Fever Unmasking Brugada‐Like Electrocardiographic Pattern Induced by Fever: ICD or NOT?
We report a case report of 71-year-old man was admitted for syncope during a febrile state. The electrocardiogram revealed a right bundle branch block and pattern of elevated ST segment in the anterior leads similar to the Brugada syndrome. These electrocardiographic anomalies disappeared when the temperature returned to normal. An electrophysiological study using aggressive protocol did not triggered ventricular arrythmia. An automatic defibrillator (ICD) was proposed due to the highrisk arrhythmic events but refused by the patient to get implanted.
Abbreviations
PES: Programmed Electrical Stimulation; ICD: Implantable Cardioverter-Defibrillator; ILR: Implantable Loop Recorder.
Introduction
Described for the first time in 1992 Brugada P, et al. [1], Brugada syndrome is a rare inherited disorder predisposing to malignant ventricular arrhythmias and the high risk of sudden death. Despite its autosomal dominant transmission [2], there is a clear male predominance [3]. The diagnosis is based on specific electrocardiographic features [4, 5], without signs of structural heart disease. The implantation of a defibrillator is the only treatment proven to be effective in preventing sudden death in symptomatic individuals with malignant ventricular arrhythmias.
It is recognized as a condition affecting young adults, typically in their 30s and 40s [6, 7], although diagnosis at an older age is not uncommon. Risk stratification for asymptomatic or older individuals is not always straightforward.
The decision to implant a defibrillator should consider the benefits of the ICD and the risk of complications [8], especially in frail elderly patients. Our case illustrates the challenges in diagnosing and managing brugada syndrome in senior patients.
Case Report
We report the case of a 71-year-old male patient with cardiovascular risk factors including hypertension and smoking, with no prior history of cardiac arrest ressuscited. His family history was negative for atherosclerotic cardiovascular events or sudden cardiac death at early age.
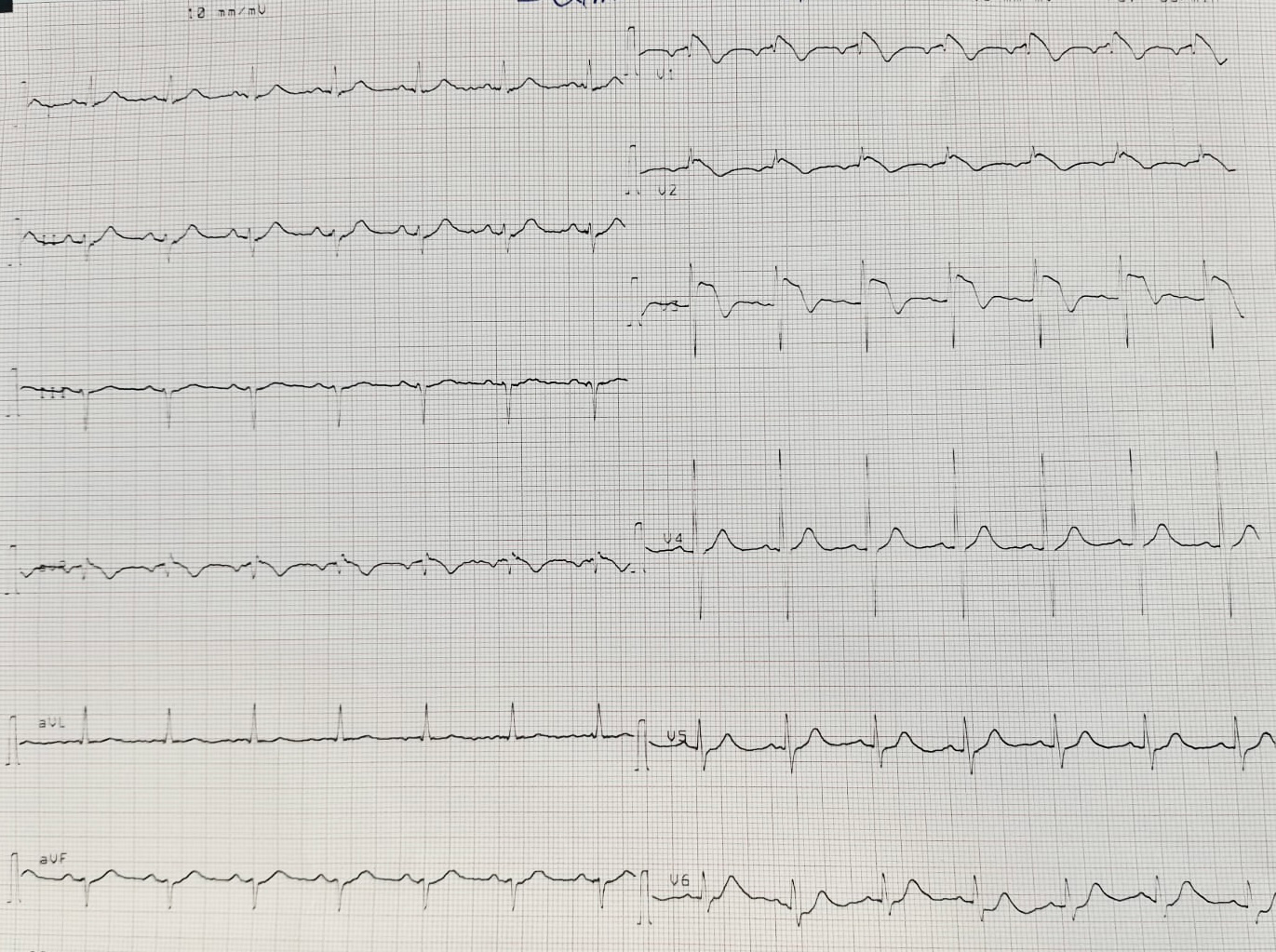
Given the patient’s age and cardiovascular risk factors, syncope raises concerns of ventricular arrythmia on ischemic heart disease, or conduction disorders. An ECG taken on admission (Figure 1) shows regular sinus rhythm, deviated heart axis to the left, normal PR interval at 160 ms, incomplete right bundle branch block, and left anterior fascicular block. Additionally, there is ST segment elevation in antero-septal leads V1-V3 followed by inverted T waves.
The patient presented to the emergency department following an episode of syncope with a traumatic fall and head injury, which occurred during his normal daily activities. He denied any presyncopal symptoms, palpitations or shortness of breath. He reported atypical chest pain and a previous episode of near-fainting 2 years ago, for which he did not seek medical attention, and he has been experiencing fever, cough, and purulent sputum for the past 48 hours.
Clinical examination upon admission finds a febrile patient at 40 degrees Celsius, hemodynamically stable. Heart sounds were well perceived at a regular rhythm without any murmurs or added noises. There were no signs of heart failure. An ecchymosis above the orbital area was noted as a result of the fall.
On echocardiography, He had no structural heart disease, no wall motion abnormalities and no pericardial effusion.
After biological sampling, the patient was promptly admitted to catheterization laboratory, the coronary angiography revealed stenosis of 50% of the right coronary artery.
Biological assessment showed negative troponin, no electrolyte disorders or acidosis, but positive markers of inflammation. The chest X-ray showed a right lower lobe pneumonia.
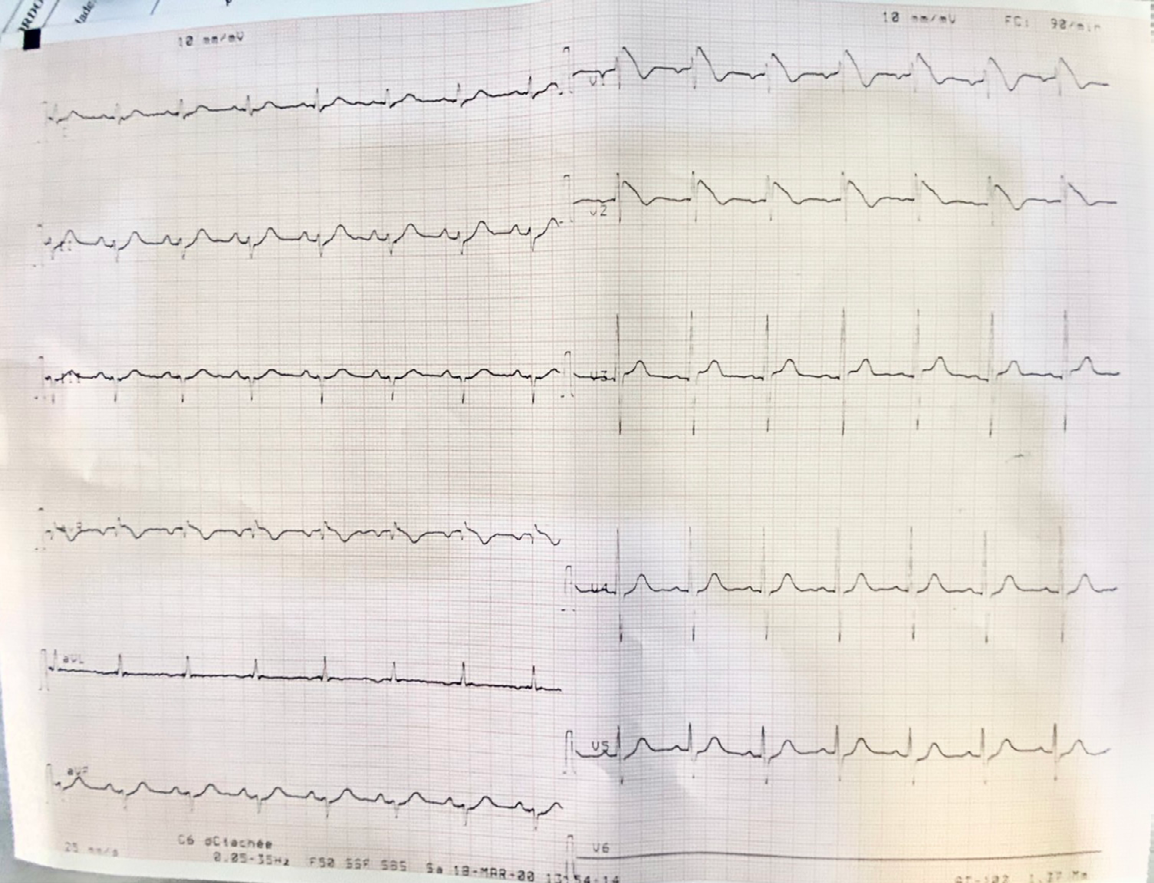
An ECG was repeated 24 hours later (Figure 2), by another medical staff, with leads V1 and V2 placed in the second intercostal space, showing the same electrical aspect in V1-V2 with no typical evolution of ischemia or q wave of necrosis. Note that the patient was still febrile.
The patient was admitted to the intensive care unit for continuous monitoring with a defibrillator nearby, he was put on antibiotics and antipyretics, with repeated ECG. He did not have any arrhythmia during hospital stay.
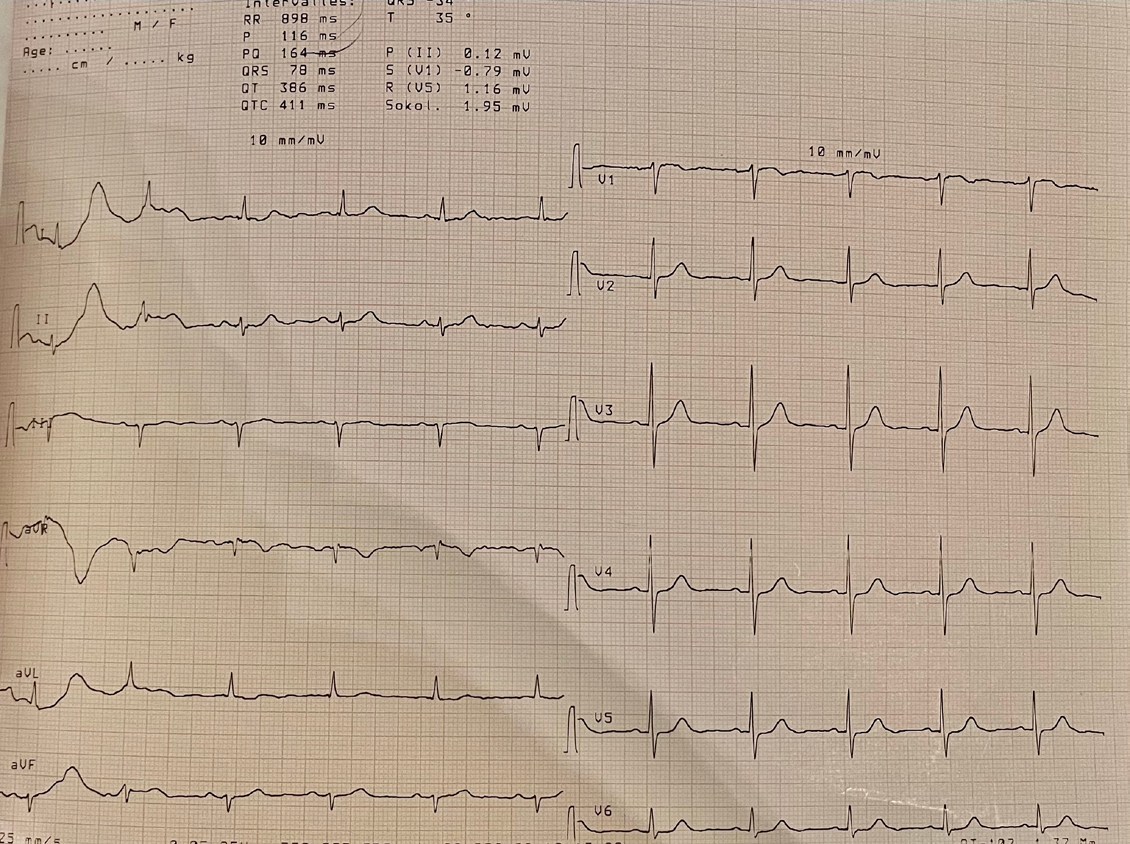
After 24 hours of being afebrile, another ECG was done (Figure 3), and the previous shift had completely regressed with a normalization of the ECG.
Considering the advanced age of our patient, it was deemed necessary to deepen the etiological research to exclude reversible causes of ST-segment elevation. Ischemic heart disease, conduction impairment, and electrolyte disturbance were all ruled out. No pulmonary embolism or mechanical mediastinal compression was found on thoracic CT scan, no pericarditis was observed. Cardiac MRI didn’t reveal any signs of arrhythmic right ventricular dysplasia or other structural heart disease.
To document any arrhythmia that may be responsible for syncope, the patient underwent a 48-hour Holter monitoring, it did not show any ventricular or supraventricular tachycardia, but there was PVCs with precordial transition which favor RVOT region.
Our patient exhibits a fever induced Type 1 brugada pattern with symptoms including syncope. Taking into account the results of all the tests, we have considered the diagnosis of brugada syndrome. The challenge was how to manage our patient with the optimal balance of benefice and risks, either to propose an implantable cardioverter- defibrillator (ICD) to confer full protection sense patients with syncope are at high-risk arrhythmic events, or implantable loop recorder (ILR) to document a ventricular arrhythmia with high risk of sudden death if the patient does not seek medical attention in time.
Our patient, refuses to get implanted with an ICD, and he didn’t afford to get an ILR, he was discharged with recommendation for regular check-up in cardiology center. He did not relapse; however, he did not present with fever.
He was made aware that his first-relatives should seek evaluation for BrS, to avoid drugs with sodium channel blocking activity, treatment of fever and the emergency for monitoring during episodes of fever, and about the warning signs: recurrence of syncope, palpitations.
Discussion
Brugada syndrome recognized as a condition affecting young adults, typically in their 30s and 40s [6, 7], although diagnosis at an older age is not uncommon. Risk stratification for asymptomatic or older individuals is not always straightforward.
The decision to implant a defibrillator should consider the benefits of the ICD and the risk of complications [8], especially in frail elderly patients. Our case illustrates the challenges in diagnosing and managing brugada syndrome in senior patients [9]. Described as an ST segment aberration in the right leads, either spontaneously or under sodium channel blocking drugs, Brugada syndrome is associated with a high risk of sudden death, accounting for 4-12% of all sudden cardiac deaths and 20% in individuals without structural heart disease [10, 11]. Average age at the diagnosis is ranging between 38 and 48 years [12].
Brugada type 1 is described, in at least one right precordial lead V1 or V2, placed at the 2nd, 3rd, or 4th intercostal space, as a J point elevation of 0.2 mV, with a coved ST elevation and T wave inversion [13].
Reported in 2-4% of the healthy population [14], this drug or fever induced electrographic pattern lacks specificity, thus it seems mandatory to exclude other acute and chronic underlying disorders that could mimicked type 1 pattern. These conditions are collectively referred to as Brugada syndrome phenocopies.
They are often reversible and characterized by a type 1 or 2 Brugada pattern in leads V1-V3. Four criteria for diagnosing of Brugada phenocopies were established by Ansalem and Baranchuk [15], based on a Brugada-like ECG pattern, a low probability of Brugada syndrome considering symptoms, personal and family history, and provocation test results (23-36% false-negative risk with flecainide compared to ajmaline [16, 17, 18]. A genetic test, is not mandatory, as it is positive in only 11-28% of patients [19].
A negative INa-block test does not [9], however, rule out a latent type of BrS (for example, the negative predictive value of the flecainide test is 36%).
Fever, a classic trigger of VF in Brugada syndrome, can unmask sodium channel dysfunctions due to the mutation. These channels are considered temperature-sensitive, but the pathophysiological mechanism by which fever unmasks the Brugada pattern remains poorly understood. A meta- analysis [20] showed that fever-induced Brugada pattern is a benign asymptomatic condition that does not require an ICD insertion, unlike Brugada syndrome.
In the presence of symptoms, notably syncope, it is necessary to distinguish if it is due to an arrhythmic origin or not. Detailed medical history, absence of prodromes, or specific triggers are of great help. But in 30% of cases, the etiology remains undetermined.
For risk stratification, the Brugada brothers [6] suggested that the induction of VT/VF in PES predicts severe arrhythmic events. On the other hand, the PRELUDE registry [7] showed that inducibility was not predictive of arrhythmic events during follow-up. According to this registry, syncope, a spontaneous type 1, a ventricular refractory period < 200ms, and fragmented QRS were predictors of ventricular arrhythmias.
Unexplained syncope in patients with spontaneous or induced type 1 justifies an implantable loop recorder [21], which helps optimizing patient management at the cost of a delayed defibrillator implantation. Paroxysmal AV block episodes and vagally mediated bradycardia were the most common causes of symptoms.
Several studies and case series Kitamura T, et al. [22] have focused on Brugada syndrome in the elderly. They showed that the incidence of VF decreases with age, that the first rhythmic event after 70 years is exceptional, and that VF recurrence after 50-70 years in ICD carriers is rare in the absence of underlying ischemic heart disease. All these studies showed that Brugada syndrome in the elderly has a good prognosis [22, 23], especially in the absence of VF under 70 years.
It should be noted that 1/3 of patients with Brugada syndrome present with unexplained syncope, and that the risk of arrhythmic events in these patients is four times higher [24] than in asymptomatic patients. Moreover, In relation to the condition, increased sinus node recovery time and sino-atrial conduction time [15] together with delayed atrial conduction and atrial standstill have been described [16]. The development of supraventricular arrhythmias is strongly linked with ventricular inducibility.
Among the Brugada syndrome patients with an indication for an implantable cardioverter-defibrillator (ICD) 27% exhibit supraventricular arrhythmias, compared to 13% of patients without an ICD indication, suggesting a more severe disease course in patients with spontaneous atrial arrhythmias [17].
As patients are getting age Postema PG, et al. [25], they are likely to develop ischemic heart disease, atrial fibrillation, and other comorbidities requiring the introduction of numerous medications. Some of these medications have been reported to induce the Type 1 pattern, thereby exposing patients to the risk of fatal arrhythmias. These medications include flecainide, amiodarone, verapamil (with case reports of type 1 pattern under these medications), and diuretics (due to electrolyte disturbances causing type 1 and proarrhythmic effects). Ivabradine has been proposed as a substitute for beta-blockers in the treatment of atrial fibrillation in patients with Brugada syndrome.
In managing our patient, we faced many challenges. The diagnosis of Brugada syndrome remains challenging as the ECG changes are dynamic and often hidden [26]. The prognosis for patients with unexplained syncope is less well- defined, with the risk of recurrence up to 53% in patients with Brugada syndrome. Clinical and ECG characteristics underlying prognostic factors between senior and younger patients and between Brugada syndrome and fever-induced Brugada pattern are not clarified. Moreover, the indication for ICDs in senior patients, according to the latest guidelines, has not been verified.
Conclusion
Diagnosis of brugada syndrome in the elderly is always unexpected. It should be emphasized that clinical presentation is the most important parameter in risk stratification of patients with brugada ECG. ICD implantation of senior brugada patients should be carefully evaluated Considering the increasing risk of inappropriate shocks because of the relatively late onset of SVT and lead failures, and the low risk of new onset of VA after 65-70 years.
Declarations
Ethical Approval
Not applicable
Consent to Participate
Not applicable
Consent for Publication
The authors declare that informed consent was obtained for the usage of de-identified images and relevant investigations of the patient.
Funding
No fundings
Competing Interests
Not applicable
References
-
Brugada P, Brugada J (1992) Right bundle branch block, persistent ST segment elevation and sudden cardiac death: a distinct clinical and electrocardiographic syndrome. A multicenter report. J Am Coll Cardiol 20(6): 1391‑1396.
-
Juang JM, Huang SKS (2004) Brugada syndrome--an under-recognized electrical disease in patients with sudden cardiac death. Cardiology 101(4): 157‑169.
-
Antzelevitch C (2003) Androgens and male predominance of the Brugada syndrome phenotype. Pacing Clin Electrophysiol PACE. Juill 26(7Pt1): 1429‑31.
-
Antzelevitch C, Yan GX, Ackerman MJ, Borggrefe M, Corrado D, et al. (2017) J-Wave syndromes expert consensus conference report: Emerging concepts and gaps in knowledge. Europace 19(4): 665‑694.
-
Behr ER, Ben-Haim Y, Ackerman MJ, Krahn AD, Wilde AAM (2021) Brugada syndrome and reduced right ventricular outflow tract conduction reserve: a final common pathway? Eur Heart J 42(11): 1073‑1081.
-
Brugada J, Brugada R, Brugada P (2003) Determinants of Sudden Cardiac Death in Individuals With the Electrocardiographic Pattern of Brugada Syndrome and No Previous Cardiac Arrest. Circulation 108(25): 3092‑3096.
-
Priori SG, Napolitano C, Gasparini M, Pappone C, Della Bella P, et al. (2002) Natural history of Brugada syndrome: insights for risk stratification and management. Circulation 105(11): 1342‑1347.
-
Sherrid MV, Daubert JP (2008) Risks and challenges of implantable cardioverter-defibrillators in young adults. Prog Cardiovasc Dis 51(3): 237‑263.
-
Popa IP, Șerban DN, Mărănducă MA, Șerban IL, Tamba BI, et al. (2023) Brugada Syndrome: From Molecular Mechanisms and Genetics to Risk Stratification. Int J Mol Sci 24(4): 3328.
-
Khan A, Mittal S, Sherrid MV (2009) Current review of Brugada syndrome: from epidemiology to treatment. Anadolu Kardiyol Derg AKD Anatol J Cardiol. 9(S2): 12‑6.
-
Antzelevitch C (2006) Brugada syndrome. Pacing Clin Electrophysiol PAC 29(10): 1130‑1159.
-
Milman A, Andorin A, Gourraud JB, Sacher F, Mabo P, et al. (2017) Age of First Arrhythmic Event in Brugada Syndrome: Data From the SABRUS (Survey on Arrhythmic Events in Brugada Syndrome) in 678 Patients. Circ Arrhythm Electrophysiol 10(12): e005222.
-
Zeppenfeld K, Tfelt-Hansen J, de Riva M, Winkel BG, Behr ER, et al. (2022) 2022 ESC Guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: Developed by the task force for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death of the European Society of Cardiology (ESC) Endorsed by the Association for European Paediatric and Congenital Cardiology (AEPC). Eur Heart J 43(40): 3997‑4126.
-
Adler A, Rosso R, Chorin E, Havakuk O, Antzelevitch C, et al. (2016) Risk stratification in Brugada syndrome: Clinical characteristics, electrocardiographic parameters, and auxiliary testing. Heart Rhythm 13(1): 299‑310.
-
Anselm DD, Evans JM, Baranchuk A (2014) Brugada phenocopy: A new electrocardiogram phenomenon. World J Cardiol 6(3): 81‑86.
-
Wilde AAM, Amin AS, Morita H, Tadros R (2023) Use, misuse, and pitfalls of the drug challenge test in the diagnosis of the Brugada syndrome. Eur Heart J 44(27): 2427‑2439.
-
Wilde AAM, Antzelevitch C, Borggrefe M, Brugada J, Brugada R, et al. (2002) Proposed diagnostic criteria for the Brugada syndrome: consensus report. Circulation 106(19): 2514‑2519.
-
Meregalli PG, Ruijter JM, Hofman N, Bezzina CR, Wilde AAM, et al. (2006) Diagnostic value of flecainide testing in unmasking SCN5A-related Brugada syndrome. J Cardiovasc Electrophysiol 17(8): 857‑864.
-
Chen Q, Kirsch GE, Zhang D, Brugada R, Brugada J, et al. (1998) Genetic basis and molecular mechanism for idiopathic ventricular fibrillation. Nature 392(6673): 293‑296.
-
Roomi SS, Ullah W, Abbas H, Abdullah H, Talib U, et al. (2020) Brugada syndrome unmasked by fever: a comprehensive review of literature. J Community Hosp Intern Med Perspect 10(3): 224‑228.
-
Kubala M, Aissou L, Traulle S, Gugenheim AL, Hermida JS (2012) Use of implantable loop recorders in patients with Brugada syndrome and suspected risk of ventricular arrhythmia. Europace 14(6): 898‑902.
-
Kitamura T, Fukamizu S, Kawamura I, Hojo R, Aoyama Y, et al. (2017) Clinical Characteristics and Long-Term Prognosis of Senior Patients With Brugada Syndrome. JACC Clin Electrophysiol 3(1): 57‑67.
-
Kamakura T, Wada M, Nakajima I, Ishibashi K, Miyamoto K, et al. (2015) Evaluation of the Necessity for Cardioverter-Defibrillator Implantation in Elderly Patients With Brugada Syndrome. Circ Arrhythm Electrophysiol 8(4): 785‑791.
-
Probst V, Veltmann C, Eckardt L, Meregalli PG, Gaita F, et al. (2010) Long-term prognosis of patients diagnosed with Brugada syndrome: Results from the FINGER Brugada Syndrome Registry. Circulation 121(5): 635‑643.
-
Postema PG, Tan HL, Wilde AA (2013) Ageing and Brugada syndrome: considerations and recommendations. J Geriatr Cardiol 10(1): 75-81.
-
Richter S, Sarkozy A, Veltmann C, Chierchia GB, Boussy T, et al. (2009) Variability of the diagnostic ECG pattern in an ICD patient population with Brugada syndrome. J Cardiovasc Electrophysiol 20(1): 69‑75.
- Ramsay Hunt Syndrome Presenting as Gait Imbalance without Facial Paralysis: A Case Report
- Unveiling Hidden Culprits: An Observational Study of Upper Gastrointestinal Endoscopy Findings in Symptomatic Cholelithiasis Patients
- Assessing Health Care Providers’ Proficiency in International Patient Safety Goals: A Study to Assess the Knowledge &Practice on Patient Safety in a Tertiary Care Teaching Hospital in Gujarat
- Challenges in Diagnosing Child Language Disorders
- Stunting Service Management Model in the South-Central Timor Region, East Nusa Tenggara, Indonesia
- Acute Small Bowel Obstruction Presenting as Gangrenous Jejunal Loop Secondary to Intestinal Endometriosis – A Rare Case Report