Acute Small Bowel Obstruction Presenting as Gangrenous Jejunal Loop Secondary to Intestinal Endometriosis – A Rare Case Report
Acute intestinal obstruction is one of the few gastrointestinal symptomatology that intestinal endometriosis frequently manifests as in the reproductive age group of females. The majority of diagnosis is still laparoscopy or laparotomy with removal of affected areas for biopsy. Endometriosis affects up to 15% of menstrual women. In 3%-37% of women, endometriosis causes gastrointestinal involvement in the sigmoid colon, rectum, and terminal ileum. Proliferation and infiltration of the intestinal wall with endometriotic tissue may result in a fibrotic response with the development of strictures and adhesions, most likely as a result of the cyclical hormonal impact of menstruation. This can eventually lead to acute to recurrent abdominal pain and bowel obstruction. When it comes to identifying endometriosis, magnetic resonance imaging offers a good sensitivity (77- 93%). On immunohistochemistry (IHC) the stromal and epithelial cells are estrogen receptor (ER) positive and the stromal cells positive for CD10. This also helps in ruling out other differentials like crohn’s disease especially involving ileum with fistulae formation, acute appendicitis with phlegmon formation and in rare instance ischemic bowel disease. We hereby present a case of a 41-year-old nulliparous female with past history of ectopic pregnancy (aborted) with small bowel endometriosis who experienced severe colicky diffuse abdominal pain. Her imaging study revealed that she had multiple edematous dilated bowel loops with no peristalsis. She was hemodynamically unstable and underwent an emergency exploratory laparotomy, which revealed gangrenous jejunal loops and histopathology confirmed gangrenous small bowel with endometriosis. Post operative period was uneventful and smooth and she is on regular follow-up.
Anand Bhandary Panambur¹* and Philipose TR²
¹Department of General Surgery, Assistant Professor, A.J. Institute of Medical Sciences and Research Center, Mangalore, India ²Department of Pathology Professor and Chair, A.J. Institute of Medical Sciences and Research Center, Mangalore, India
Abbreviations
ER: Estrogen Receptor; DIE: Deep Infiltrating Endometriosis.
Introduction
Only around 10% of all overall cases of intestinal endometriosis affect the small bowel [1, 2, 3, 4]. In turn, endometriosis causes small intestinal obstruction in fewer than 7% of cases. Amongst these only 1-2 % of these cases require surgical resection [5, 6, 7, 8]. It is very much necessary to keep this as a differential diagnosis in a case of acute intestinal obstruction in females especially in females in reproductive age group. Endometriosis is defined as the presence of normal endometrial tissue located outside of the endometrial cavity and myometrium [1, 2]. It is a chronic condition that significantly reduces a patient’s quality of life. It affects 4-17% of menstrual women, with approximately 37% experiencing gastrointestinal involvement [3, 4]. Endometriosis commonly affects the ovaries, uterine ligaments, rectovaginal septum, cul-de-sac, pelvic peritoneum, colon, and appendix, in that order [1, 2, 3, 4, 5, 6, 7, 8].
Recto sigmoid is the most prevalent intestinal location of endometriosis, accounting for 50-90% of cases [5, 6, 8] followed by the small bowel, appendix, and caecum, which account for 2-16%, 3-18%, and 2-5% of cases, respectively [7, 9, 10, 11]. Exclusive ileal involvement is rare (1-7%) [9].
Wolthuis et al. state that intestinal endometriosis makes for 3–37% of intestinal cases and that the small intestine is implicated in just around 10% of all cases of intestinal endometriosis. 3 In turn, less than 7% of cases result in small intestinal obstruction brought on by endometriosis. Furthermore, surgical excision is required in less than 1% of these patients. According to Saleem et al., many studies have found that the incidence of endometriosis in the appendix ranges between 0.2% and 1.3% [12]. These figures attest to the highly uncommon clinical occurrence of endometriosis resulting in small intestinal obstruction.
We, hereby present a case of a 41-year-old nulliparous female with small bowel endometriosis who experienced severe acute colicky abdominal pain with hemodynamic instability. Her emergency imaging study (ultrasound abdomen) revealed that she had multiple edematous dilated bowel loops with no peristalsis. She underwent an emergency exploratory laparotomy, which revealed gangrenous jejunal loops followed by primary end to end jejunal anastomosis and histopathology confirmed gangrenous small bowel with endometriosis.
Case Presentation
A 41-year-old nulliparous female was referred to our surgical department with acute diffuse pain abdomen from gynecology department. On examination, she was afebrile but tachycardic with a heart rate of 110bpm, blood pressure of 90/60 mmHg and oxygen saturation of 97% on room air. She was pale, her abdomen was distended, with generalized tenderness, guarding rigidity was noted and she had sluggish bowel sounds. Ultrasound of abdomen and pelvis was performed which revealed multiple mildly dilated fluid filled bowel loops with absent peristalsis. Few of the loops showed edematous wall thickening f/s/o small bowel obstruction. Imaging also showed minimal interbowel space free fluid and bilateral pleural effusion with small loculated collections with septations in pelvic cavity. Patient had underwent left salphingectomy for ectopic pregnancy 10 yrs back. The patient’s blood workup showed a raised C-reactive protein of 42 mg/L (normal <3 mg/L) and a hemoglobin that had dropped to 6.9g/dl from 10.3g/dl, with leukocytosis (20,620/mm3) with neutrophilia (90%) and serum albumin of 2.9g/dl.
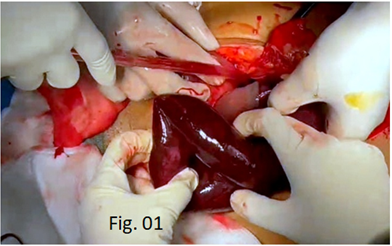
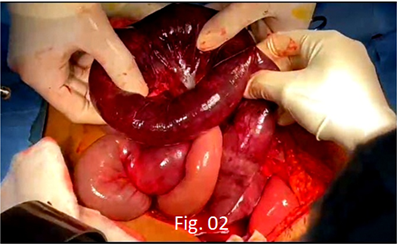
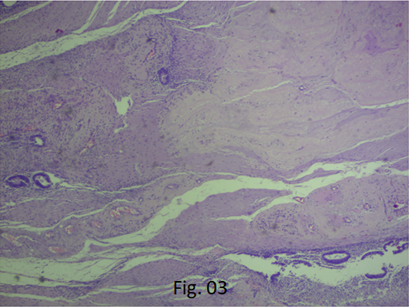
Due to unstable hemodynamic state, instead of CECT abdomen, patient underwent emergency exploratory laparotomy. Intraoperatively gangrenous jejunal segment measuring approximately 80 cms was noted with dense adhesions between the bowel loops, (Figures 1 & 2) It was about 30cms away from the DJ flexure. Resection and primary anastomosis of the remnant jejunal segment was performed and the specimen was sent for histopathological examination. Immediate postoperative period was uneventful. Patient was transfused with 2pints of PRBC and albumin infusions. Histological examination of the resected jejunum showed extensive mucosal necrosis extending up to the muscularis. Submucosa showed dilated vessels with extensive necroinflammatory infiltrate extending up to the serosa. Also showed intestinal mucosa with wall showing islands of endometrial stroma and glands. Figure 3, Resected bowel loops were consistent with the clinical diagnosis of gangrenous small bowel with endometriosis.
Discussion
The exact cause of endometriosis is yet unknown. Numerous authors and researchers have put forth various theories and hypothesis about the pathobiology of endometriosis. These theories include: (1) the Minh’s metastatic theory, which postulates that endometrial tissues spread through blood or lymphatic channels; (2) the Sampson’s regurgitation theory, wherein retrograde menstrual blood flow occurs; (3) the metaplastic development theory, which postulates that coelomic epithelium changes into endometrial tissue; and (4) recently stem cell theory, which suggests that bone marrow stem cells differentiate into endometrial tissue at unusual anatomical locations [2, 3, 4].
In our case, the likely possibility of intestinal endometriosis is due to metastatic theory and regurgitation theory mainly due to the past history of ectopic pregnancy which would have been the triggering factor and the ovarian endometrial cyst itself would have acted as a lead point in causing kinking of the intestine with its mesentry explaining the acute intestinal obstruction as a presenting feature.
Subperitoneal endometrial implants larger than 5 mm are indicative of deep infiltrating endometriosis (DIE), a severe form of endometriosis. Endometriosis of the small intestine frequently has no symptoms. When symptoms do appear, they are nonspecific and include deep pelvic pain, constipation, diarrhea, nausea, vomiting, abdominal bloating, or vague abdominal symptoms [14]. Periodic hemorrhage and endometriotic fluid leakage from the endometrial implant that penetrates the intestinal wall might result in stricture formation, fibrosis, and chronic inflammatory process [15].
The small intestine is affected by intestinal endometriosis in only around 10% of cases overall [9].
Between 7 to 23% of intestinal endometriosis cases are found to have bowel obstruction [15]. DIE impacts the mesenteric side of the serosa in the gastrointestinal tract [15]. DIE manifests as a soft-tissue mass with modest to moderate enhancement on contrast-enhanced CT imaging. 16 Only 1-2 percent of these instances necessitate surgical resection. Additionally, transmural dissemination has been noted, leading to mass formation that resembles tumors, intestinal obstruction, and rectal haemorrhage [16]. In rare cases, it can result in intestinal perforation, malignant transformation, and intussusception [16].
When endometrial deposits of the intestinal wall are suspected, diagnostic laparoscopy and biopsy remain gold standard for diagnosis [15, 16, 17]. When it comes to identifying endometriosis, magnetic resonance imaging offers a good sensitivity (77-93%) [18]. On immunohistochemistry the stromal and epithelial cells are estrogen receptor (ER) positive and the stromal cells positive for CD10. This confirms the diagnosis of DIE. Further, there are reports of Instestinal endometriosis mimicking crohn’s disease especially involving ileum with fistulae formation [19, 20, 21] acute appendicitis with phlegmon formation and in rare instance ischaemic bowel disease.
On the basis of the clinical history, endometriosis may be suspected18. Pelvic endometriosis occurs concurrently in less than 50% of patients [20]. Endometriosis causes a great deal of morbidity, including social and economic anguish, for women and their families, ranging from reproductive problems to excruciating pain. When women of reproductive age report to health facility with nebulous signs and symptoms of abdominal pain, it is crucial to maintain a high index of suspicion regarding intestinal endometriosis though it is rare [18, 19]. Women can be offered several treatment options sooner if this disease is diagnosed early in the stage of the disease [15, 16, 17]. Catastrophic clinical consequences, including in our patient’s case, small bowel resection, can be avoided with early diagnosis and management.
The surgical strategy is determined by the degree of intestinal endometriosis and its clinical manifestation. Small deposit patients may be offered medicinal care initially, followed with an elective resection. However, for big lesions producing an impending obstruction, the afflicted bowel must be removed. In order to diagnose and treat our patient, surgical management was used. In our case scenario, due the hemodynamic instability on presentation and sudden deterioration of the vitals, emergency ultrasound was performed. Clinical acumen and lab reports were also suggestive of peritonitis and hence patient underwent emergency laparotomy for the intestinal obstruction and due to financial constraints, HPE report was considered for diagnosis has it was reported by the chair of pathology and hence immunohistochemical studies were deferred.
Conclusion
Acute intestinal obstruction is one of the few gastrointestinal symptomatology that intestinal endometriosis frequently manifests as in the reproductive age group of females. The majority of diagnosis is still laparoscopy or laparotomy with removal of affected areas for biopsy, even if radiological findings can be non-specific. When a young nulliparous patient exhibits abdominal pain and intestinal obstructive symptoms, this particular diagnosis should be suspected. Endoscopic biopsies may not provide enough information for a diagnosis because endometrial tissue involves the deeper layers of the abdominal wall. It can be difficult to distinguish endometriosis from other bowel diseases such ischemic colitis or inflammatory bowel disease since it can cause a non-specific pattern of inflammation when the intestinal mucosa is affected. Magnetic resonance imaging offers a good sensitivity if the patient is hemodynamically stable at presentation and IHC can help aid in the tissue diagnosis. It is of paramount importance to keep other close differentials like Crohn’s disease, Ishaemic bowel disease, and complicated appendicitis in mind before approaching at a final clinical diagnosis.
Author Contributions
Collection of Data
Anand Bhandary Panambur
Manuscript Writing and Approval
Anand Bhandary Panambur, Thoppil Reba Philipose
Conflict of Interest Statement
The authors have no conflicts of interest to declare.
Funding Sources
The authors did not receive any funding.
References
-
Clement PB (2002) Disease of the peritoneum in Blaustein’s Pathology of the Female genital Tract. In: 5th (Edn.), Kurman RJ, (Ed.), Springer, New York, NY, USA.
-
Ellenson LH, Pirog EC (2015) The female genital tract in Robbins and Cotran Pathologic Basis of Disease. In: 9th (Edn.), Elsevier, Philadelphia, USA.
-
Vercellini P, Viganò P, Somigliana E, Fedele L (2014) Endometriosis: pathogenesis and treatment Nature Reviews. Endocrinology 10(5): 261-275.
-
Wang Y, Nicholes K, Shih IM (2020) The origin and pathogenesis of endometriosis. Annual Review of Pathology: Mechanisms of Disease 15(1): 71-95.
-
Darvishzadeh A, McEachern W, Lee TK, Bhosale P, Shirkhoda A, et al. (2016) Deep pelvic endometriosis: a radiologist’s guide to key imaging features with clinical and histopathologic review. Abdom Radiol 41(12): 2380-2400.
-
Chamié LP, Ribeiro DMFR, Tiferes DA, Macedo Neto AC, Serafini PC (2018) Atypical Sites of Deeply Infiltrative Endometriosis: Clinical Characteristics and Imaging Findings. Radiographics 38(1): 309-328.
-
Snyder BM, Beets JW, Lessey BA, Horton SRW, Abrams GA (2018) Postmenopausal Deep Infiltrating endometriosis of the colon: Rare location and novel medical therapy. Case Rep Gastrointest Med Feb pp: 9587536.
-
Teke Z, Aytekin FO, Atalay AO, Demirkan NC (2008) Crohn’s disease complicated by multiple stenoses and internal fistulas clinically mimicking small bowel endometriosis. World J Gastroenterol 14: 146-151.
-
De Ceglie A, Bilardi C, Blanch S, Picasso M, Di Muzio M, et al. (2008) Acute small bowel obstruction caused by endometriosis: A case report and review of the literature. World J Gastroenterol 14(21): 3430-3434.
-
Mussa FF, Younes Z, Tihan T, Lacy BE (2001) Anasarca and small bowel obstruction secondary to endometriosis. J Clin Gastroenterol 32: 167-171.
-
Townell NH, Vanderwalt JD (1984) Intestinal endometriosis: diagnosis and management. Br J Surg 71: 629-630.
-
Habib N, Centini G, Lazzeri L, Amoruso N, El Khoury L, et al. (2020) Bowel Endometriosis: Current Perspectives on Diagnosis and Treatment. Int J Womens Health 12: 35-47.
-
Mușat F, Păduraru DN, Bolocan A, Constantinescu A, Ion D, et al. (2023) Endometriosis as an Uncommon Cause of Intestinal Obstruction-A Comprehensive Literature Review. J Clin Med 12(19): 6376.
-
Riaz N, Khurshaidi N (2007) Acute small bowel obstruction secondary to ileal endometrioma. J Coll Phys Surg Pak 17: 228-229.
-
Mehmood S, Zhao S, Ain Q, Van Dellen J, Beggan C (2021) Endometriosis of the Small Bowel: A Diagnostic Enigma. Cureus 13(6): e15520.
-
Garg NK, Bagul NB, Doughan S, Rowe PH (2009) Intestinal endometriosis--a rare cause of colonic perforation. World J Gastroenterol 15(5): 612-624.
-
Kido A, Himoto Y, Moribata Y, Kurata Y, Nakamoto Y (2022) MRI in the Diagnosis of Endometriosis and Related Diseases. Korean J Radiol 23(4): 426-445.
-
Scarmato VJ, Levine MS, Herlinger H, Wickstrom M, Furth EE, et al. (2000) Ileal endometriosis: radiographic findings in five cases. Radiology 214: 509-512.
-
Croom RD, Donovan ML, Schwesinger WH (1984) Intestinal endometriosis. Am J Surg 148: 660-667.
-
Dang Y, Zhang S (2024) Causal relationship between endometriosis and inflammatory bowel disease: A Mendelian randomization analyses. Clin Transl Med 14(1): e1496.
-
Casiraghi S, Baggi P, Lanza P, Bozzola A, Vinco A, et al. (2018) Simultaneous Diagnosis of Acute Crohn’s Disease and Endometriosis in a Patient Affects HIV. Case Rep Gastrointest Med pp: 1509167.
- Ramsay Hunt Syndrome Presenting as Gait Imbalance without Facial Paralysis: A Case Report
- Unveiling Hidden Culprits: An Observational Study of Upper Gastrointestinal Endoscopy Findings in Symptomatic Cholelithiasis Patients
- Assessing Health Care Providers’ Proficiency in International Patient Safety Goals: A Study to Assess the Knowledge &Practice on Patient Safety in a Tertiary Care Teaching Hospital in Gujarat
- Challenges in Diagnosing Child Language Disorders
- Stunting Service Management Model in the South-Central Timor Region, East Nusa Tenggara, Indonesia
- A Single-Center, Prospective Study Focused on Quality Indicators, Success Rate, Features, Outcomes, and Indications of Endoscopic Retrograde Cholangiopancreatography (ECRP) Practice at a Tertiary Care Hospital