A Single-Center, Prospective Study Focused on Quality Indicators, Success Rate, Features, Outcomes, and Indications of Endoscopic Retrograde Cholangiopancreatography (ECRP) Practice at a Tertiary Care Hospital
Objective: To assess, in a single center-based study, the indications, results, success rates, incidence, and risk factors for complications linked to endoscopic retrograde cholangiopancreatography (ERCP) procedure and validate the ASGE/American College of Gastroenterology Task Force recommendations. Methods: We conducted a prospective analysis of all patients who underwent ERCP at tertiary care center in Mangalore, India between October 2018 and September 2023, a span of five years. ERCP was performed under sedation/ general anesthesia. Review of the patient's demographics, ERCP indications, outcomes, quality indicators, and related complications of the procedure was analyzed. Potentially relevant patient and procedure related risk factors for overall post ERCP complications were analyzed. To determine the likelihood of post-ERCP problems and post-ERCP pancreatitis (PEP) in patients with specific risk factors, such as demographic characteristics, variations in procedural procedures, pancreatic duct modifications, and others, two multivariate logistic regression models were performed. Results: A total of 948 patients were included in this study. 76.2% of naïve papilla cannulation was achieved successfully; 68% of procedures include women, 32% involve men, 84% involve benign pathology, and 26% involve suspected or confirmed malignancy. (42% women and 58% men). Suspected or confirmed choledocholithiasis was the commonest indication for an ERCP. Success rates, operative outcomes, and post-procedural complications such as hemorrhage, pancreatitis, Cholangitis, perforation were the primary outcomes of interest in our study. We also discussed the management of the failed procedures. This was followed by suspected ascending cholangitis, acute biliary pancreatitis, dysfunction of the sphincter of Oddi, and suspected malignancy. The most prevalent findings among all patients was choledocholithiasis in 43.6%, dilated duct in 35.8% and biliary stricture in 10.1%. The most common intervention was sphincterotomy, which was performed in 851 (96.8%) patients who underwent first-ever ERCP, followed by dilatation and stenting. 10.9% of the patients had post-ERCP complications, with post-ERCP pancreatitis being the commonest, followed by bleeding and cholangitis.Conclusions: In our center's ERCP procedures are carried out by experienced surgeons wellversed with endoscopic procedures who achieve good procedural outcomes, meeting the quality standards and good procedural success. Even ERCP has some morbidity and mortality risk, it is a valuable tool for addressing pancreatobiliary disease. The technical success rates met or beyond the ASGE/American College of Gastroenterology Task Force recommendations which was the main objective of this study. When compared to other centers across the country and the western world, cannulation success rates are adequate and comparable to the set norms. Since ERCP seldom results in mortality and has low rates of peri-operative complications, it is regarded as a safe interventional biliary procedure.
Paraashar R Rai¹, Anand Bhandary P²* and Anand Ignatius P³
¹Resident, A.J. Institute of Medical Sciences and Research Center, Mangalore, India ²Department of General Surgery, Assistant Professor, A.J. Institute of Medical Sciences and Research Center, Mangalore, India ³Department of General Surgery, Professor, A.J. Institute of medical sciences & Research Centre, Mangalore, India
Conclusions: In our center's ERCP procedures are carried out by experienced surgeons wellversed with endoscopic proce- dures who achieve good procedural outcomes, meeting the quality standards and good procedural success. Even ERCP has some morbidity and mortality risk, it is a valuable tool for addressing pancreatobiliary disease. The technical success rates met or beyond the ASGE/American College of Gastroenterology Task Force recommendations which was the main objective of this study. When compared to other centers across the country and the western world, cannulation success rates are adequate and comparable to the set norms. Since ERCP seldom results in mortality and has low rates of peri-operative complications, it is regarded as a safe interventional biliary procedure. Keywords: Endoscopic Retrograde Cholangiopancreatography; (ERCP); Pancreatobiliary Disease; Choledocholithiasis; Sphincterotomy; Cholangitis; ERCP Stent; Post ERCP Pancreatitis(PEP)
Abbreviations
CBD: Common Bile Duct; ASGE: American Society of Gastrointestinal Endoscopy; ESGE: European Society for Gastrointestinal Endoscopy; ERCP: Endoscopic Retrograde Cholangiopancreatography; STROCSS: Strengthening the Reporting of Cohort Studies in Surgery.
Introduction
Any endoscopic procedure intended to cannulate the pancreatic duct or the common bile duct (CBD) is referred to as an endoscopic retrograde cholangiopancreatography (ERCP) procedure. Both benign and malignant pancreatic and biliary disorders are treated using ERCP. With a steep learning curve and the potential for major, life-threatening complications, it is a technically challenging treatment. Due to its relatively high complications rates, which range from 3 to 15%, ERCP remains one of the most technically challenging therapeutic endoscopic procedures [1].
The most common indications of ERCP are removal of choledocholithiasis, relieving bile duct obstruction by stent insertion in benign and malignant strictures, drainage of pancreatic fluid collection in acute on chronic pancreatitis, Biliary or pancreatic Sphincter of Oddi dysfunctions, ampullary carcinoma in poor surgical candidates to relieve obstruction and postoperative management of biliary perioperative complications [1].
Cholangitis, perforation, hemorrhage, and pancreatitis are the important complications of the procedure [2, 3]. The most frequent complication following ERCP is pancreatitis, which can occur in 1-7% of individuals and up to 25% of high-risk patients. A small percentage of individuals may experience severe pancreatitis, which can necessitate endoscopic or surgical procedures and prolonged stay in hospital. The majority of post-ERCP pancreatitis cases are mild to moderate [4].
With time, ERCP performance is evolving into a platform for increasingly sophisticated, therapeutic, and advanced procedures such as cholangioscopy and ERCP with altered anatomy. There is a steep significant learning curve for both technical endoscopic abilities and judgment during ERCP procedures during the training period. Therefore, completing such a difficult endoscopic treatment requires the right training, experience, and competence.As a result, the American Society of Gastrointestinal Endoscopy (ASGE) released an updated list of ERCP quality markers in 2015 [5]. A set of performance metrics for pancreatobiliary endoscopy was also released by the European Society for Gastrointestinal Endoscopy (ESGE) [6].
Therefore, the aim and objective was to assess, in a single tertiary center-based study, the indications, results, success rates, incidence, and risk factors for complications linked to endoscopic retrograde cholangiopancreatography (ERCP) procedure and validate the ASGE/American College of Gastroenterology Task Force recommendations and highlight upon the inicators.
Methodology
Techniques
Following ethical approval from the Institutional Ethical Committee (IEC) and in accordance with the Declaration for good clinical practice, this study was conducted in the Department of General Surgery endoscopic unit. The endoscopy center’s audit for quality and performance indicators (Tables No 01, 02) was completed at the beginning of data entry, and the results were recorded in a predetermined proforma with reference to the following:
- Information about the facility, including the number of beds, endoscopic machines used and radiological services offered, etc.
- Organization (endoscopist count, informed consent,
- ERCP procedural room, sedation technique adopted, post-ERCP pancreatitis prevention policy, sterilization of the endoscopy equipment monitoring, etc.).
- •
- Operator attributes (education, years of experience, and the number of procedures they have completed in their career/academia)
- •
- Radiological services – available
- •
- Documentation about the ERCP performed with indications and recommendations as per the guidelines,
- 6 days a week, usually during the day; only in the presence of experienced operators
- Medical Staffing
- •
- Number of employed endoscopists =3
- •
- Number of endoscopists performing ERCP =3
- •
- Male =3
- •
- Female - None
- •
- The number of experienced operators =3
- •
- Dedicated nurses =2
- •
- Performs ERCP independently= 3
- •
- Trainee performing ERCP - None
- Characteristics of
- Center and
- Profile of
- Operators
- Hospital size
- •
- Large >1200 beds
- Hospital setting for ERCP
- •
- General Surgery unit dedicated to endoscopy with beds
- •
- Independent endoscopy service with dedicated fluoroscopic ERCP equipment inside the endoscopy unit
- Proposed Research Questions Specific To The Community Setting
- 1. How often is purely diagnostic ERCP performed in general clinical practice ?
- 2. .What are the complication rates of ERCP in general practice ?
- 3. What is the overall technical success rate of ERCP in the community setting ?
- 4. What is the utilization rate of pre - cut Sphincterotomy in the community setting ?
- 5. What is the incidence of pancreatitis, bleeding & perforation in community practice?
Table 1: ASGE 2006 Task Force on Quality in Endoscopy Proposed 11 Research Questions, with 5 of the.
Questions Specifically Directed at ERCP in the Community.
| Grade of recommendation | Measure type | Performance target % | Goal achieved, yes/no | |
|---|---|---|---|---|
| Preprocedure | ||||
| (1) Frequency with which ERCP is performed for an indication that is included in a published standard list of appropriate indications and the indication is documented | 1C+ | Process | 98 | Yes |
| (2) Frequency with which informed consent is obtained, including specific discussions of risks associated with ERCP and fully documented | 1C | Process | >98 | Yes |
| (3) Frequency with which appropriate antibiotics for ERCP are administered for settings in which they are indicated | 2B | Process | >98 | Yes |
| (4) Frequency with which ERCP is performed by an endoscopist who is fully trained and credentialed to perform ERCP | 3 | Process | >98 | Yes |
| (5) Frequency with which the volume of ERCPs performed per year is recorded per endoscopist Intraprocedural | 1C | Process | >98 | Yes |
| (6a) Frequency with which deep cannulation of the ducts of interest is documented | 1C | Process | >98 | Yes |
Table 2: Quality Indicators as per the Standard Guidelines. aPublished data from our center [7]. bPatients are asked to follow up
| (6b) Frequency with which deep cannulation of the ducts of interest in patients with native papilla without surgically altered anatomy is achieved and documented (priority indicator) | 1C | Process | 90 | Yes |
|---|---|---|---|---|
| (7) Frequency with which fluoroscopy time and radiation dose are measured and documented | 2C | Process | >98 | No |
| (8) Frequency with which common bile duct stones <1 cm in patients with normal bile duct anatomy are extracted successfully and documented | 1C | Outcome | 90 | Yes |
| (9) Frequency with which stent placement for biliary obstruction in patients with normal anatomy whose obstruction is below the bifurcation is successfully achieved and documented (priority indicator) Postprocedure | 1C | Outcome | 90 | Yes |
| (10) Frequency with which a complete ERCP report that details the specific techniques performed, accessories used, and all intended outcomes is prepared | 3 | Process | >98 | Yes |
| (11) Frequency with which acute adverse events and hospital transfers are documented | 3 | Process | > 98 | No |
| (12) Rate of post-ERCP pancreatitis (priority indicator) | 1C | Outcome | N/A | Yes |
| (13) Rate and type of perforation | 2C | Outcome | <0.2 | No |
| (14) Rate of clinically significant hemorrhage after sphincterotomy or sphincteroplasty in patients undergoing ERCP | 1C | Outcome | No | |
| (15) Frequency with which patients are contacted at or greater than 14 days to detect and record the occurrence of delayed adverse events after ERCP | 3 | Process | > 90 | No |
Table 3: Quality Indicators as per the Standard Guidelines. aPublished data from our center [7]. bPatients are asked to follow up
We conducted a prospective analysis of all patients who underwent ERCP at our tertiary care center in Mangalore, India between October 2018 and September 2023, a span of five years. ERCP was performed under general anesthesia/ sedation. Review of the patient’s demographics, ERCP indications, outcomes, quality indicators, and related complications of the procedure was analyzed. Potentially relevant patient and procedure related risk factors for overall post ERCP complications were analyzed. To determine the likelihood of post-ERCP problems and post-ERCP pancreatitis (PEP) in patients with specific risk factors, such as demographic characteristics, variations in procedural procedures, pancreatic duct modifications, and others, two multivariate logistic regression models were performed.
Patients with altered anatomy and duodenal deformity or infiltration were excluded. All procedures were carried out using Olympus Endoscopes. The Strengthening the Reporting of Cohort Studies in Surgery (STROCSS) criteria were followed when doing the study [8].
An anaesthesiologist administered midazolam with LMA to patients undergoing ERCP while they were conscious. Automated instruments were used to monitor blood pressure, heart rate, and arterial oxygen saturation. Demographics, clinical history, blood test results, technical procedures, procedural findings, diagnosis, and the kind and complications following ERCP were all included in the data. Every patient was kept under observation for a minimum of
24 to 48 hours.
Successful ERCP were defined as clearance of CBD in choledocholithiasis and CBD worm, passage of stents along the stricture with relief from jaundice in malignant and benign stricture.
Inclusion Criteria
- Age between 18 to 80 years
- Patients undergoing therapeutic ERCP
- Patients with partial CBD clearance
- Patients with all data of pre, intra and post-ERCP reports
- Patients with details record of 1-month post-ERCP follow up to recognize any
- adverse events.
Exclusion Criteria
- Age >80 years
- Refusal for consent
- Unstable vitals
- Gastric outlet obstruction
- Previous gastrojejunostomy
- Massive ascites/ Child-Pugh II/III
- On antiplatelets and anticoagulants for last 5 days
- Severe thrombocytopenia and coagulopathy.
- Insufficient data.
Statistical Analysis
A computer running Microsoft Windows was used for data analysis. After being entered into a Microsoft Excel spreadsheet, the data was checked for errors. IBM Corp.’s SPSS Statistics for Windows (issued in 2024, Version 29.0; Armonk, New York, USA) was used for statistical analysis. Frequencies and percentages were used to display categorical variables. Univariate tests were performed to examine the association of having a complication with sex, age, procedure type, class, anesthesia use, antibiotic use, and grade of difficulty. A 2-sample t test was used to assess continuous variables, while a chi square test was used to analyze categorical variables. In order to assess the independent impacts of factors, while accounting for the contribution of the other variables in the model, multivariate logistic regression was carried out, incorporating into the model those variables that were determined to be significant on univariate analysis.
Furthermore, logistic regression analyses have been performed to examine the relationship between technical success and complications and medical experience. A P value of 0.05 was deemed statistically significant for every analysis. Although it is acknowledged that Bonferroni’s method of correction [9] for multiple testing of outcome data would eliminate all findings of statistical significance, with the exception of P values of 0.001, all P values are reported uncorrected for multiple testing of data. Therefore, the results should be interpreted as preliminary and intended solely for descriptive purposes in all other cases where nominal significance is mentioned. To examine the relationship between complications and patient satisfaction, other analyses were conducted. The chi squared test, Fisher’s exact test, and analysis of variance models are among the techniques employed for these analyses.
Results
In all, 948 patients underwent 1024 ERCP procedures. Over the period of five years, from October 1, 2018, to September 30, 2023, the study included 421 (43.4%) procedures in males and 579 (56.6%) procedures in females (mean age being 57.8 years, range from 3 - 76 years). 82.5% of the patients were classified as ASA I or II, 14.3% as ASA III, and 3.2 as ASA IV, according to pre procedure risk assessment. (ASA- American Society of Anaesthesiologists) 34.6% (354) were acute procedures, while 65.4% (670) were elective procedures. 74% of the procedures were grade 1 in difficulty, 16% were grade 2, and 10% were grade 3, according to the modified Schutz score [10]. 780 patients (76.2%) had a papilla in a naive state, while 244 patients (23.8%) had a prior sphincterotomy or stent insertion (Table 3).
| Status | Total (%) no. of procedures |
|---|---|
| Naive | 780 (76.2%) |
| Previous Sphincterotomy/ stenting | 190.46 (18.6%) |
| Previous Cannulation | 34.8 (3.4%) |
| Previous failed Cannulation | 18.43 (1.8%) |
| Total | 1024 |
Table 4: Upon Endoscopy with Side Viewing Camera, the Appearance/ Status of the Papilla.
Patient Demographics
Out of 1024 patients, 10.9% (346) patients had complications. 579 were females out of which 123 showed complications versus 421 males, 156 had complications in the form of morbidity at large and mortality (Table 4).
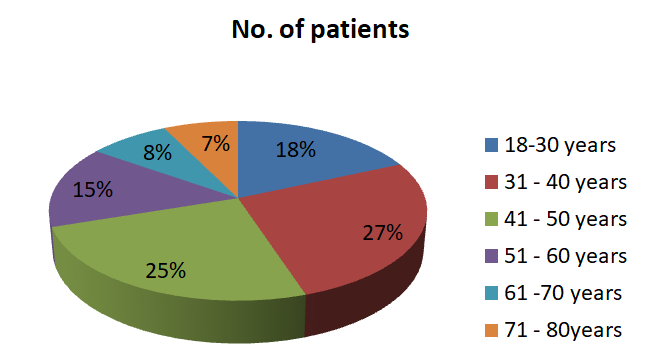
- Chart 1: Demographics as Per the Age Distribution.
- Patient Without Complications , N Patient With Complications , N p-value
- No. Of Patients
- 1024
- 346 (10.9%)
- Sex (Male/ Female)
- 421 / 579
- 156 / 123
- Ns
- Age (18-80years)
- 18- 30 yrs
- 188
- 57
- NS
- 31 – 40 yrs
- 272
- 108
- NS
- 40 – 50 yrs
- 256
- 62
- NS
- 51 – 60 yrs
- 152
- 48
- NS
- 61 – 70 yrs
- 81
- 30
- NS
- 71 – 80 yrs
- 75
- 41
- NS
- Indication For Ercp
- Choledocholithiasis
- 339
- 5
- Ns
- Suspected Malignancies
- 78
- 7
- Ns
- Pre-Cut
- 8
- 6
- <0.005
- Benign Strictures
- 95
- 8
- Ns
- Stenting
- 79
- 5
- <0.005
Table 5: Table Depicting the Patient Demographics, Indications and Clinical Significance; NS: Non Significant.
Choledocholithiasis and suspected stones were the most common indication for ERCP, accounting for 59.8% of all procedures. The other common indications are Lab and imaging suggestive of biliary disease, jaundice thought secondary to biliary malignant obstruction, stent placements for varied biliary pathologies, bile leak, gallstone/ idiopathic pancreatitis and suspected malignancies (Table 5). The most common finding was biliary stones in 446 (43.6%) procedures, with only 156 (15.2%) resulting in a normal finding (Table 6). Other ERCP findings being biliary strictures/ suspected malignancy, biliary sludge, stent removal and primary sclerozing pancreatitis.
631 patients (78.0%) underwent therapeutic treatments, while 174 patients (21.6%) underwent diagnostic procedures. 641 patients (84.8%) underwent sphincterotomy, 36 patients (4.8%) underwent pre-cut sphincterotomy, 166 patients (22.0%) received plastic bile duct stents, 42 patients (5.6%) received plastic pancreatic stents, and 56 patients (7.4%) received metallic stents.
| Indications | No. | % Of 1024 Procedures |
|---|---|---|
| Choledocholithiasis | 344 | 33.60% |
| Clinical and Biomedical or Imaging Data Suggestive of Pancreatic or Biliary Tract Disease. | 270 | 26.40% |
| Suspected Stone | 268 | 26.20% |
| Jaundice Thought Secondary to Biliary Obstruction | 152 | 14.80% |
| Stent Placement Across Strictures, Fistulae or Post Operative Bile Leak or Large Common Bile Duct Stones | 84 | 8.20% |
| Ampullary Cancer in Poor Surgical Candidates | 41 | 4% |
| Others | 29 | 2.80% |
| Pancreatitis of Unknown Etiology/ Gallstone Pancreatitis | 32 | 3% |
| Bile Leak | 25 | 2.40% |
| Signs or Symptoms Suggesting Pancreatic Malignancy When Direct Imaging is Equivocal or Normal | 16 | 1.60% |
| Pancreatic Therapeutics | 15 | 1.50% |
| Balloon Dilation of Distal Strictures | 20 | 2% |
| Stent Removal | 20 | 2% |
| Primary Sclerozing Cholangitis | 10 | 1% |
| Tissue Sampling From Pancreatic or Bile Duct | 10 | 1% |
| Pre-Operative Evaluation of Chronic Pancreatitis or Pseudocyst | 33 | 3.20% |
Table 6: Tabulation of the Overall Study Showing the Incidence of Indications for Performing ERCP and Therapeutic Intervention.
89 (90.7%) of the patients with normal bile duct anatomy had their common bile duct stones extracted successfully (less than 1 cm). Due to the fact that five patients had large stones (>10mm), four patients had concurrent strictures, and two patients were intolerant of pain, the CBD stone extraction treatment was abandoned.
Six patients had altered peri-papillary anatomy, and four individuals had inflammatory pathologies, which resulted in unsuccessful cannulation. Stricture and stone prevented the effective placement of pancreatic stents in the remaining 12 individuals with chronic pancreatitis.
| Fingings | No. | % Of 1024 Procedures |
|---|---|---|
| Biliary Stones | 446 | 43.60% |
| Dilated Duct | 367 | 35.80% |
| Normal | 156 | 15.20% |
| Biliary Strictures | 103 | 10.10% |
| Suspected Malignancies | 85 | 8.30% |
| Bile Leak | 40 | 3.90% |
| Pancreatitis | 44 | 4.30% |
| Sod Dysfunction | 25 | 2.40% |
| Primary Sclerosing Cholangitis | 10 | 1% |
| Others | 29 | 2.80% |
| Biliary Sludge | 18 | 1.8 |
| Occluded Stent | 12 | 1.20% |
| Ampullary Abnormalities | 124 | 12.10% |
| Stent Removal | 25 | 2.40% |
| Ascending Cholangitis | 8 | 0.80% |
Table 7: Tabulation showing the common finding amongst the patients undergoing ERCP.
Within 24 hours of the treatment, complications were identified; 35 patients (4.2%) experienced complications overall. The majority of patients (61, or 6%), had pancreatitis. Bleeding happened in 133 patients (13%) and cholangitis in 123 people (12%). Ten patients had perforations, two of whom had gallbladder carcinoma with involvement in the duodenum and biliary duct. 9 patients developed refractory septic shock secondary to evident ascending cholangitis, 6 patients died of pulmonary insufficiency and cardipulmonary complications, and two patients passed away within 48 hours of the procedure. These patients had concomitant metastatic disease and were at high risk for procedure/ any interventions. Twenty-seven patients experienced sedation- related complications; all of these patients were high-risk individuals with varied multiple comorbidities (Table 7).
| Complications | Total No. Of Procedures N = 1024 |
|---|---|
| Pancreatitis | 61 (6%) |
| Cholanitis | 123 (12%) |
| Perforation | 10 (1%) |
| Haemorrhage | 133 (13%) |
| Refractory Septic Shock | 9 (1.7%) |
| Aspiration(Pulmonary Insufficiency Paco2<32mmhg) & Cardiopulmonary Complications | 10 (1%) |
| Total | 346 (10.9%) |
| Mortality | 7 (0.69%) |
Table 8: Table Showing the Incidence of Complications Morbidity, Mortality Following ERCP.
Discussion
An important and diagnostic cum therapeutic procedure that is commonly used in the treatment of various pancreatobiliary pathologies is therapeutic ERCP. Although there is a chance of minor complications, ERCP is typically regarded as safe and effective. Most of the research and findings are derived from developed western nations [11]. Our objective of this literature was to provide an overview of ERCP practice in a developing nation such as India, noting success rates and complications that could be compared to previous research from developed countries with advanced centers and technology. (Rishabh Prakash Jain et.al. Procedural Outcomes Analysis of Endoscopic Retrograde Cholangiopancreatography Procedures at Tertiary Centre Hospital in South India) We evaluated 1024 patients who had therapeutic ERCPs performed at our facility for this study. In low volume centers, the ERCP success rate ranges from 76.0% to 80.3%, while in high volume centers, it ranges from 86.9% to 94.3% [12, 13, 14]. Our study’s success percentage, 86.76%, is nearly identical to earlier findings. Both benign and malignant disorders had success rates of 84.34% and 77.35%, respectively. Hilar stricture has a lower success rate than distal biliary stricture.
According to studies from academic institutions, 85.6– 98.1% of cases resulted in effective bile duct cannulation [15, 16, 17]. According to the ASGE quality statement for priority, stone removal should be less than 10 mm with normal anatomy and cannulation rates should be greater than 90%. 18 Both of the quality indicators were met in our study.
Pancreatitis is the one of the most common complications in big series following ERCP (PEP), accounting for 2% to 7% of procedures [18, 19, 20, 21, 22]. In contrast, 8–15% of procedures are linked to this complication in randomized trials, when reporting may be more reliable [23, 24]. Between 0.5 to 2% of individuals under-going ERCP experience hemorrhage [25, 26]. As anticipated, sphincterotomy or pre-cut is linked to this complication [26, 27]. Cholangitis complicates between 0.5% and 2% of ERCPs, according to the majority of large studies [28, 29]. The least frequent ERCP complication is perforation.26 According to large datasets, perforation complicates 0.1% to 1.8% of ERCPs [16, 27, 28, 29]. like the ones occurring in our case scenario in this study. The study we conducted found that our facility meets practically all ASGE procedural quality requirements.
The range of cardiopulmonary events or anesthetic complications includes catastrophic myocardial infarction, pulmonary embolism, respiratory failure, and cardiac arrest, as well as moderate, temporary hypoxia and hypotension.
Conclusions
The study found that skilled surgeons conduct ERCP successfully at high-volume centers, nearly achieving quality requirements. The study identified an unmet need to improve the quality of ERCP-related procedures, including anaesthesia techniques, microbiological surveillance, and training programs. Success requires ongoing training and skill maintenance. Therapeutic ERCP is now a highly effective and safe procedure in the hands of experienced endoscopist. The indications and success rates as well as morbidity and mortality are acceptable compared to those in earlier reports and published guidelines. In comparison to previous similar studies from the west and published guidelines, the indications, success rates, and rates of morbidity and mortality are all acceptable and within the frame work of the ASGE/ ESGE guidelines. Our findings tackle topics that have not been thoroughly examined before and, when combined with information from academic departments, offer a more comprehensive view of ERCP quality indicators.
Author Contributions
Conceptualization, writing original draft – Anand Bhandary Panambur Panambur Formal analysis, supervision and writing review – Anand Bhandary Panambur & Paraashar R Rai Compilation of relevant references and editing – Anand Bhandary Panambur & Anand Peter Ignatius
Funding Information
The authors did not receive any funding.
Conflict of Interest Statement
Authors declare that there is no conflict of interest.
References
-
Baron TH, Petersen BT, Mergener K (2006) Quality indicators for endoscopic retrograde cholangiopancreatography. Gastrointest Endosc 101: 892-897.
-
Silviera ML, Seamon MJ, Porshinsky B (2009) Complications related to endoscopic retrograde cholangiopancreaticography: a comprehensive clinical review. J Gastrointestin Liver Dis 18(1): 73-82.
-
Andriulli A, Loperfido S, Napolitano G (2007) Incidence rates of post-ERCP complications. A systematic survey of prospective studies. Am J Gastroenterol 102: 1781-1788.
-
Cotton PB, Garrow DA, Gallagher J, Romagnuolo J (2009) Risk factors for complications after ERCP: a multivariate analysis of 11,497 procedures over 12 years. Gastro Endo 70: 80-88.
-
Adler DG, Lieb JG II, Cohen J (2015) Quality indicators for ERCP. Gastrointest Endosc 81: 54-66.
-
Domagk D, Oppong KW, Aabakken L (2018) Performance measures for ERCP and endoscopic ultrasound: a European Society of Gastrointestinal Endoscopy (ESGE) Quality Improvement Initiative. United European Gastroenterol J 50: 1116-1127.
-
Kola A, Piening B, Pape UF (2015) An outbreak of carbapenem-resistant OXA-48-producing Klebsiella pneumonia associated to duodenoscopy. Antimicrob Resist Infect Control 4: 8.
-
Agha R, Abdall-Razak A, Crossley E (2019) STROCSS Group. The STROCSS 2019 guideline: strengthening the reporting of cohort studies in surgery. Int J Surg 72: 156- 165.
-
Armstrong RA (2014) When to use the Bonferroni correction. Ophthalmic Physiol Opt 34(5): 502-508.
-
Schutz SM, Abbott RM (2000) Grading ERCPs by degree of difficulty: a new concept to produce more meaningful outcome data. Gastrointest Endosc 51: 535-539.
-
Cotton PB, Lehman G, Vennes AJ (1991) Endoscopic sphincterotomy complications and their management: an attempt at consensus. Gastrointest Endosc 37: 383- 393.
-
Vitte RL, Morfoisse JJ (2007) Investigator Group of Association Nationale des Gastroenterologues des Hopitaux Generaux. Evaluation of endoscopic retrograde cholangiopancreatography procedures performed in general hospitals in France. Gastroenterol Clin Biol 31: 740-749.
-
Kapral C, Duller C, Wewalka F (2008) Case volume and outcome of endoscopic retrograde cholangiopancreatography: results of a nationwide Austrian benchmarking project. Endo 40: 625-630.
-
Coté GA, Imler TD, Xu H, Teal E, French DD, et al. (2013) Lower provider volume is associated with higher failure rates for endoscopic retrograde cholangiopancreatography. Med Care 51: 1040-1047.
-
Colton J, Colleen C, Curran MS (2009) Quality indicators, including complications, of ERCP in a community setting: a prospective study. Gastrointest Endosc 70: 457-467.
-
Williams EJ, Taylor S, Fairclough P (2007) Risk factors for complication following ERCP; results of a large−scale, prospective multicenter study. Endoscopy 39: 793-801.
-
Toros AB, Kesici B, Argun F, Gokcay S, Sari S, et al. (2013) Evaluation of Repeat ERCP: Analysis of a Four- Year Experience. J Gastroint Dig Syst 2: 116.
-
Adler DG, Lieb JG, Cohen J (2015) Quality indicators for ERCP. Gastrointest Endosc 81: 54-66.
-
Thaker AM, Mosko JD, Berzin TM (2015) Postendoscopic Retrograde Cholangiopan-creatography Pancreatitis: A Retrospective Analysis of 7,168 Cases. Pancreatology 11: 399-405.
-
Testoni PA, Testoni S, Giussani A (2011) Difficult biliary cannulation during ERCP: how to facilitate biliary access and minimize the risk of post-ERCP pancreatitis. Dig Liver Dis 43: 596-603.
-
Lohr JM, Aabaken L, Arnelo U, Gronroos J, Halttunen J, et al. (2012) How to cannulate? A survey of the Scandinavian Association for Digestive Endoscopy (SADE) in 141 endoscopists. Scandinavian Journal of Gastroenterology 47: 861-869.
-
Cotton PB, Garrow DA, Gallagher J, Romagnuolo J (2009) Risk factors for complications aft er ERCP: a multivariate analysis of 11,497 procedures over 12 years. Gastrointest Endosc 70: 80-88.
-
Andriulli A, Solmi L, Loperfido S, Leo P, Festa V (2004) Prophylaxis of ERCP-related pancreatitis: a randomized controlled trial of somatostatin and gabexate mesylate. Clin Gastroenterol Hepatol 2: 713-718.
-
Rabenstein T, Fischer B, Wiessner V, Schmidt H, Radespiel-Troger M, et al. (2004) Low molecular weight heparin does not prevent acute post-ERCP pancreatitis. Gastrointest Endosc 59: 606-613.
-
Lal D, Lane M, Wong P (2003) Complications of endoscopic retrograde cholangiopancreatography. N Z Med J 116(1177): U496.
-
Gomez Ponce RL (2002) Early complications of endoscopic retrograde cholangiopancreato-graphy performed January 1998 to December 2000 in Peru. Rev Gastroenterol Peru 22: 33-43.
-
Kuran S, Parlak E, Oguz D, Cicek B, Disibeyaz S, et al. (2006) Endoscopic sphincterotomy-induced haemorrhage: treatment with heat probe. Gastrointest Endosc 63: 506-511.
-
Siegman-Igra Y, Spinrad S, Rattan J (1988) Septic complications following endoscopic retrograde cholangiopancreatography: the experience in Tel Aviv Medical Centre. J Hosp Infect 12: 7-12.
-
Byl B, Deviere J, Struelens MJ, Roucloux I, De Coninck A, et al. (1995) Antibiotic prophylaxis for infectious complications after therapeutic endoscopic retrograde cholangiopancreatography: a randomized, double-blind, placebo-controlled study. Clin Infect Dis 20: 1236-1240.
- Ramsay Hunt Syndrome Presenting as Gait Imbalance without Facial Paralysis: A Case Report
- Unveiling Hidden Culprits: An Observational Study of Upper Gastrointestinal Endoscopy Findings in Symptomatic Cholelithiasis Patients
- Assessing Health Care Providers’ Proficiency in International Patient Safety Goals: A Study to Assess the Knowledge &Practice on Patient Safety in a Tertiary Care Teaching Hospital in Gujarat
- Challenges in Diagnosing Child Language Disorders
- Stunting Service Management Model in the South-Central Timor Region, East Nusa Tenggara, Indonesia
- Acute Small Bowel Obstruction Presenting as Gangrenous Jejunal Loop Secondary to Intestinal Endometriosis – A Rare Case Report