Ramsay Hunt Syndrome Presenting as Gait Imbalance without Facial Paralysis: A Case Report
Ramsay Hunt Syndrome (RHS) is the reactivation of a Varicella Zoster Virus (VZV) infection affecting the geniculate ganglion and is also known as Herpes Zoster Oticus. It is clinically diagnosed with a classical triad of ipsilateral facial paralysis, otalgia, and vesicular rash near the ear and auditory canal. It is not always necessary to have the classical triad, and it can also present atypically without facial nerve palsy, with variants such as Zoster sine herpete. We are presenting a case of Ramsay hunt syndrome with no facial paralysis but with an atypical presentation of gait imbalance, who had a vesicular rash around the ear a week before presentation. He was started on steroids and valacyclovir after confirmation of diagnosis, with which his symptoms improved drastically. Maintaining a high index of clinical suspicion is crucial for diagnosing the syndrome, particularly when it presents without the classic triad of symptoms. The potential involvement of adjacent cranial nerves should also be considered, and a low threshold for suspicion facilitates early diagnosis and treatment, helping to prevent long-term, irreversible complications.
Abbreviations
RHS: Ramsay Hunt Syndrome; VZV: Varicella Zoster Virus; CT: Computed Tomography; MRI: Magnetic Resonance Imaging; ELISA: Enzyme-Linked immunosorbent Assay.
Introduction
Ramsay Hunt Syndrome, named after American neurologist James Ramsay Hunt during the World War I era, is also known as geniculate ganglion herpes zoster or herpes zoster oticus [1]. It is a late complication of varicella zoster virus infection, resulting in inflammation of the geniculate ganglion of the seventh cranial nerve [2]. It usually presents with the classic triad of ipsilateral facial paralysis, otalgia, and vesicular rash, but can also exhibit significant variability in its presentation. Commonly seen in people over the age of 60, occurring in 5 out of 100,000 people in a year. 12% of patients develop facial palsy, and it is important to know the atypical presentation as well, especially when adjacent cranial nerves can be involved [3]. We are reporting a case of Ramsay Hunt syndrome in an immunocompetent patient who presented with vesicular rash and gait imbalance and aim to inform clinicians regarding the atypical presentation and management of RHS to prompt early diagnosis and treatment to prevent long-term complications in elderly patients.
Case Report
An elderly man in his 80’s with a known past medical history of atrial fibrillation on Eliquis and flecainide and essential hypertension presented to the emergency department with gait imbalance. He has been feeling off balance and having difficulty walking, which started a few days before the presentation. He was also diagnosed with shingles on his left side of his ear and face a few weeks ago and completed his antiviral medication, which resolved at the time of presentation. He had associated double vision when both eyes were open, but it resolved with either of them closed. His images were stacked on each other.
Patient denied any tinnitus or ringing in the ear or hearing loss, or any upper respiratory infection symptoms. Patient denied any fall or trauma. On physical examination, he was alert and oriented x 3, pupillary light reaction was normal within limits bilaterally, and ears, nose, and throat were grossly symmetric. On neurological exam, he was alert and oriented with speech fluency, no dysarthria or aphasia, and cranial nerves were intact, with the power 5 out of 5 in both upper and lower extremities bilaterally. Normal tone noted in the bilateral upper and lower extremities with no abnormal movements noted. Reflexes were 2+ bilaterally. On sensory exam, he lacked bilateral upper and lower extremity sensation for light touch, but proprioception was diminished in the lower extremities. His coordination was intact; finger- to-nose and heel-to-shin were intact bilaterally, with no truncal ataxia noted.
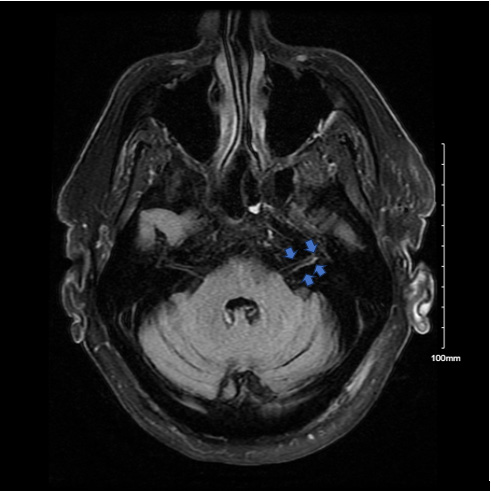
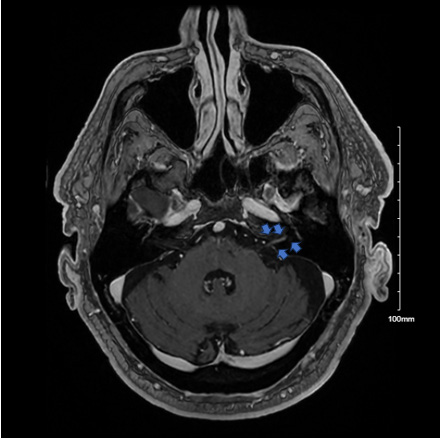
His vitals were stable on admission, and initial laboratory workup up including complete blood count and complete metabolic profile, urine analysis, were normal. TSH was also normal. Given his significant diplopia and gait imbalance, a Computed Tomography (CT) scan of the head followed by CT angio head and neck with and without contrast, with postprocessing was done, which showed no flow-limiting stenosis, branch occlusion, aneurysm, or vascular malformation. Magnetic Resonance Imaging (MRI) brain without contrast was done, which showed no acute intracranial infarct or hemorrhage. He completed treatment with valacyclovir and a short course of prednisone for his shingles. Vitamin B12, folic acid, and Vitamin D levels were normal. The neurology team was consulted and performed a lumbar puncture, which showed a total cell count of 100, with 4% neutrophils, 87% lymphocytes, 9% monocytes, and a total nucleated cell count was 18 cells per mm3. Cerebrospinal fluid (CSF) protein was 59 (normal range 12-60 mg/dL, glucose was 75 (normal range 40-70 mg/ dl), and cultures showed no growth. CSF samples were sent for the meningitis panel, as mentioned in Table 1, and were negative. Other CSF studies included CSF VDRL, CSF Herpes simplex PCR, and West Nile virus were negative, but IGM varicella zoster was positive, and IgG was negative. Cytology was negative as well. Neurology recommended MRI brain and internal auditory canal with and without contrast, which showed findings suspicious for Ramsay- Hunt syndrome with abnormal enhancement of the left 7th and 8th cranial nerves as well as the left external ear and periauricular soft tissues, as shown in Figures 1 & 2. MRI also showed a 7 mm presumed meningioma along the left tentorial leaflet. Neurosurgery was consulted for a left tentorial leaflet meningioma and recommended no intervention. Neurology team confirmed the diagnosis of Ramsay hunt syndrome in the setting of diplopia and left temporal nerve pain, IgM positive Herpes Zoster CSF fluid, and started on 21-day course of Valacyclovir 2000 mg tid and 7 days of prednisone 60 mg with no taper. His gait imbalance has improved since steroids were started.
Follow-up outpatient neurology appointments showed improvement in his gait and back to baseline after therapy sessions. Follow-up MRI brain showed no enhancement of the cranial nerves.
Discussion
Ramsay Hunt syndrome (RHS) is caused by the Varicella Zoster virus (VZV), which belongs to the human herpesvirus family. Varicella zoster is a double-stranded DNA virus and specifically belongs to human alpha herpes virus 3 [4]. VZV causes chicken pox and is spread by respiratory droplets in the acute phase. Once the infection has resolved, the virus remains latent in the cranial nerves or dorsal root ganglia and subsequently gets reactivated during times of stress or immunocompromised states. When the virus reactivates, it causes a vesicular rash in the distribution of the nerve in which it has been dormant, causing shingles. In Ramsay Hunt syndrome, the virus primarily reactivates along the facial nerve, in which it remained dormant, causing facial paralysis, but it can also involve other cranial nerves [2].
Ramsay Hunt syndrome can affect both immunocompetent and immunocompromised patients and has an incidence of 5 per 100,000 people per year [3]. It accounts for 7% of facial paralysis and 30% accounts for zoster sine herpete, which is another variant of Ramsay hunt with ear pain and facial weakness [5].
Commonly affects patients in their 7th and 8th decades, and men and women are equally affected [6].
Typically presents with the classic triad of ipsilateral facial paralysis, otalgia, and painful vesicles on the ear. It involves a characteristic rash which correlates with the areas of innervation by the facial nerve, involving the ear, concha bowl, anti-helix, and post auricular sulcus, but can also involve the auditory canal, scalp, cheek, tongue, or palate [7]. It can have a prodrome of pain, headache, fever, and fatigue, followed by facial paralysis, which is seen typically in 1-3 days of onset of the rash.
Ramsay Hunt syndrome is a clinical diagnosis, and laboratory testing lacks sensitivity. Culture can be obtained from vesicular fluid, blood, saliva, or tears, and PCR testing has a sensitivity of 58%. Enzyme-linked immunosorbent Assay (ELISA) testing has a high sensitivity of around 82- 99% but has limited utility in an acute setting [5]. MRI can show inflammation of the geniculate ganglion of the affected facial nerve, but CT does not contribute to diagnosis. Most cases of Ramsay Hunt can be diagnosed clinically and usually don’t need much workup; our case had an atypical presentation with gait imbalance, which prompted us to carry out an extensive diagnostic workup. Several case reports in the literature describe atypical presentations of Ramsay Hunt Syndrome. For example, Chou et al. reported a patient who presented with a fear of falling, while Thioub et al. documented a case without facial palsy. Nishizawa et al. described a patient who had no skin rash, and Maruyama et al. reported a case where the rash appeared in the oral cavity rather than the typical location in the ear [8, 9, 10, 11]. Additionally, a literature review by Di Berardino et al. found that atypical presentations are more frequently observed following stapedectomy. These findings underscore the importance of clinician awareness regarding atypical forms of the syndrome to ensure timely diagnosis and treatment [12].
Treatment of RHS involves antivirals and steroids, given mainly to decrease the long-term complications. Acyclovir, valacyclovir, and famciclovir have been noticed to be effective and used at the dosing of 500 mg five times a day, which is more affordable than others. Valacyclovir is used at 1000 mg three times a day, famcylcvior at 500 mg three times a day. The duration of treatment is usually 7 to 10 days; however, there have been studies that showed continuing therapy for 21 days, as there could be prolonged and delayed degeneration of facial nerve axons up to 21 days [13]. High- dose corticosteroids are co-administered with antiviral treatment and can be given IV or orally. Usually prednisone at 1 mg/kg/day up to a maximum of 60 mg per day is prescribed and followed by taper to prevent adrenal insufficiency. Complications include pain, rash, facial paralysis, hearing loss, tinnitus, vertigo, and corneal abrasion are usually short-term, and long-term complications mostly include postherpetic neuralgia, scarring, and depression and anxiety from loss of facial function. Prognostically, information on the extent of nerve involvement can be obtained via electrodiagnostic testing like electroneuronography and electromyography.
In conclusion, RHS not only presents as rash, facial paralysis, and ear pain but can also have other variants of presentation, including gait imbalance, as seen in our case. In older adults who are commonly affected and with their increased risk of falls, a low threshold of suspicion is essential when prodromal symptoms are present. Early diagnosis and management can prevent both short and long- term complications in this disease condition, as initiation of treatment resolves most of the deconditioning symptoms in this age group.
| Component | |
|---|---|
| E COLI K1, CSF | Not Detected |
| Haemophilus Influenzae, CSF | Not Detected |
| Listeria Monocytogenes, CSF | Not Detected |
| Neisseria Meningitidis, CSF | Not Detected |
| Comment: Only Encapsulated Strains Of N. Meningitidis Will Be Detected By The Biofire ME Panel. Unencapsulated N. Meningitidis Will Not Be Detected. | |
| Streptococcus Agalactiae, CSF | Not Detected |
| Streptococcus Pneumoniae, CSF | Not Detected |
| Cytomegalovirus, CSF | Not Detected |
| Enterovirus, CSF | Not Detected |
| Herpes Simplex Virus 1, CSF | Not Detected |
| Comment: Dedicated Herpes Simplex Virus 1 & 2 (HSV-1 & HSV-2) Nucleic Acid Amplification Testing Of Cerebrospinal Fluid (CSF) Is Recommended For Patients With Suspected CNS HSV Infection. | |
| Herpes Simplex Virus 2, CSF | Not Detected |
| Comment: Dedicated Herpes Simplex Virus 1 & 2 (HSV-1 & HSV-2) Nucleic Acid Amplification Testing Of Cerebrospinal Fluid (CSF) Is Recommended For Patients With Suspected CNS HSV Infection. | |
| Human Herpesvirus 6, CSF | Not Detected |
| Human Parechovirus, CSF | Not Detected |
| Varicella Zoster Virus, CSF | Not Detected |
| Cryptococcus Neoformans/Gattii, CSF | Not Detected |
| Comment: Cryptococcal Antigen Testing Of Cerebrospinal Fluid (CSF) With Titer For Positives Is Recommended For Immunocompromised Patients With Suspected CNS Cryptococcal Infection. |
Table 1: Meningitis Panel of Cerebrospinal Fluid Sample.
Acknowledgements
None
Informed Consent
Verbal informed consent obtained from the patient
References
-
Sweeney CJ, Gilden DH (2001) Ramsay Hunt syndrome. J Neurol Neurosurg Psychiatry 71(2): 149-154.
-
Paiva ALC, Araujo JLV, Ferraz VR, Veiga JCE (2017)
-
Murakami S, Hato N, Horiuchi J, Honda N, Gyo K, et al. (1997) Treatment of Ramsay Hunt syndrome with acyclovir-prednisone: significance of early diagnosis and treatment. Ann Neurol 41(3): 353-357.
-
Al-Turab M, Chehadeh W (2018) Varicella infection in the Middle East: Prevalence, complications, and vaccination. J Res Med Sci 23: 19.
-
Lee HY, Kim MG, Park DC, Park MS, Byun JY, et al. (2012) Zoster sine herpete causing facial palsy. Am J Otolaryngol 33(5): 565-571.
-
Van Le M (2012) Image diagnosis: Ramsay Hunt syndrome. Perm J 16(4): 51-52.
-
Ostwal S, Salins N, Deodhar J, Muckaden MA (2015) Management of Ramsay Hunt syndrome in an acute palliative care setting. Indian J Palliat Care 21(1): 79-81.
-
Chou CC, Lo YT, Su HC, Chang CM (2022) Fear of falling as a potential complication of Ramsay Hunt syndrome in older adults: a case report. BMC Geriatr 22(1): 901.
-
Thioub D, Ibrahim AT, Mbaye KD, Jules ZY, Lakhe NA, et al. (2023) Atypical presentation of Ramsay Hunt syndrome without facial palsy in an immunocompetent Senegalese adult patient. Case Rep Clin Med 12(7): 218-222.
-
Nishizawa T, Ishikawa K, Matsuo T, Higuchi N, Ishiguro K, et al. (2021) Atypical Ramsay Hunt syndrome (zoster sine herpete) with otitis media. J Gen Fam Med 22(6): 344-346.
-
Maruyama S, Ichimura N, Wakayama Y, Omori M, Sakaguchi K, et al. (2025) Disseminated herpes zoster presenting as atypical Ramsay-Hunt syndrome with oral lesions: A case report. Journal of Oral and Maxillofacial Surgery, Medicine, and Pathology.
-
Di Berardino F, Zanetti D (2018) Typical or Atypical Ramsay-Hunt Syndrome in Delayed Facial Palsy After Stapedectomy? J Int Adv Otol 14(2): 233-238.
-
Coulson S, Croxson GR, Adams R, Oey V (2011) Prognostic factors in herpes zoster oticus (Ramsay Hunt syndrome). Otol Neurotol 32(6): 1025-1030.
- Unveiling Hidden Culprits: An Observational Study of Upper Gastrointestinal Endoscopy Findings in Symptomatic Cholelithiasis Patients
- Assessing Health Care Providers’ Proficiency in International Patient Safety Goals: A Study to Assess the Knowledge &Practice on Patient Safety in a Tertiary Care Teaching Hospital in Gujarat
- Challenges in Diagnosing Child Language Disorders
- Stunting Service Management Model in the South-Central Timor Region, East Nusa Tenggara, Indonesia
- Acute Small Bowel Obstruction Presenting as Gangrenous Jejunal Loop Secondary to Intestinal Endometriosis – A Rare Case Report
- A Single-Center, Prospective Study Focused on Quality Indicators, Success Rate, Features, Outcomes, and Indications of Endoscopic Retrograde Cholangiopancreatography (ECRP) Practice at a Tertiary Care Hospital