Unveiling Hidden Culprits: An Observational Study of Upper Gastrointestinal Endoscopy Findings in Symptomatic Cholelithiasis Patients
Background: Cholelithiasis, commonly known as gallstone disease, is often managed surgically through cholecystectomy. However, many patients continue to experience persistent gastrointestinal symptoms post-surgery, raising questions about hidden upper GI pathologies that may mimic gallstone-related discomfort. Could these overlooked conditions be the true culprits behind lingering symptoms? Aim & Objectives: 1. to analyze the role of upper gastrointestinal endoscopy (UGIE) as a routine pre-operative investigation in cholelithiasis patients with typical biliary colic or atypical upper abdominal symptoms undergoing elective cholecystectomy.2.to find out co existing pathologies in symptomatic cholelithiasis patients. Methods: An observational study was conducted on 80 patients diagnosed with symptomatic cholelithiasis. All patients un derwent preoperative UGIE to assess for associated GI abnormalities. The findings were analyzed and correlated with symp tom presentation, demographic factors, and postoperative outcomes. Statistical Analysis: Descriptive statistics were used to analyze the prevalence of pathological upper gastrointestinal endos copy (UGIE) findings, including gastritis, hiatus hernia, peptic ulcer disease, polyps, and malignancy, expressed as percentages. Data were recorded and processed using Microsoft Excel for preliminary analysis. The Chi-square test was applied to assess the association between the type of pain (typical vs. atypical) and endoscopic findings. Statistical analysis was conducted us ing IBM SPSS Statistics (Version 27), with significance level set at 0.05 for all tests. Results: This prospective study was conducted at a tertiary care medical college hospital in Mangalore, Karnataka, India. It in cluded 80 patients diagnosed with gallbladder stones via ultrasound, who subsequently underwent upper gastrointestinal en doscopy (UGIE) to evaluate coexisting GI pathology. UGIE detected abnormalities in a significant proportion of patients, with gastritis being the most prevalent finding, followed by reflux esophagitis and peptic ulcer disease. A subset of patients tested positive for Helicobacter pylori infection. Notably, patients with abnormal UGIE findings had a higher incidence of persistent postoperative symptoms compared to those with normal UGIE results. The study observed a higher prevalence of gallstones in females compared to males, with a female-to-male ratio of 1:0.45. Gallstones were more commonly found in individuals over 40 years of age, with the majority of female patients being above 60 years. A subset of patients with inflammatory GI pathology tested positive on the rapid urease test and were treated with an H. pylori eradication regimen, leading to symptom improve ment. Furthermore, upper GI abnormalities were more frequently observed in patients with a single gallstone compared to those with multiple calculi. Additionally, all patients with a normal UGIE had a normal gallbladder wall thickness. This study highlights the importance of evaluating upper GI pathology in patients with gallstones to optimize management and improve postoperative outcomes. Conclusion: This study highlights the critical role of upper gastrointestinal endoscopy (UGIE) in the preoperative evaluation of symptomatic cholelithiasis. Findings suggest that gastrointestinal inflammatory conditions, rather than gallstones, are of ten the primary cause of symptoms. Laparoscopic cholecystectomy should be deferred until after GI treatment; if symptoms resolve, surgery may not be needed.
Anand Bhandary Panambur*¹, Anand Peter Ignatius² and Rahul R Shenoy³
¹Department of General Surgery, Assistant Professor, A.J. Institute of Medical Sciences and Research Center, Mangalore, India ²Professor A.J. Institute of Medical Sciences and Research Center, Mangalore, India ³Resident, Department of General Surgery, A.J. Institute of medical sciences & Research Centre, Mangalore, India
postoperative symptoms compared to those with normal UGIE results. The study observed a higher prevalence of gallstones in females compared to males, with a female-to-male ratio of 1:0.45. Gallstones were more commonly found in individuals over 40 years of age, with the majority of female patients being above 60 years. A subset of patients with inflammatory GI pathology tested positive on the rapid urease test and were treated with an H. pylori eradication regimen, leading to symptom improve ment. Furthermore, upper GI abnormalities were more frequently observed in patients with a single gallstone compared to those with multiple calculi. Additionally, all patients with a normal UGIE had a normal gallbladder wall thickness. This study highlights the importance of evaluating upper GI pathology in patients with gallstones to optimize management and improve postoperative outcomes. Conclusion: This study highlights the critical role of upper gastrointestinal endoscopy (UGIE) in the preoperative evaluation of symptomatic cholelithiasis. Findings suggest that gastrointestinal inflammatory conditions, rather than gallstones, are of ten the primary cause of symptoms. Laparoscopic cholecystectomy should be deferred until after GI treatment; if symptoms resolve, surgery may not be needed. Keywords: Gallstones; Cholelithiasis; Ugi Endoscopy (Ugie); Laparoscopic Cholecystectomy; Minimal Access Surgery; H.Pylori; Post Cholecystectomy Syndrome; Observational Study
Abbreviations
PCS: Post-Cholecystectomy Syndrome; GI: Gastrointestinal; PUD: Peptic Ulcer Disease; GERD: Gastroesophageal Reflux Disease; UGE: Upper GI Endoscopy; RAT: Rapid Urease Test; PPIs: Proton Pump Inhibitors.
Introduction
Gallstones, also referred to as cholelithiasis, are among the most common conditions encountered in surgical practice [1, 2]. It is estimated that approximately 5–10% of the Asian population is affected by gallstones. In the Asian subcontinent, cholelithiasis is more prevalent in females and individuals over the age of 40 [3, 4]. In contrast, gallbladder disease affects approximately 15–16.6% of females and 5–7.9% of males in Western countries [5, 6, 7, 8]. Risk factors for gallstone formation include obesity, high-fat diet, sedentary lifestyle, genetic predisposition, and metabolic disorders such as diabetes mellitus and hyperlipidemia [9, 10].
Over the past few years, there has been an increase in the diagnosis of gallstones due to changes in dietary habits, widespread use of imaging technology for abdominal evaluations, and greater awareness among the general population regarding various diseases [2, 8]. The primary mode of management for symptomatic gallstones is cholecystectomy [11]. Approximately 85–90% of patients with symptomatic cholelithiasis experience significant symptom relief following gallbladder removal. However, a subset of patients continues to experience persistent symptoms postoperatively, a condition referred to as post-cholecystectomy syndrome (PCS) [12].
Research indicates that underlying upper gastrointestinal (GI) pathology is often responsible for these persistent symptoms. Studies have shown that in patients who underwent cholecystectomy but had no stones detected intraoperatively, the incidence of persistent symptoms post-surgery was as high as 40% [13, 14, 15].
Although laparoscopic cholecystectomy is a routine procedure, it is not without risks. The procedure requires general anesthesia, which carries its own risks and complications. Additionally, the creation of pneumoperitoneum during surgery places a burden on the cardiopulmonary system, particularly in patients with pre-existing cardiac or respiratory conditions [16, 17]. The procedure itself is associated with complications such as bile duct injury, bleeding, infection, and postoperative adhesions, which can contribute to long-term morbidity [18, 19].
Identifying patients with concurrent upper GI pathology and treating them prior to surgery could reduce the number of unnecessary cholecystectomies. This is particularly important because upper GI symptoms often mimic those of biliary tract disease [20, 21]. Gastritis, reflux esophagitis, and peptic ulcer disease are common upper GI conditions that can present with symptoms similar to gallstone disease, such as epigastric pain, bloating, nausea, and dyspepsia [22]. Helicobacter pylori infection is frequently implicated in these conditions, and its eradication has been shown to significantly improve symptoms in affected patients [23].
The coexistence of upper GI disorders in patients with gallstone disease may contribute to PCS [24, 25].
Although gallstone disease is asymptomatic in the majority of individuals, cholecystectomy is frequently regarded as the best treatment for symptomatic cases. However, accurately determining whether gallstones are the true cause of a patient’s symptoms remains a challenge [26]. Several studies have demonstrated that patients who experience persistent symptoms following cholecystectomy often have findings on upper GI endoscopy [27, 28]. Treatment of these underlying GI conditions has been shown to alleviate dyspeptic symptoms and pain after surgery [29, 30]. Upper GI pathologies are frequently the actual cause of symptoms that are mistakenly attributed to gallbladder disease [15–20].
Given the overlap in symptoms between gallstone disease and upper GI disorders, preoperative upper GI evaluation, including endoscopy, should be considered in selected patients. This approach may help in avoiding unnecessary surgeries and improving patient outcomes by addressing the actual underlying pathology. Many patients present with persistent dyspeptic symptoms after cholecystectomy, highlighting the need for a thorough evaluation of these symptoms. This study was undertaken to assess the prevalence of concurrent upper GI pathology in patients with gallstone disease and to determine whether targeted treatment of these conditions could improve symptom relief, potentially reducing the need for unnecessary surgical intervention.
Materials and Method
The study was conducted in the Department of General Surgery at A J Institute of Medical Sciences and Research Centre, Mangalore. It was designed as an observational study and was carried out over a period of two years, from August 2022 to July 2024. The study utilized purposive sampling, and the sample size was determined based on a study conducted by H. Diettrich et al.,31 with a minimum requirement of 80 subjects.
Inclusion Criteria
- Patients above 18 Years Of Age
- Radiologically proven diagnosis Of Cholelithiasis
- Patients with Typical or Atypical symptoms of Cholelithiasis
Exclusion Criteria
- Patients < 18 Years of Age
- Acute abdomen
- Choledocholithiasis
- Surgical Obstructive Jaundice
- Gall Bladder stone pancreatitis
- Gall Bladder neoplasm
- Previous Gall Bladder or Pancreatic surgery
- All congenital anomalies of biliary duct system recorded incidentally or accidentally even if gall bladder stones are present. Criteria for Deferring Laparoscopic Cholecystectomy in Patients with Concurrent Upper GI Pathologies 1. Active Peptic Ulcer Disease (PUD)
- Recent upper GI bleeding (within the past 4 weeks).
- Presence of ulcer-related perforation or gastric outlet obstruction.
2. Gastroesophageal Reflux Disease (GERD)
- Los Angeles (LA) Grade C or D esophagitis.
- Presence of Barrett’s esophagus with high-grade dysplasia.
3. Large Hiatal Hernia (>5 cm) or Paraesophageal Hernia
- Symptomatic paraesophageal hernia requiring repair.
- Severe reflux or regurgitation with significant dysphagia.
4. Acute Upper GI Bleeding
- Hemodynamic instability.
- Recent transfusion requirement for ongoing bleeding.
5. Unexplained Gastric Mass • Suspicious gastric mass detected on endoscopy, awaiting biopsy results.
Method of Data Collection
This prospective study included approximately 80 patients diagnosed with symptomatic gallbladder stones, either clinically or radiologically, in the Department of General Surgery at A J Institute of Medical Sciences and Research Centre. Verbal and written informed consent was obtained from all participants. Patient data included demographic details, presenting symptoms (typical or atypical biliary colic), ultrasonography findings, upper GI endoscopy (UGE) results, and biopsy reports when applicable. After clinical evaluation, all patients underwent UGE a few days before surgery. If necessary, biopsies were taken for histopathological examination.
Endoscopic findings were categorized as normal, infective, inflammatory, erosive, ulcerative, or malignant. Patients with ulcers underwent biopsy and H. pylori testing via the rapid urease test (RAT). H. pylori-positive cases were treated with a triple eradication regimen, while other ulcers were managed with proton pump inhibitors (PPIs) for four weeks. Patients with gastric or duodenal inflammation were started on PPI therapy before undergoing laparoscopic cholecystectomy. Patients with malignant findings on endoscopy did not proceed with cholecystectomy but were further evaluated and managed based on tumor staging.
Statistical Analysis
Descriptive statistics were used to analyze the distribution of pathological UGE findings, including gastritis, hiatus hernia, peptic ulcer disease, polyps, and malignancy, and were expressed as percentages. Categorical variables were compared using the Chi-square test or Fisher’s exact test, as appropriate. Continuous variables were analyzed using the independent t-test or Mann-Whitney U test, depending on the normality of distribution assessed by the Shapiro-Wilk test. All data were recorded in Microsoft Excel and analyzed using IBM SPSS Statistics version 27. A p-value <0.05 was considered statistically significant.
Results and Observations
The present study was done at a teaching hospital on 80 cases that met predefined criteria and gave an informed consent for the study demographic data. The findings of the study are discussed below.
Demographic Data
| Age | Case No | Percent |
|---|---|---|
| 18-20 years | 1 | 1.25% |
| 21-30 years | 7 | 8.75% |
| 31-40 years | 15 | 18.75% |
| 41-50 years | 21 | 26.25% |
| 51-60 years | 18 | 22.50% |
| 61-70 years | 12 | 15.00% |
| more than 70 years | 6 | 7.50% |
Table 1: Age Group.
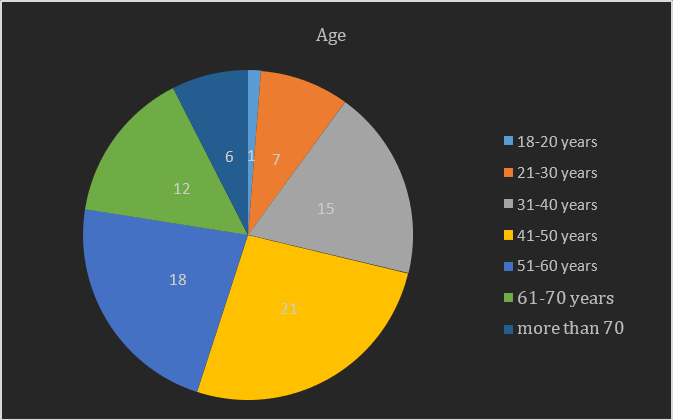
Graph 1: Age Group.
1 case (1.25%) belonged to the age group between 18 years and 20 years ,7 case (8.75%) belonged to the age group between 21 years and 30 years , 15 cases (18.75%) belonged to the age group between 31 years and 40 years , 21 cases (26.25%)belonged to the age group between 41 years and 50 years ,18 cases (22.50%) belonged to the age group between 51 years and 60 years , 12 cases(15%) belonged to the age group between 61 years and 70 years and 6 cases (7.5%)belonged to the age group more than 70 years the mean age was 50.76b years SD + 15.27 years.
Gender Distribution
| Gender | Frequency | Percentage |
|---|---|---|
| male | 25 | 31.25% |
| female | 55 | 68.75% |
| Total | 80 | 100.00% |
Table 2: Table Depicting the Gender Distribution.
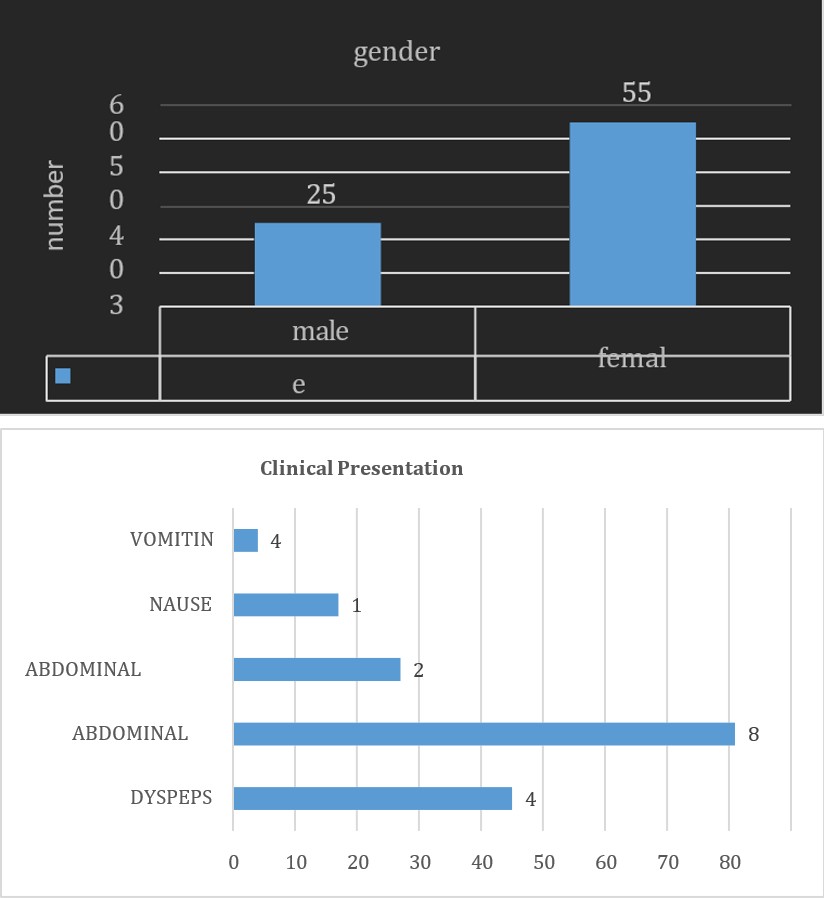
Graph 2: Pie Diagram Depicting the Gender Distribution.
68.75% were females and 31.75% were males, the male to female ratio was 0.45 to 1 .The difference in gender was
Clinical Details
statistically significant with the P value 0.032.
| Clinical Presentation | Frequency | Percent |
|---|---|---|
| Dyspepsia | 45 | 56.25% |
| Abdominal Pain | 81 | 100.00% |
| Abdominal Bloating | 27 | 33.75% |
| Nausea | 17 | 21.25% |
| Vomiting | 4 | 5.00% |
Table 3: Table Depicting the Distribution of Clinical Presentation.
Graph 3: Coloum Bar Diagram Depicting the Distribution of Clinical Presentation.
In the order of frequency of symptoms abdominal pain was seen in 80 cases (100.00%) , dyspepsia was seen 45 cases (56.25%) , abdominal bloating was seen 27 cases (33.75%), nausea was seen 17 cases (21.25%) , vomiting was seen 4 cases (25%).
Pre-Existing Co-Morbidities
| Pre-Existing Co Morbidities | Frequency | Percentage |
|---|---|---|
| Diabetes Mellitus | 23 | 28.40% |
| Hypertension | 18 | 22.22% |
| Hypothyroidism | 11 | 13.58% |
Table 4: Table Depicting the Pre-Existing Co Morbidities.
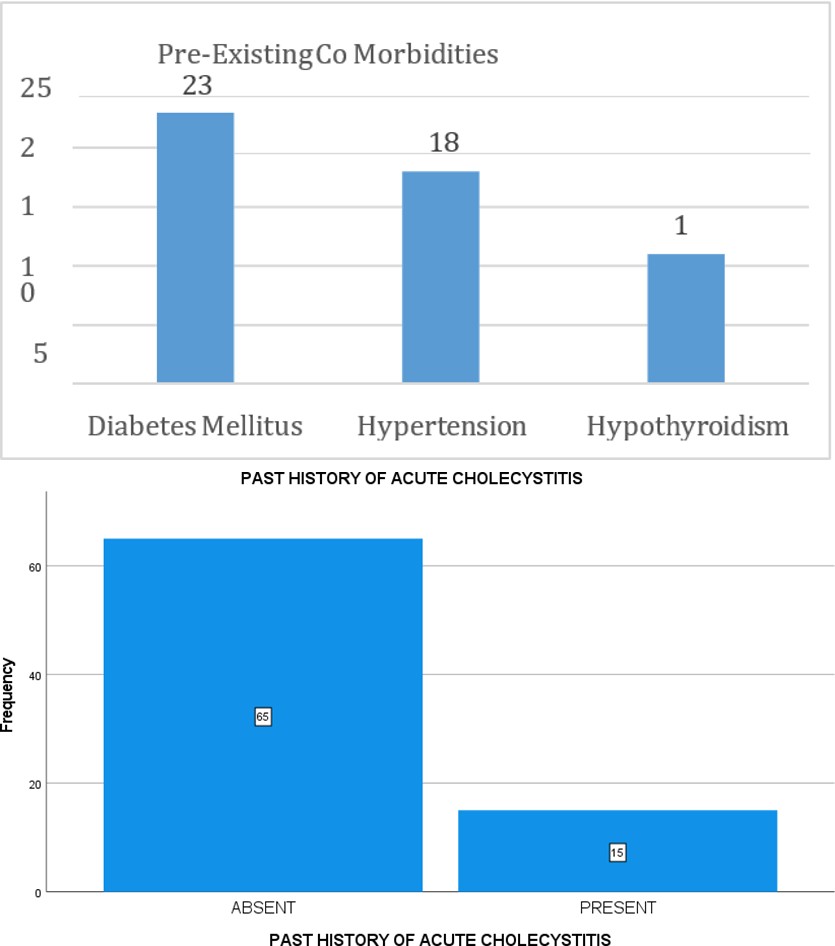
Graph 4: Bar Diagram Depicting the Pre-Existing Comorbidities. The pre-existing co morbidities were as follows diabetes mellitus was present in 23 cases (28.40% ) , hypertension
Previous Attacks of Cholecystistis
| Previous Attacks Of Cholecystistis | Frequency | Percent |
|---|---|---|
| Absent | 65 | 81.30% |
| Present | 15 | 18.70% |
Table 5: Previous Attacks of Cholecystistis.
Graph 5: Bar Diagram Showing Previous Attacks of Cholecystistis.
81.3% had previous attacks of cholecystitis in the present study.
The Distribution of Number of Stones on Ultrasound Abdomen
| Frequency | % | |
|---|---|---|
| Multiple Stones | 48 | 60% |
| Single Stone | 12 | 40% |
Table 6: The Distribution of Number of Stones on Ultrasound.
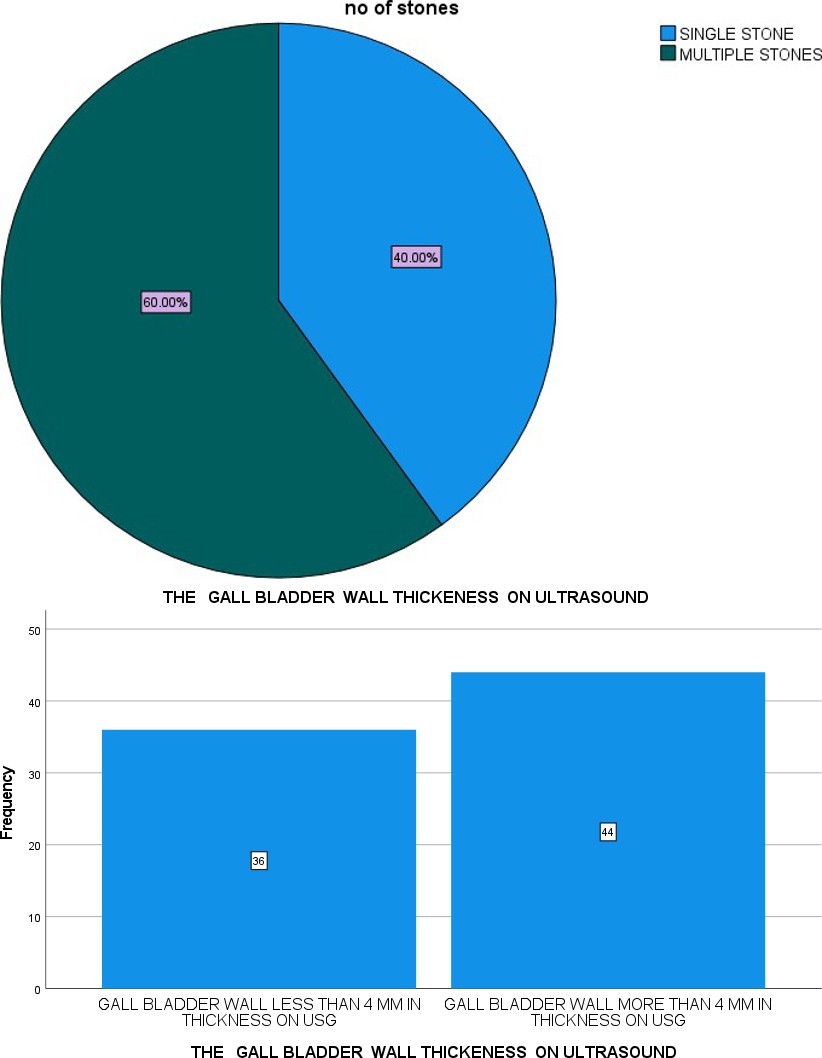
Graph 5: The Distribution of Number of Stones on Ultrasound.
In the present study, 60 % had multiple stones and 40% had single stones.
The Gall Bladder Wall Thickeness on Ultrasound Abdomen
| Frequenc Y | Percentage | |
|---|---|---|
| Gall Bladder Wall >4mm | 44 | 55% |
| Gall Bladder Wall Thickening <4mm | 36 | 45% |
Table 7: The Gall Bladder Wall Thickeness on Ultrasound.
Graph 7: The Gall Bladder Wall Thickeness on Ultrasound.
55% had a gall bladder wall thickness more than 4 mm on ultrasound. Pericholecystic Collection on Ultrasound Abdomen
| Frequency | Percent | |
|---|---|---|
| Pericholecystic collection present | 2 | 2.50% |
| No Pericholecystic collection | 78 | 97.50% |
Table 8: Pericholecystic Collection on Ultrasound.
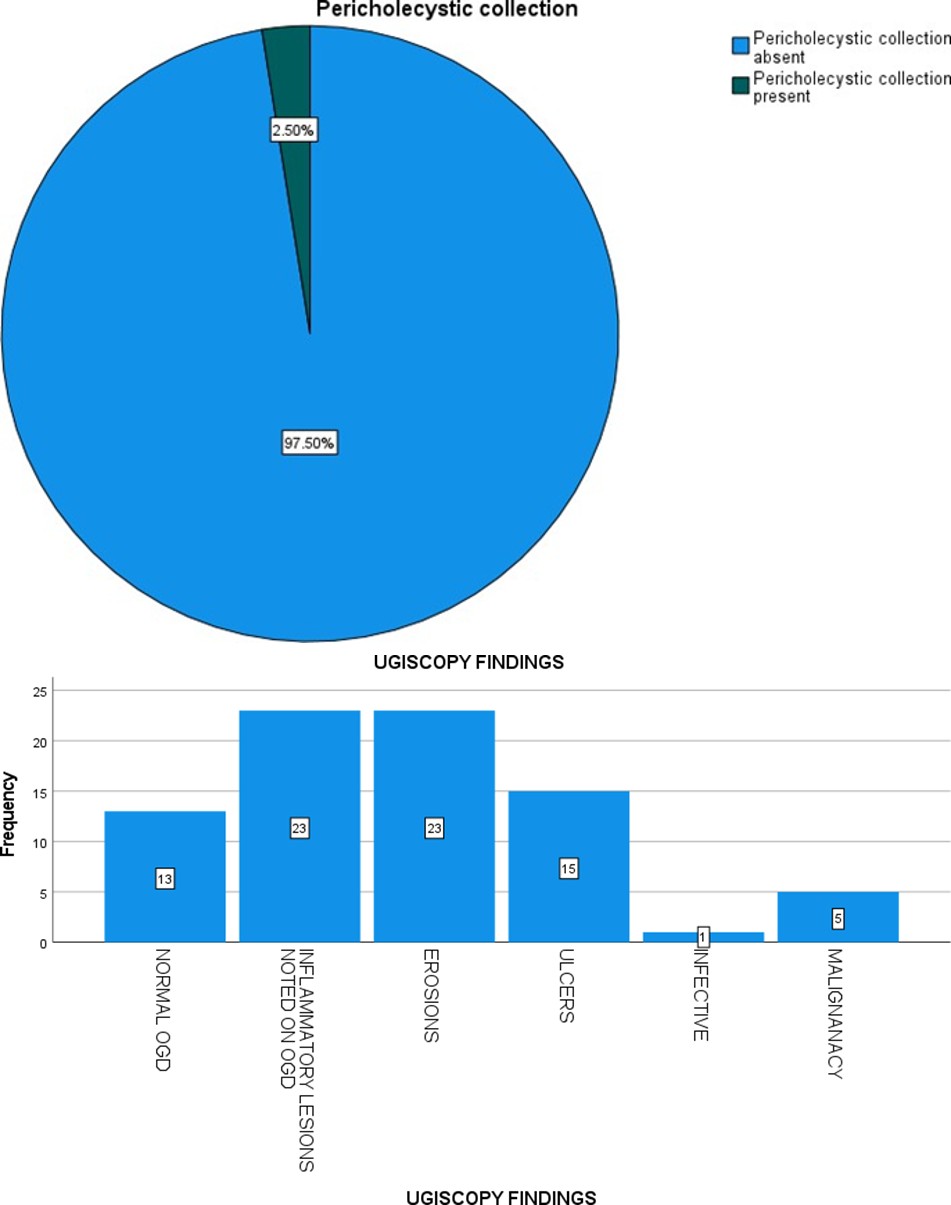
Graph 8: Pericholecystic Collection on Ultrasound.
2.5% had pericholecystic collection on ultrasound.
The Distribution Of Ugie Findings
| Frequency | Percent | |
|---|---|---|
| Normal Ugie | 13 | 16.25% |
| Inflammatory Lesions Noted On Ugie | 23 | 28.75% |
| Erosions | 23 | 28.75% |
| Ulcers | 15 | 18.75% |
| Infective | 1 | 1.25% |
| Malignancy | 5 | 6.25% |
Table 9: Distrbution of Ugie Findings.
Graph 9: Distribution Of UGEI Findings.
In our study, upper GI endoscopy (UGIE) findings were abnormal in 83.75% of patients, while 16.25% had normal findings. The most common pathology was inflammatory lesions (28.75%), followed by erosions (28.75%), ulcers (18.75%), malignancy (6.25%), and infective pathology (1.25%). These results align with previous studies, which have reported a significant prevalence of upper GI pathologies in patients with symptomatic gallstone disease. Our study highlights the importance of identifying and managing coexisting upper GI conditions before proceeding with cholecystectomy.Additionally, Helicobacter pylori infection was detected in 43.48% of inflammatory lesion cases via the rapid urease test (RUT), further reinforcing the role of H. pylori in upper GI inflammation and symptom persistence. Treatment with an eradication regimen led to symptom improvement in these patients. Compared to prior research, our findings demonstrate that gastritis and erosions (56.5%) are the most frequent UGIE abnormalities in symptomatic cholelithiasis patients, followed by peptic ulcers and malignancies (25%). This emphasizes the need for preoperative UGIE in gallstone patients presenting with upper abdominal symptoms to ensure optimal management and avoid unnecessary surgeries.
Rapid Urease Test
| Frequency | Percent | |
|---|---|---|
| H Pylori Present | 10 | 43.48% |
| H Pylori Absent | 13 | 56.52% |
Table 10: Rapid Urease Test.

Graph 10: Rapid Urease Test.
In the present study we had 23 inflammatory lesion in which rapid urease test was done of which 10 cases (43.48%) were positive for H Pylori infection.
Out of 80 patients evaluated with upper GI endoscopy prior to laparoscopic cholecystectomy, 61 patients proceeded with surgery. Among the remaining 19 patients, the following findings were noted:
- 13 patients tested positive for Rapid Urease Test (RUT) for Helicobacter pylori.
- 5 patients were diagnosed with malignancy (esophageal or gastric cancer).
- 1 patient had severe GERD with LA - D esophagitis and a recent history of upper GI bleeding.
These findings highlight the importance of preoperative upper GI evaluation in optimizing patient selection for laparoscopic cholecystectomy.
Discussion
| Supreeth Kumar Reddy Kunnuru, et al. (17) | Present study | |
|---|---|---|
| 18-30 years | 96 (24%) | 10% (8) |
| 31-40 years | 80 (20%) | 18.75%(15) |
| 41-50 years | 60 (15%) | 26.25%(21) |
| 51-60 years | 100 (25%) | 22.50%(18) |
| 61-70 years | 40 (10%) | 15.00%(12) |
| more than 70 years | 24 (6%) | 7.50%(6) |
Table 11: Gall Stones were Common After 40 Years of Age Similar to the Presents Today.
Supreeth Kumar Reddy Kunnuru, et al. [17] noted that gall stones were common after 40 years of age similar to the presents today. In the present 61% were above the age of 40 years which is similar to the study by Supreeth Kumar Reddy Kunnuru et al 17 56% were above the age of 40 years . As compared, the commonest age group in the study had 21 cases (26.25%) belonged to the age group between41 years and 50 years., As compared to he study by Supreeth Kumar Reddy Kunnuru et al 17 51-60 years the commonest age group.
Gender Comparison with Other Studies
Supreeth Kumar Reddy Kunnuru et al 17 noted that 69% were females and 31% were male patients. which is similar to the present study. we also had females more than females. In Kim et al.’s study, the female to male ratio was 1.4 : 19 . A Novacek also noted that gallstones are common in females by 2-3 than males. 45% were females and 55% were males , the male to female ratio was 0.85 to 1 .The difference in gender was statistically significant with the P value 0.032.
The Distribution of Clinical Presentation
In the order of frequency of symptoms abdominal pain was seen in 80 cases (100.00%) , dyspepsia was seen 45 cases (56.25%) , abdominal bloating was seen 27 cases (33.75%), nausea was seen 17 cases (21.25%) , vomiting was seen 4 cases (25%).
According to Fitzgerald et al., upper abdominal pain, dyspepsia, and nausea and vomiting are the common symptoms of gallstone disease11. In our study, pain abdomen was the commonest symptomatology (99% of patients) followed by heart burn (25.5%) and dyspepsia (23%). We got upper GI endoscopy positive findings in 75.5% of our total patients. Only 24.5% of patients presented with normal UGIE. It means 3/4th of cholelithiasis patients were associated with other gastroduodenal problems. In Ayuo et al.’s study 12; common findings in upper GI endoscopy were gastric ulcer (3.1%), duodenal ulcer (11%), gastritis (8.4%), duodenitis (5%), and reflux esophagitis (7.9%).
In our study, gastritis (22%), gastric erosion (19%), reflux esophagitis (12%), lax lower end of esophagus (10%), and gastric and duodenal ulcer (7%) were comparable to the above study. 13(16.25%) cases had a normal UGIE , 23(28.75%) cases had inflammatory lesions noted on UGIE 23(28.75%) cases had erosions , 15(18.75%) cases had ulcers , 1(1.25%) cases had a infective etiology , and 5(6.25%) cases had malignancy.
| Gastritis | Gastric erosion | H.pylori positive | Gastric and duodenal ulcer | Esophagitis | Lax LE |
|---|---|---|---|---|---|
| 90 | 76 | 54 | 30 | 49 | 40 |
| 22% | 19% | 13% | 7% | 12% | 10% |
Table 12: In the Present Study we Had 23 Inflammatory Lesion in which Rapid Urease Test was Done of which 10 Cases (43.48%) were P
Summary
This prospective study was conducted at a tertiary care medical college hospital in Mangalore, Karnataka, India. A total of 80 patients diagnosed with gallbladder stones via ultrasound underwent upper GI endoscopy to assess the correlation between upper GI pathology and gallstone disease.
The study found a higher prevalence of gallstones in females compared to males, with a female-to-male ratio of 1:0.45. Gallstones were more common in patients over 40 years of age, with the majority of affected females being around 60 years old. A subset of patients with inflammatory pathology on upper GI endoscopy tested positive for Helicobacter pylori using the rapid urease test. These patients showed symptomatic improvement after receiving an H. pylori eradication regimen.
Additionally, upper GI endoscopic abnormalities were more frequently observed in patients with single gallstones compared to those with multiple gallbladder calculi. Patients with normal upper GI endoscopic findings also had normal gallbladder wall thickness. Several studies have reported a strong association between gallbladder disease and upper GI pathology. A study by Diettrich et al. found that nearly 40% of patients with gallstones had concurrent upper GI conditions, including gastritis, reflux esophagitis, and peptic ulcer disease, which often contributed to persistent symptoms post-cholecystectomy. Similarly, Csendes et al. reported that H. pylori infection was prevalent in gallstone patients and that eradication therapy significantly improved their symptoms, reinforcing the role of upper GI pathology in symptom persistence.
Other studies have also highlighted that patients with single gallstones are more likely to exhibit upper GI abnormalities compared to those with multiple calculi. Moreover, research has indicated that patients with normal upper GI endoscopic findings tend to have normal gallbladder wall thickness, suggesting that inflammation in the upper GI tract might influence gallbladder pathology. Given these findings, preoperative upper GI evaluation in gallstone patients is crucial, as addressing underlying gastrointestinal conditions may reduce unnecessary cholecystectomies and improve patient outcomes.
Conclusion
The findings of this study underscore the critical role of gastrointestinal evaluation, particularly upper gastrointestinal endoscopy (UGE), in the management of patients with gallstone disease.
- A significant proportion of patients experiencing pain have underlying gastrointestinal inflammatory pathology rather than gallstones as the primary cause. Hence, it is advisable to first diagnose and treat any existing gastrointestinal disease and subsequently reassess symptoms.
- Laparoscopic cholecystectomy should be deferred until gastrointestinal inflammatory conditions are appropriately managed. If symptoms resolve following treatment, patients may be placed under observation rather than undergoing surgery.
Supporting Evidence
- Gallstones frequently remain asymptomatic, and their detection has increased due to the widespread use of advanced imaging modalities.
- Upper gastrointestinal symptoms are often mistakenly attributed to gallstones when, in reality, they may result from other pathologies such as gastritis, peptic ulcer disease, or Helicobacter pylori infection, which share similar clinical presentations.
- A thorough gastrointestinal evaluation should be conducted before diagnosing gallstones as the definitive cause of symptoms and proceeding with surgical intervention.
Given the potential for misattribution of symptoms, this study reinforces the need for a comprehensive, evidence- based approach to gallstone disease management, ensuring that unnecessary cholecystectomies are avoided, and patient outcomes are optimized.
Recommendations
Our study observed that a subset of patients with inflammatory pathology on upper gastrointestinal endoscopy (UGE) tested positive for Helicobacter pylori (H. pylori) using the rapid urease test. Previous research has also suggested a potential association between gallstones and H. pylori infection. Therefore, further studies are warranted to explore whether H. pylori colonization in the gallbladder mucosa plays a role in the pathogenesis of gallstone disease.
Based on our findings and existing literature, we propose the following recommendations
Routine Upper GI Endoscopy Prior to Cholecystectomy: Given that many patients with gallstones have concurrent upper gastrointestinal pathology, a preoperative UGE should be considered, particularly in those presenting with dyspeptic symptoms.
Identifying and treating conditions such as gastritis, peptic ulcer disease, or H. pylori infection may help alleviate symptoms without the need for surgery.
Targeted H. pylori Screening and Eradication: Studies have suggested a correlation between H. pylori and gallstone disease. Screening for H. pylori, particularly in patients with persistent dyspeptic symptoms, may be beneficial. If detected, eradication therapy could be considered as part of the treatment plan.
Deferring Cholecystectomy in Patients with Upper GI Inflammatory Conditions: In patients diagnosed with both gallstones and upper gastrointestinal pathology, medical management should be prioritized. Laparoscopic cholecystectomy should only be performed if symptoms persist following adequate treatment of the gastrointestinal condition.
Long-Term Follow-Up for Non-Operative Management: Patients with asymptomatic gallstones or those who improve after medical therapy should be placed under long-term surveillance. Regular follow-ups with clinical assessment and imaging can help monitor disease progression and guide further management.
Further Research on the Role of H. pylori in Gallstone Formation: More extensive studies, including histopathological and microbiological analyses of gallbladder mucosa, are needed to establish whether H. pylori plays a direct role in gallstone formation and symptomatology. Investigating the impact of H. pylori eradication on gallstone disease progression could provide valuable insights into future management strategies.
Improved Diagnostic Criteria for Symptomatic Gallstones: Current diagnostic protocols should incorporate a more comprehensive approach, distinguishing between pain due to gallstones and symptoms arising from gastrointestinal pathology. Developing clear guidelines for differentiating true biliary colic from other dyspeptic conditions could help reduce unnecessary surgeries.
These recommendations aim to refine the clinical approach to gallstone disease, minimizing unnecessary surgical interventions while ensuring optimal patient outcomes.
A prospective multicenter observational cohort study should be designed to validate these findings by enrolling a large, diverse group of symptomatic cholelithiasis patients scheduled for cholecystectomy across various tertiary care centers. A standardized UGIE protocol would be implemented to uniformly categorize findings (normal, inflammatory, erosions, ulcers, infective, malignancy), with detailed preoperative assessments and postoperative follow-ups at defined intervals (e.g., 1, 3, and 6 months) to monitor symptom resolution. A robust sample size (e.g., >500 patients) and multivariate statistical analyses (e.g., logistic regression, Kaplan-Meier curves) would ensure sufficient power to correlate UGIE findings with persistent symptoms and evaluate the impact of targeted treatments such as H. pylori eradication. Inter-center calibration and centralized data monitoring would further ensure data consistency, with the collaborative results ultimately guiding clinical guidelines for the routine preoperative evaluation of gallstone disease. Data consistency would be further guaranteed by inter-center calibration and centralized data monitoring, and the joint findings would eventually inform clinical recommendations for the standard preoperative assessment of gallstone disease.
Author Contributions
Collection and/or Assembly of Data
Anand Bhandary Panambur, Rahul Shenoy.
Manuscript Writing and Approval
Anand Bhandary Panambur, Anand Peter Ignatius.
Conflict of Interest Statement
The authors have no conflicts of interest to declare.
Funding Sources
The authors did not receive any funding. References
1. Dey S, Chatterjee S, Ghosh S, Sikdar N (2016) The geographical, ethnic variations and risk factors of gallbladder carcinoma: a worldwide view. J Investig Genomics 3(3): 00051.
2. Weerakoon H, Vithanage I, Alahakoon O, Weerakoon K (2022) Clinico-epidemiology and aetiopathogenesis of gallstone disease in the South Asian region: a scoping review protocol. BMJ open 12(6): e057808.
3. Mansoor S, Effan F, Ibnerasa SH, Butt SE, Rathore SA (2007) Morphological Spectrum of Gallbladder Disease: a retrospective study in a private medical college in Lahore. Pak J Med Sci 11(4): 1505-1058.
4. Jayasundara JA, de Silva WM (2013) Histological assessment of cholecystectomy specimens performed for symptomatic cholelithiasis: routine or selective?. The Annals of The Royal College of Surgeons of England 95(5): 317-322.
5. Aerts R, Penninckx F (2003) The burden of gallstone disease in Europe. Alimentary pharmacology & therapeutics 18: 49-53.
6. Stinton LM, Shaffer EA (2012) Epidemiology of gallbladder disease: cholelithiasis and cancer. Gut and liver 6(2): 172.
7. Mi N, Liang Z, Yang M, Zhao J, Tian L, et al. (2024) Genetic risk, adherence to healthy lifestyle behaviors, and risk of cholelithiasis: A population-based cohort study. Preventive Medicine 107942.
8. Li S, Guizzetti L, Ma C, Shaheen AA, Dixon E, et al. (2023) Epidemiology and outcomes of symptomatic cholelithiasis and cholecystitis in the USA: trends and urban– rural Variations. Journal of Gastrointestinal Surgery 27(5): 932-944.
9. Wakabayashi G, Iwashita Y, Hibi T, Takada T, Strasberg SM, et al. (2018) Tokyo Guidelines 2018: surgical management of acute cholecystitis: safe steps in laparoscopic cholecystectomy for acute cholecystitis (with videos). Journal of Hepato‐biliary‐pancreatic Sciences 25(1): 73-86.
10. Thunnissen FM, Baars C, Arts R, Latenstein CS, Drenth
JP, et al. (2023) Persistent and new-onset symptoms after cholecystectomy in patients with uncomplicated symptomatic cholecystolithiasis: A post hoc analysis of 2 prospective clinical trials. Surgery 174(4): 781-786.
11. Shabanzadeh DM (2023) The Symptomatic Outcomes
of Cholecystectomy for Gallstones. Journal of Clinical Medicine 12(5): 1897.
12. Lee H, Askar A, Makanji D, Ranjha K, Karki BB, Courcol J,
et al. (2024) The incidence of post cholecystectomy pain (PCP) syndrome at 12 months following laparoscopic cholecystectomy: a prospective evaluation in 200 patients. Scandinavian Journal of Pain 24(1): 20230067.
13. Hayden P, Cowman S (2011) Anaesthesia for laparoscopic surgery. Continuing Education in Anaesthesia, Critical
Care & Pain 11(5): 177-180.
14. Bruhat MA, Chapron C, Mage G, Pouly JL, Canis M, et al.
(1993) The benefits and risks of laparoscopic surgery. Revue francaise de gynecologie et d’obstetrique 88(2): 84-88.
15. Reitano E, De’Angelis N, Schembari E, Carrà MC,
Francone E, et al. (2021) Learning curve for laparoscopic cholecystectomy has not been defined: a systematic review. ANZ Journal of Surgery 91(9): E554-E560.
16. De Bortoli N, Tolone S, Frazzoni M, Martinucci I, Sgherri
G, et al. Gastroesophageal reflux disease.
17. Kunnuru SKR, Kanmaniyan B, Thiyagarajan M, Singh
BK, Navrathan N (2021) A Study on Efficacy of UGI Scopy in Cholelithiasis Patients before Laparoscopic Cholecystectomy. Minim Invasive Surg 2021: 8849032.
18. Ayuo PO, Some FF, Kiplagat J (2014) Upper gastrointestinal endoscopy findings in patient referred with upper gastrointestinal symptoms in Eldoret, Kenya: a retrospective review. East African Medical Journal 91(8).
19. Fitzgerald JE, Fitzgerald LA, Maxwell-Armstrong CA,
Brooks AJ (2009) Recurrent gallstone ileus: time to change our surgery? Journal of Digestive Diseases 10(2): 149-151.
20. Kim SB, Kim KH, Kim TN (2017) Sex differences in prevalence and risk factors of asymptomatic cholelithiasis in Korean health screening examinee: a retrospective analysis of a multicenter study. Medicine (Baltimore) 96(13): e6477.
21. Rashid F (2010) Role of routine oesophago- gastroduodenoscopy before cholecystectomy. International Journal of Surgery 8(3).
22. Frierson HF (1989) The gross anatomy and histology of the gallbladder, extrahepatic bile ducts, Vaterian system, and minor papilla. The American journal of surgical pathology. 13(2): 146-162.
23. Toouli J, Bhandari M (2006) Anatomy and physiology of the biliary tree and gallbladder. Diseases of the Gallbladder and Bile Ducts Diagnosis and Treatment, Second Edition. Massachusetts: Blackwell Publishing pp: 3-21.
24. Song ST, Shi J, Wang XH, Guo YB, Hu PF, et al. (2020)
Prevalence and risk factors for gallstone disease: A population‐based cross‐sectional study. Journal of digestive diseases 21(4): 237-245.
25. Dachman AH, Schneck C (2018) Embryology of the gallbladder. InImaging Atlas. CRC Press 18: 13-20.
26. Saldinger PF, Bellorin-Marin OE (2019) Anatomy,
Embryology, Anomalies, and Physiology of the Biliary Tract. InShackelford’s Surgery of the Alimentary Tract 2: 1249-1266.
27. Hull NC, Schooler GR, Lee EY (2020) Bile Duct and Gallbladder. InPediatric Body MRI. Springer Cham 1: 235-253.
28. Abdalla S, Pierre S, Ellis H (2013) Calot’s triangle. Clinical
anatomy 26(4): 493-501.
29. Suzuki M, Akaishi S, Rikiyama T, Naitoh T, Rahman MM,
et al. (2000) Laparoscopic cholecystectomy, Calot’s triangle, and variations in cystic arterial supply. Surgical endoscopy. 14(2): 141-144.
30. Song ST, Shi J, Wang XH, Guo YB, Hu PF, et al. (2020)
Prevalence and risk factors for gallstone disease: A population‐based cross‐sectional study. Journal of digestive diseases 21(4): 237-245.
31. Diettrich H, Wundrich B, Kobe E, Noack S, Weber K (1990)
Gastroscopy before cholecystectomy. Gastroenterol J 50(4): 173-174.
- Ramsay Hunt Syndrome Presenting as Gait Imbalance without Facial Paralysis: A Case Report
- Assessing Health Care Providers’ Proficiency in International Patient Safety Goals: A Study to Assess the Knowledge &Practice on Patient Safety in a Tertiary Care Teaching Hospital in Gujarat
- Challenges in Diagnosing Child Language Disorders
- Stunting Service Management Model in the South-Central Timor Region, East Nusa Tenggara, Indonesia
- Acute Small Bowel Obstruction Presenting as Gangrenous Jejunal Loop Secondary to Intestinal Endometriosis – A Rare Case Report
- A Single-Center, Prospective Study Focused on Quality Indicators, Success Rate, Features, Outcomes, and Indications of Endoscopic Retrograde Cholangiopancreatography (ECRP) Practice at a Tertiary Care Hospital