Occupancy of the Suprascapular Notch by the Suprascapular Nerve: An Anatomic Study
The purpose of the study was to evaluate the dimensions of the suprascapular nerve and the suprascapular notch in freshfrozen cadaveric shoulders and to calculate the occupancy ratio of the notch, i.e. the space occupied by the suprascapular nerve and the superior transverse scapular ligament (STSL). The suprascapular nerve and the suprascapular notch were dissected, and the following parameters were included in the study: presence and shaper of the notch, dimensions of the lower border of the superior transverse scapular ligament and dimensions of the notch and the dimensions of the suprascapular nerve in two directions perpendicular to each other. All measurements were performed using a digital Vernier caliper. The cross-sectional area of the suprascapular nerve was assumed to be elliptical; the area of a U-shaped notch was assumed to be semi-elliptical and the area of the triangular-shaped notch were calculated accordingly. The area of the between the various notch types and the cross-sectional area of the suprascapular nerve in the various notch types were statistically compared. The reliability of continuous measurements was analyzed using intraclass correlation coefficients (ICCs). The suprascapular notch was present in all cases. A U-shaped notch was the most common type (22, 69%) followed by a triangular-shaped notch (10, 31%). The interobserver reliability of the suprascapular nerve and notch dimensions was excellent (ICC = 0.92 and 0.96 respectively). The cross-sectional area of the suprascapular nerve was 5.982.34 mm2 with no difference between the two body sides. The cross-sectional area of the U-shaped suprascapular notch was significantly larger than that of the V-shaped notch (19.98 5.34 mm2 versus 13.777.34 mm2, p=0.02). Correspondingly, the occupancy of the suprascapular notch by the suprascapular nerve was higher in V-shaped rather than U-shaped notches (37.199.34% versus 49.417.32%, p=0.03).
Introduction
The suprascapular notch is located at the superior border of the triangular scapula in proximity with base of the coracoid process. The notch is superiorly enclosed by the superior transverse scapular ligament (STSL). Occasionally the STSL is absent, and the notch acquires the form of a foramen. Several morphological variations of the suprascapular notch have been described and can be V, U, J or O-shaped [1, 2, 3, 4]. Rengachary, et al. [4] have described 6 types of the suprascapular notch based on its shape in American cadaveric population. Occasionally, the STSL is ossified, or the notch is missing [1, 2, 5, 6]. An ossified STSL is found in 10.3% of patients with a rotator cuff tear [7].
The suprascapular nerve is a mixed motor and sensory nerve which originates from the superior trunk of the brachial, consisting of fibers from the C5 and C6 nerve roots and typically is passing through the suprascapular notch innervating with 1-3 branches the supraspinatus muscle [4]. It then passes through the spinoglenoid foramen at the base of the scapular spine innervating the infraspinatus muscle. The suprascapular nerve can be extrinsically compressed or subjected to excessive traction leading to a peripheral neuropathic syndrome associated with posterior shoulder pain, atrophy of the supraspinatus and/or infraspinatus muscle and reduced muscle strength [8, 9, 10].
Suprascapular neuropathy may affect 1-2% of all patients who present with shoulder pain, especially younger than 40 years of age [11]. In overhead athletes the incidence of suprascapular neuropathy is higher and is estimated to be present in 12% to 33% in all athletes [8]. The etiology of suprascapular neuropathy is variable. The suprascapular nerve may be entrapped at various locations including the suprascapular notch, the spinoglenoid notch or the STSL. Occasionally, space-occupying lesions may exert direct pressure on the nerve, primarily at the spinoglenoid notch [12].
Aim of the Study
The primary aim of the study was to measure the dimensions of the suprascapular nerve and the suprascapular notch in fresh-frozen cadaveric shoulders and the secondary aim to calculate the occupancy ratio of the suprascapular notch, i.e. the space occupied by the suprascapular nerve and the STSL.
Materials and Methods
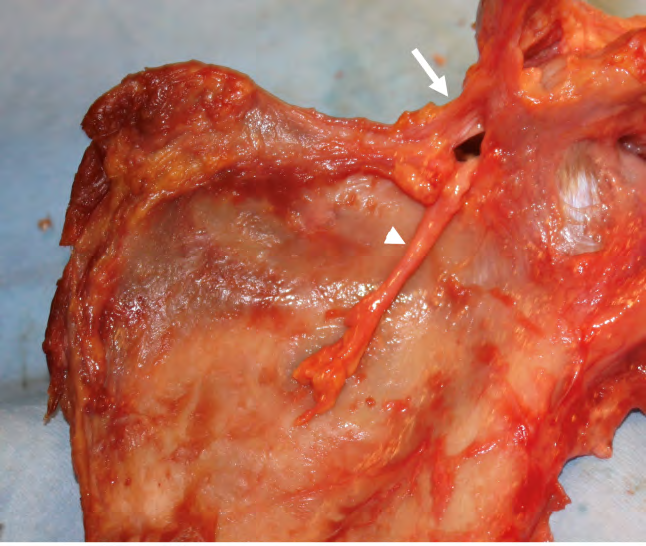
The present study was carried out on 32 fresh-frozen cadaveric shoulders, used previously in shoulder arthroscopy workshops. All shoulders were from male donors aged 47- 68 years with a mean age of 58.33 years. In their medical history no shoulder disease was present. There were 23 right shoulders and 9 left shoulders. The study was approved by the institutional Scientific Committee (Approval number 1287/11/09/2023). The suprascapular nerve and the suprascapular notch were dissected using a combination of sharp and blunt dissection (Figure 1).
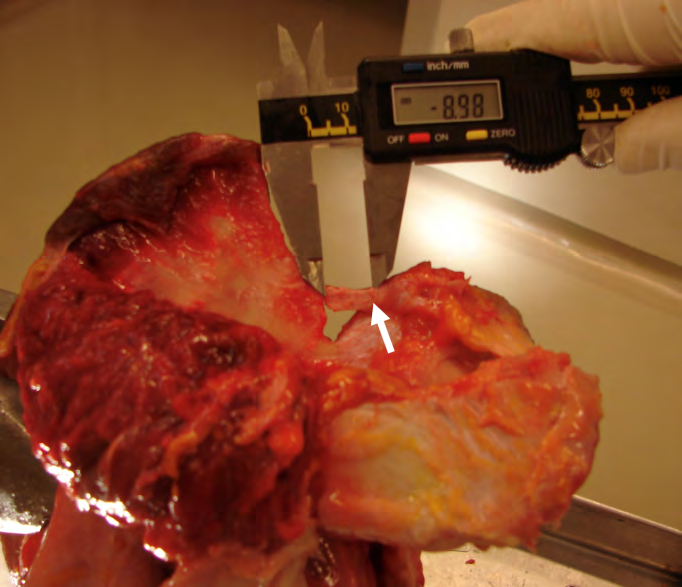
The parameters included in the study were the presence of a notch, the shape, the dimension of the lower border of the superior transverse scapular ligament and the dimensions of the notch and the dimensions of the suprascapular nerve in two directions perpendicular to each other. All measurements were performed using a digital vernier caliper (Figure 2). The distances were expressed in millimeters and the area expressed in square millimeters, mm2.
We chose to use an elliptical rather than a circular shape of the suprascapular nerve, because very often the two measurements of the nerve were significantly dissimilar (Figure 3). The cross-sectional area (CSA) of the suprascapular nerve was assumed to be elliptical and was calculated using the formula A = πab, where, A is the area, a is the length of the semi-major axis, b is the length of the semi-minor axis and π equals 3.14. For example, in a suprascapular nerve with horizontal diameter 3.3 mm and vertical diameter 2.6 mm, the area of the nerve, assuming an elliptical shape was 6.74 mm2 and its circumference 9.3 mm.
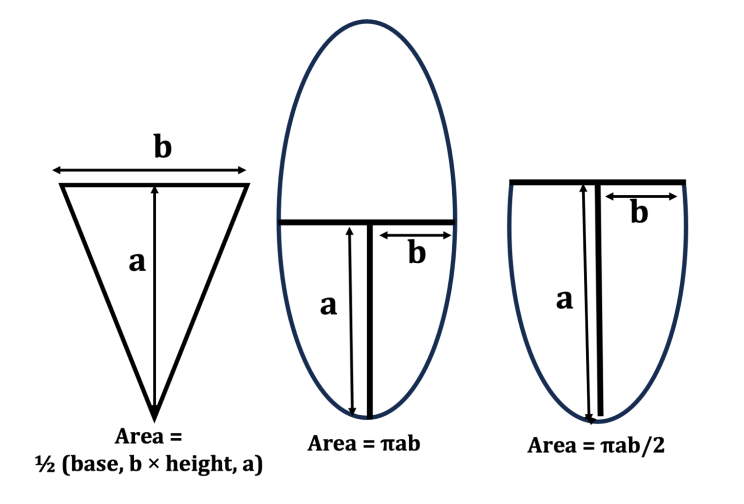
In a U-shaped notch the area was assumed to be semi- elliptical and was calculated using the formula A = πab/2, where, A is the area, a is the length of the semi-major axis, b is the length of the semi-minor axis and π equals 3.14. For example, in a notch where the depth was 6.5 mm and the upper limit of the notch, i.e. the inferior surface of the STSL was 7 mm, the area of the notch was 17.87 mm2 and the perimeter 17.61 mm.
In a triangular-shaped notch the Area of the Triangle (A) was calculated with the formula A = ½ (base × height). The inferior dimension of the STSL was the base of the triangle and the distance between the STSL and the deepest point of the notch was assumed to be the height of the triangle.
The area of the between the various notch types and the cross-sectional area of the suprascapular nerve in the various notch types were statistically compared using the Mann Whitney U test due to uneven distribution of data. The level of statistical significance was set at p<0.05. Intraobserver reliability of the measurements was evaluated by performing all measurements in 7 shoulders twice within 24 hours. The reliability of continuous measurements was analyzed using intraclass correlation coefficients (ICCs). Statistical analysis was performed using SPSS software, version 28.0 (SPSS Inc, Chicago, IL)
Results
The suprascapular notch was present in all cases. A U-shaped notch was the most common type (22, 69%) followed by a triangular-shaped notch (10, 31%). The interobserver reliability of the suprascapular nerve and notch dimensions was excellent (ICC = 0.92 and 0.96 respectively). The STSL was band-shaped in 25 cadavers (78%) and fan- shaped in 7 cadavers (22%).
The horizontal diameter of the suprascapular nerve was 3.26±1.01 mm and the vertical diameter 266±1.32 mm (p=0.03). CSA of the suprascapular nerve was 5.98±2.34 mm2. There was no difference in the suprascapular nerve CSA between the right and the left side (p=0.23), probably because most of the shoulders were right shoulders.
The CSA of the U-shaped suprascapular notch was significantly larger than that of the V-shaped notch (19.98 ±5.34 mm2 versus 13.77±7.34 mm2, p=0.02). Correspondingly, the occupancy of the suprascapular notch by the suprascapular nerve was higher in V-shaped rather than U-shaped notches (37.19±9.34% versus 49.41±7.32%, p=0.03).
Discussion
Our study showed that the suprascapular nerve has ample space within the suprascapular notch, especially in a U type notch compared to a V-shaped notch. Release of the STSL increases the available space within the suprascapular notch.
The morphologic properties of the suprascapular nerve and the suprascapular notch have been described using mostly formalin-fixed cadaveric shoulders [5, 13, 14] or dried scapula’s [1, 2, 3, 6]. Formalin, a solution of formaldehyde is the most common chemical fixative used in histopathology, providing excellent preservation of tissue morphology [15]. The fixative induces various changes in the tissues including shrinkage, swelling, and hardening of various components [16, 17, 18]. Fixation in 10% buffered formalin initially causes slight swelling of tissue specimens but during processing the specimen may shrink 20% - 30% of its volume [16, 17, 18]. Most tissues shrink when placed in a formalin fixative solution [19, 20]. We used in our study only fresh frozen cadaveric shoulders to reduce the effect of formalin fixation on the soft tissues.
We formulas to calculate the area of the suprascapular notch measuring in V-shaped notches the depth and the length of the sides of the notch and in U-shaped notches the depth and the inferior length of the STSL. Other authors used a visual analysis software of photographs of the notch [13], but most are measuring only the vertical depth and the superior and intermediate transverse diameters of the suprascapular notch [5, 3, 6, 14].
Several methods have been used to measure the CSA of the suprascapular notch including quantitative analysis of cadaveric photographs of the suprascapular notch, MRI, and ultrasound imaging [13, 14, 21, 22].
Quantitative visual data analysis software was used to measure the areas of the STSL and the anterior coracoscapular ligament, when present, as well as the diameters of the SN and associated vessels [13]. The mean diameter of the SN was 2.4 ± 0.33 mm and the area of the suprascapular opening between 73.51 mm2 and 131.61 mm2 [13].
In a similar study in on formalin-fixed cadaveric shoulders digital photographs of the suprascapular notch were obtained and analysed using a quantitative analysis software [14]. In this study the mean surface area of the suprascapular opening ranged between 22.6 ± 12.4 mm2 and 32.1 ± 14 mm2.
The suprascapular notch and its contents can be evaluated using ultrasound imaging. In a relevant study using ultrasound imaging in volunteers, the notch width, the notch depth and the distance between the skin and the notch base were measured [21]. The presence of the STSL was verified in 96% of the cases. The notch width was 12.85 mm in the right and 12.39 mm in the left shoulder and the notch depth 8.22 and 8.06 mm respectively.
The CSA of the suprascapular notch has been measured using MRI in patients with suprascapular nerve entrapment and in controls [22]. In the entrapment group the CSA was 44.94 ± 10.40 mm2 and in the entrapment group 64.50 ± 8.93 mm2. The accuracy of the measurements has though been rightfully debated [23] because in MRI sequences, which are not 3 dimensional, the location of the suprascapular notch is not precise due to difficulty in delineating its anatomical borders.
Although the most common aetiology of suprascapular neuropathy is compression by a cyst at the spinoglenoid notch (in 42% of the cases) [12], external compression of the suprascapular nerve during his course through the suprascapular notch is possible. A V-shaped, narrow, or deep suprascapular notch has been implicated as a potential cause of nerve compression [20]. In our study the CSA of the V-shaped suprascapular notch was significantly lesser compared to the most encountered O-shaped notch. Similarly, the space occupied by the suprascapular nerve was larger in V-shaped suprascapular notches. On the other hand, many patients with suprascapular nerve neuropathy show clinical and electrophysiological evidence of more extensive peripheral nerve disease and diffuse muscle involvement [9]. Arthroscopic decompression of the suprascapular nerve aims at dissecting the STSL in order to increase the space available for the nerve. This technique provides significant pain relief but incomplete muscle strength recovery [10]. The problem must be recognized early and treated promptly.
The present paper has several strengths and limitations. The study was performed using fresh-frozen cadaveric shoulders avoiding the negative effect of formalin embalming. All measurements were performed by the author obtaining excellent interobserver reliability. On the other hand, only shoulders without a clinical history of shoulder operations or diseases were included, which may influence the results and depreciate the effect of low suprascapular nerve occupancy of the suprascapular notch. The presence of the suprascapular veins and their space-occupying effect in the suprascapular notch has also not been considered.
Conclusion
Our study showed that compression of the suprascapular nerve in a V-shaped suprascapular notch is more probable due to the higher occupancy ration of the suprascapular nerve within the notch. Release of the STSL in those cases may be more beneficial compared to a U-shaped suprascapular notch where the available space is higher.
Conflicts of Interest
The author has no competing interest to declare.
Funding
No funding was received in support of this study.
References
-
Agrawal D, Singh B, Dixit SG, Ghatak S, Bharadwaj N, et al. (2015) Morphometry and variations of the human suprascapular notch. Morphologie 99(327): 132-140.
-
Albino P, Carbone S, Candela V, Arceri V, Vestri AR, et al. (2013) Morphometry of the suprascapular notch: correlation with scapular dimensions and clinical relevance. BMC Musculoskeletal Disorders 14: 172.
-
Polguj M, Jędrzejewski K, Podgórski M, Topol M (2011) Morphometric study of the suprascapular notch: proposal of classification. Surgical and Radiologic Anatomy 33(9): 781-787.
-
Rengachary SS, Burr D, Lucas S, Hassanein KM, Mohn MP, et al. (1979) Suprascapular entrapment neuropathy: a clinical, anatomical, and comparative study. Part 2: anatomical study. Neurosurgery 5(4): 447-451.
-
Long R, Wang N, Liu W, Liu Z, Cheng S, et al. (2019) An anatomical study of the superior transverse scapular ligament of Jining population. Surgical and Radiologic Anatomy 41(11): 1345-1349.
-
Podgórski M, Topol M, Sibiński M, Grzelak P, Stefańczyk L, et al. (2014) New parameters describing morphological variations in the suprascapular notch region as potential predictors of suprascapular nerve entrapment. BMC Musculoskeletal Disorders 15: 396.
-
Kim JY, Rhee YG (2018) The prevalence and morphometric analysis of ossified superior transverse scapular ligaments in patients with rotator cuff tears. Journal of Shoulder and Elbow Surgery 27(6): 1044-1050.
-
Lajtai G, Pfirrmann CW, Aitzetmüller G, Pirkl C, Gerber C, et al. (2009) The shoulders of professional beach volleyball players: high prevalence of infraspinatus muscle atrophy. The American Journal of Sports Medicine 37(7): 1375-1383.
-
Le Hanneur M, Maldonado AA, Howe BM, Mauermann ML, Spinner RJ (2019) “Isolated” Suprascapular Neuropathy: Compression, Traction, or Inflammation? Neurosurgery 84(2): 404-412.
-
von Knoch M, Frosch S, Baums MH, Lehmann W (2021) Motor Recovery of the Suprascapular Nerve after Arthroscopic Decompression in the Scapular Notch - a Systematic Review. Journal of Orthopedics and Trauma Surgery 159(5): 546-553.
-
Zehetgruber H, Noske H, Lang T, Wurnig C (2002) Suprascapular nerve entrapment. A meta- analysis. International Orthopaedics 26(6): 339-343.
-
Memon M, Kay J, Ginsberg L, Simunovic N, Bak K, et al. (2018) Arthroscopic management of suprascapular neuropathy of the shoulder improves pain and functional outcomes with minimal complication rates. Knee Surgery, Sports Traumatology, Arthroscopy 26(1): 240- 266.
-
Jezierski H, Wysiadecki G, Sibiński M, Borowski A, Podgórski M, et al. (2016) A quantitative study of the arrangement of the suprascapular nerve and vessels in the suprascapular notch region: new findings based on parametric analysis. Folia Morphologica 75(4): 454-459.
-
Polguj M, Rożniecki J, Sibiński M, Grzegorzewski A, Majos A, et al. (2015) The variable morphology of suprascapular nerve and vessels at suprascapular notch: a proposal for classification and its potential clinical implications. Knee Surgery, Sports Traumatology, Arthroscopy 23(5): 1542- 1548.
-
Coleman R (1995) Reducing the levels of formaldehyde exposure in gross anatomy laboratories. The Anatomical record 243(4): 531-533.
-
Eltoum I, Fredenburgh J, Myers RB, Grizzle WE (2001) Introduction to the theory and practice of fixation of tissues. J Histotechnol 24: 173-190.
-
Winsor L (1994) Tissue processing. In: Woods A, et al. (Eds.), Laboratory histopathology. Churchill Livingstone, New York, USA.
-
Kurita H, Nakanishi Y, Nishizawa R, Xiao T, Kamata T, et al. (2010). Impact of different surgical margin conditions on local recurrence of oral squamous cell carcinoma. Oral Oncology 46(11): 814-817.
-
Rutherford EE, Karanjia ND (2004) The measurement of liver resection margins. HPB : the Official Journal of the International Hepato Pancreato Biliary Association 6(1): 18-20.
-
Łabętowicz P, Synder M, Wojciechowski M, Orczyk K, Jezierski H, et al. (2017) Protective and Predisposing Morphological Factors in Suprascapular Nerve Entrapment Syndrome: A Fundamental Review Based on Recent Observations. BioMed Research International 2017: 1-10.
-
Yücesoy C, Akkaya T, Ozel O, Cömert A, Tüccar E, et al. (2009) Ultrasonographic evaluation and morphometric measurements of the suprascapular notch. Surg Radiol Anat 31(6): 409-414.
-
Park J, Su MY, Kim YU (2022) Accuracy of suprascapular notch cross-sectional area by MRI in the diagnosis of suprascapular nerve entrapment syndrome: a retrospective pilot study. Korean J Anesthesiol 75(6): 496-501.
-
Al-Redouan A, Kachlik D (2022) Suprascapular notch cross-sectional area on MRI is not highly accurate in the diagnosis of suprascapular nerve entrapment: counter point of view. Korean J Anesthesiol 75(6): 536-538.
- Pattern of Breast Lesions in Ovu Inland, Delta State, South Southern Nigeria
- Morphometric Analysis of the Human Femur: Exploring Platymetric and Robusticity Indices Among the Nigerian Population
- Anatomical Variation of Arteria Lusoria: Clinical Implications for Dysphagia Lusoria and Surgical Risk
- Morphometric Study of the Vertebral Body and Pedicle of Typical Cervical Vertebrae Using Radiological Image
- Epigenetic Mechanisms Driving Human Evolutionary Changes
- Neuroprotective Effects of Ginkgo Biloba Extract on Bilateral Common Carotid Artery Ischaemic Stroke Induced in Wistar Rat