Topographical Variations of Wormian Bones in Eastern-Indian Dry Human Skulls: Current Perspective and Review of Literature
Wormian bones occur due to the failure of fusion of the additional ossification centers with prominent skull bones. It may be misinterpreted as a fracture in cases of trauma. Several studies reported the racial differences in the incidence of Wormian bone. We aimed to determine the incidence of Wormian bone in the adult dry skull of the eastern Indian population with its location. A total of 30 adult dry (male – 14; female – 16) skulls of unknown age were included in the study. 53.33% (16) of the skull had the Wormian bones, out of which 13.33% (4) had a single Wormian bone; a maximum of ten Wormian bone was observed in a skull. The highest incidence of Wormian bone was observed in the lambdoid suture and pterion (62.5%) followed by asterion and coronal sutures with an incidence of 31.25% and 6.25%, respectively. Out of the four Inca bones, the largest Inca measured 63.8 x 59.6mm. Wormian bones are present in normal individuals with lower incidence. The number of Wormian bones increased in the pathological condition that shows its pathological and diagnostic implications. The knowledge about the Wormian bone is necessary to differentiate it from fracture or diagnosis of pathological condition underlying it. We hope the present study helps radiologists or surgeons in successfully differentiating a skull fracture from the Wormian bones by using modern-day imaging techniques.
Introduction
Wormian bones or sutural bones are occurring due to the failure of fusion of the additional ossification centers with main skull bones [1]. It may vary in size, shape, location and number in different individuals. Few studies reported in the literature show racial or regional variation. The individual bone that occurs at the posterior fontanelle is named as Inca bone, preparital bone or Goethe’s ossicle [2, 3]. Wormian bones occurrence is related to both genetic and environmental factors. Though Wormian bones usually occur in few individuals, it is also reported in many autosomal dominant genetic disorders [4]. The most common site of occurrence is in the lambdoid suture, followed by other sutures and fontanelle. The least common site is bregma. Knowledge about the incidence and location of sutural bone is essential to interpret the radiological images of the skull to distinguish the Wormian bone from fracture lines. In the case of misinterpretation, the treatment course is different and causes a delay in the timely treatment of emergencies. Thus, the present study was aimed to determine the incidence of Wormian bone in the adult dry skull of the eastern Indian population with its location.
Materials and Methods
A total of 30 adults dry (male – 14; female – 16) skulls of unknown age from the Department of Anatomy, All India Institute of Medical Sciences, Bhubaneswar were included in this study after institutional ethical committee approval. The skull with ante-mortem or post-mortem injuries or disarticulated skulls were excluded. Each skull was examined from anterior to posterior for the presence of sutural or wormian bones. The presence of wormian bone with its location, side, number and dimension was recorded. The measurements are taken with the help of a digital Vernier caliper with 0.01mm precision.
Statistical analysis
The comparison of incidence in different locations and dimensions of right and left was performed using a student’s t-test. The size of the wormian bones was expressed as mean ± SEM. All statistical analyses were performed by using SPSS (Statistical Package for Social Sciences) version 25.0 (SPSS, Chicago, IL). A P value < 0.05 was considered statistically significant.
Results
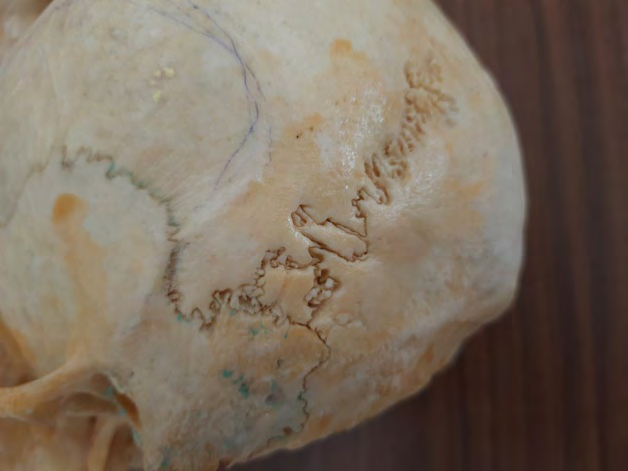
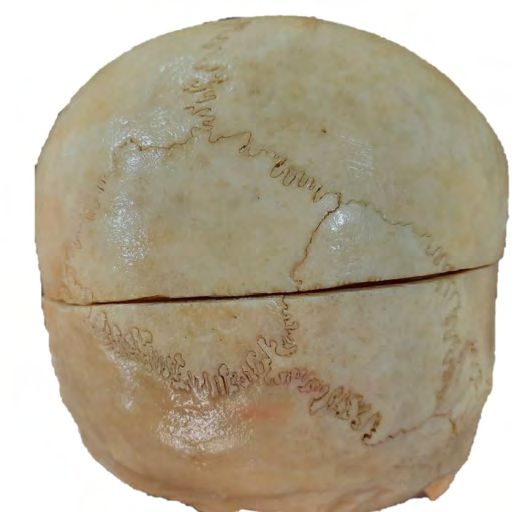
Out of 30 skulls examined, 16 (53.33%) skulls had single or multiple Wormian bones. The number of Wormian bones in a skull were ranging from one to ten. Single Wormian bone was found in four skulls (13.33%), two to five Wormian bones were found in eight skulls (26.67%). More than five Wormian bones were observed in four skulls (13.33%). The maximum number of Wormian bones were found in a single skull is ten (3.33%). In the present study, a total of 60 wormian bones were observed, out of which four (13.33%) are Inca bones. Incidence of wormian bones is maximum in lambdoid suture (62.5%) (right – 56.25%; left – 50%; bilateral – 43.75%) and pterion (62.5%) (right – 43.75%; left – 25%; bilateral – 6.25%), followed by asterion and coronal sutures composed of 31.25% and 6.25% of wormian bone. Wormian bones were not found in sagittal suture and bregma. Overall, 62.5% of skulls shown bilateral wormian bone. The incidence of wormian bones on the right side is slightly higher than the left side. Size of inca bone is relatively larger than Wormian bone. Out of the four Inca bone, the largest Inca was measuring 63.8 x 59.6mm was found in a female skull along with five wormian bones in the lambdoid suture (Figures 1-3).

Discussion
Wormian bones was named after the Danish anatomist Olaus Worm, who mentioned it in a letter to Thomas Bartholin in 1643 [5, 6]. The first description of wormian bone as “ossiculum antiepilepticum” in the literature was made by Paracelsus (1493-1541) [5]. They believed sutural bone has antiepileptic characters. Several authors mentioned it as ossa suturalis, accessory ossicles, Paracelsian ossicle, Ossa wormiana, ossicula Andernaci, ossa Goethiano, ossa triquetra, ossa triangularis, ossa quadratum, suturaux, fontanellaires, insules, intercalaria and raphogeminantia based on their discoverer, shape, location and function [7]. The morphogenesis of wormian bones is still controversial. In 1977, El-Najjar et.al., reported that wormian bones formation is not influenced by mechanical distortion [8]. However, recent studies suggesting that mechanical factor that spread sutures apart results in the formation of wormian bones [9]. Some authors suggesting the genetic factor for the formation of wormian bone as its incidence was higher in few congenital disorder such as cleidocranial dysostosis, pycnodysostosis, rickets, kinky hair, osteogenesis imperfect, Menkes disease, hypothyroidism and hypophosphatasia, Down syndrome, otopalatodigital syndrome, primary acro‑osteolysis and congenital disorders affecting the neural tube development [7, 10, 11].
The incidence of wormian bone in the literature is widely varying from 9% to 73%. The highest incidence was reported in the south Indian population (73.1%). In contrast, the lowest was reported in the Turkey population (9%) [7, 12]. Incidence of multiple wormian bones was reported higher in the West Anatolia population (39.3%) [6]. The maximum and minimum rates of sutures that had Wormian Bones were found in left lambdoid 40.7% and right occipitomastoid 1.3% sutures, respectively. There was only a significant difference between the rate of right and left squamous sutures (P = 0.04). A study conducted on the Eastern Indian population reported 45% of skull having wormian bones, out of which 30% contains multiple wormian bones [5]. In the present study, we observed 53.3% of skulls with wormian bones. In line with the previous literature, Lambdoid suture observed to have a higher incidence of wormian bone and bregma not having any wormian bone in the present study.
Even though wormian bones are present in normal individuals, its incidence is increased in the pathological condition that shows its pathological and diagnostic implications [13]. The detailed description of the incidence, size, distribution in the normal individuals helps us to differentiate it from the wormian bones in the pathological condition [14]. Several authors hypothesized that the wormian bone should be arranged more than ten in number and each should be more than 4 to 6mm in size to label it as a pathological [14]. Wormian bones were commonly seen in the pathological condition where there is raised intracranial pressure or premature closure of sutures like hydrocephalus and cleidocranial dysplasia respectively [9, 15]. Rarely in cases of decreased ossification of the skull, cranial sutures and fontanelles to be wider and for the skull to remain in a malleable state for a longer period of time [9]. The knowledge about the sutural bone is necessary for the physician for the early diagnosis and timely management of disorders associated with it. We hope the present study helpful to radiologists and surgeons in successfully differentiating a skull fracture from normal suture with Wormian bones by using modern-day imaging techniques.
Conflict of Interest
The authors declare that they have no conflict of interest.
References
-
OLoughlin VD (2004) Effects of Different Kinds of Cranial Deformation on the Incidence of Wormian Bones. Am J Phys Anthropol 123(2): 146-155.
-
Marathe RR, Yogesh AS, Pandit SV, Joshi M, Trivedi GN (2010) Inca-Interparietal bones in neurocranium of human skulls in central India. J Neurosci Rural Pract 1(1): 14-16.
-
Zambare BR (2001) Incidence of interparietal bones in adult skulls. J Anat Soc India 50: 11-12.
-
Bellary SS, Steinberg A, Mirzayan N, Shirak M, Tubbs RS, et al. (2013) Wormian bones: A review. Clin Anat 26: 922-927.
-
Ghosh SK, Biswas S, Sharma S, Chakraborty S (2017) An anatomical study of wormian bones from the eastern part of India: is genetic influence a primary determinant of their morphogenesis? Anat Sci Int 92(3): 373-382.
-
Cirpan S, Aksu F, Mas N (2015) The incidence and topographic distribution of sutures including wormian bones in human skulls. J Craniofac Surg 26(5): 1687- 1690.
-
Murlimanju BV, Prabhu LV, Ashraf CM, Kumar CG, Rai R, et al. (2011) Morphological and topographical study of Wormian bones in cadaver dry skulls. J Morphol Sci 28(3): 176-179.
-
El Najjar MY, Dawson GL (1977) The effect of artificial cranial deformation on the incidence of wormian bones in the lambdoidal suture. Am J Phys Anthropol 46(1): 155-160.
-
Lara PAS, Graham JM, Hing AV, Lee J, Cunningham M (2007) The morphogenesis of wormian bones: A study of craniosynostosis and purposeful cranial deformation. American Journal of Medical Genetics 143A(24): 3243- 3251.
-
Randhawa M, Dhawan S, Kumar S, Singanamala B, Bhatia A, et al. (2019) Wormian bones and dilated scalp veins in an infant with epilepsy. J Pediatr Neurosci 14(2): 103- 104.
-
Goyal N, Garg A, Kumar Y (2019) Incidence and medicolegal significance of wormian bones in human skulls in North India Region. Int J Appl Basic Med Res 9(3): 165-168.
-
Govsa F, Ozer MA, BayrakTaroglu S, Aktas EO (2014) Anatomoradiological identification of intrasutural bones for importance of cranial fracture. Turk Neurosurg 24(3): 357-362.
-
Kalpan S, Kemp S, Oh K (1991) Radiographic manifestations of congenital anomalies of the skull. Radiol Clin N Am 29(2): 195-218.
-
Cremin B, Goodman H, Spranger J, Beighton P (1982) Wormian bones in osteogenesis imperfecta and other disorders. Skeletal Radiol 8(1): 35-38.
-
Semler O, Cheung MS, Glorieux FH, Rauch F (2010) Wormian bones in osteogenesis imperfecta: Correlation to clinical findings and genotype. Am J Med Genet 152A: 1681-1687.
- Pattern of Breast Lesions in Ovu Inland, Delta State, South Southern Nigeria
- Morphometric Analysis of the Human Femur: Exploring Platymetric and Robusticity Indices Among the Nigerian Population
- Anatomical Variation of Arteria Lusoria: Clinical Implications for Dysphagia Lusoria and Surgical Risk
- Morphometric Study of the Vertebral Body and Pedicle of Typical Cervical Vertebrae Using Radiological Image
- Epigenetic Mechanisms Driving Human Evolutionary Changes
- Neuroprotective Effects of Ginkgo Biloba Extract on Bilateral Common Carotid Artery Ischaemic Stroke Induced in Wistar Rat