(8): 442.
-
Saif-Ali R, Al-Qirbi A, Al-Geiry A, Al-Habori M (2003) Effect of Catha edulis on plasma glucose and C-peptide in both Type 2 diabetics and non-diabetics. J Ethnopharmacol 86(1): 45-49.
-
El-sayed MIK, Amin HA (2012) Effect of Catha Edulis on Insulin, Resistin and Cortisol Levels in Type-2 Diabetics and Non-Diabetics. American Journal of Biochemistry and Biotechnology 8(3): 157-163.
- Potential Medicinal Herbs and Secondary Metabolites in Combating Corona Virus
- Monkeypox and its Clinical Implications in Pregnancy
- Pharmacognostical Analysis of the Leaves of Important Nervine Medicinal Plant: Strychnos Nux-Vomica L
- Assessment of Antibacterial Activity of Various Solvent Extracts of Dictyota Dichotoma Against Multidrug Resistant Bacterial Strain
- An Insights of Bioactive Elements on Malignancy: Mechanistic Avenues
- Advances and Future Directions in Pharmacognosy and Chinese Medicine